
Remember me

Bronchopulmonary dysplasia (BPD) remains one of the most common and costly conditions affecting preterm infants,1 with associated significant long-term respiratory and neurodevelopmental morbidity into adulthood.2 Infants with BPD are twice as likely to die or have cognitive and motor delays including cerebral palsy3 with more respiratory tract infections4 and abnormal lung function in adulthood.2 Severe BPD and being discharged on home oxygen are important outcomes for parents who have significant anxiety caring for their child.5 BPD, particularly more severe forms requiring postnatal corticosteroid (PNC) treatment, places a significant burden on paediatric and adult respiratory and intensive care services, as well as the wider education and social services.6
There has been a greater focus on avoiding invasive ventilation to prevent lung injury and cautious PNC use to facilitate extubation and reduce BPD and mortality risk while minimising the potential neurotoxic effects.7 With significant changes in neonatal respiratory management in recent years, there are little contemporary data on changes with BPD severity and respiratory support at discharge. Hence, it is crucial to assess the temporal trends in survival, respiratory care and outcomes in preterm infants as these practices evolve. Furthermore, visualisation of contemporaneous population-based outcome data, including detailed important respiratory outcomes, is crucial in addressing the variation in how clinicians perceive risk and estimate outcomes which impacts on treatment decision making and parental discussion.8
ObjectivesWe aimed to describe the recent changes in neonatal respiratory practices, outcomes and mortality in preterm infants born below 32 weeks gestation across a national health service setting. To support clinical care of these high-risk infants, our secondary aim was to develop an online dashboard depicting the incidence of these important outcomes.
Material and methodsStudy designThis was a population-based retrospective cohort study using deidentified data from the National Neonatal Research Database (NNRD). The study was reported using the Strengthening the Reporting of Observational Studies in Epidemiology guideline.
Data source and patient populationNNRD contains detailed neonatal information entered by healthcare professionals at the point of care.9 A total of 185 neonatal units (online supplemental table 1) contributed to the NNRD covering over 90% of neonatal units in England in 2010, with complete coverage in England from 2012 and Wales from 2014. All preterm infants born below 32 weeks of gestational age (GA) from 2010 to 2020 and admitted to neonatal units in England and Wales contributing to the NNRD were included. Infants who were not admitted for neonatal care were not included, accounting for 9.6% of all live births born below 32 weeks GA as determined from the Office of National Statistics10 during this period, with 68% of these born below 24 weeks GA. Infants with birthweight z scores below −4 or above 4, based on the UK WHO growth chart,11 and discharged to non-participating neonatal units were excluded as they were likely erroneous or incomplete entries.
Definition of clinical practices and outcomesData were extracted for key clinical practices, including antenatal corticosteroids, surfactant and PNC use. The type and definition of PNC analysed were based on a recent UK survey12 to ensure that the PNC was intended to treat or prevent BPD: dexamethasone,13 methylprednisolone14 and budesonide15 (all defined as more than two consecutive days of treatment), and hydrocortisone16 17 (defined as more than six consecutive days of treatment).
Four outcome measures were analysed. First, death before discharge from the neonatal unit. Second, respiratory requirement at discharge in surviving infants. Third, BPD defined as the dependence on any form of respiratory support or oxygen at 36 weeks of corrected GA (CGA). If infants were discharged before 36 weeks CGA, respiratory support at discharge was used. Infants who died before 36 weeks CGA were excluded from this denominator. This definition aligns with recent evidence18 and UK reporting.19 Information on room air challenge test was not recorded. Fourth, severe BPD, defined as requiring non-invasive (including high flow >2 L/min) and invasive pressure support ventilation at 36 weeks CGA, aligning with the Jensen 2019 grade two and three BPD definitions.18 Further definitions of the variables used are described in online supplemental table 2.
AnalysisSummary statistics (median, IQR and percentages) were used to describe the data. Trends in the categorical and continuous data across birth years and respiratory support type at discharge were analysed by using the χ2 test for trend20 and an extension of the Wilcoxon rank-sum test,21 respectively. To account for competing risk when analysing respiratory outcomes across the birth year, the composite outcomes of death and/or respiratory outcomes were used.
All statistical analyses were performed using STATA SE V.17 and complete case analysis, with an assumed significance level of α=0.01 to reduce the type 1 error due to multiple analyses. Multivariable logistic regression was used to obtain the OR of the outcomes across the birth years (modelled as categorical variable with 2010 as the reference group), adjusted for GA at birth, birthweight z score and sex with robust variance estimator accounting for clustering within units. Restricted cubic spline was used to model the continuous variables of GA at birth and birthweight z scores. Population heat maps specific for gestation, sex and birthweight centile11 were devised for the incidence of mortality and respiratory outcomes. These were split into 2010–2015 and 2016–2020 to reflect outcome changes from the last 5 years. An online dashboard was produced using Microsoft Power BI. Infants born below 23 weeks GA were excluded due to small numbers and lack of birthweight centiles.11 Cells with less than 10 infants were suppressed.
ResultsData from 84 440 infants were extracted. A total of 977 (1.2%) infants were excluded as their birthweight z scores were below −4 or above 4 (96 infants) or discharged to non-participating units (881 infants). Hence, 83 463 preterm infants with 4 878 314 daily episodes were analysed.
Neonatal practicesFrom 2010 to 2020, more mothers received antenatal corticosteroids, especially in infants born below 24 weeks GA (figure 1A). The proportion of infants who received surfactant decreased from 65% in 2010 to 60% in 2020 (figure 1B). The percentage of infants ventilated in the first 48 hours of life initially increased before declining during the latter part of the study period, with the total number of mechanical ventilation days remaining similar at a median of 1–2 days (online supplemental table 3).
 Figure 1
Figure 1 Heat map depicting the neonatal practices of (A) antenatal corticosteroids, (B) surfactant and (C) postnatal corticosteroids use in 83 463 preterm infants born below 32 weeks gestation in the respective years and gestational age as well as the (D) standard of care derived from the National Institute for Health and Care Excellence (NICE) guidelines.7 40 Data presented as the percentage of infants with the respective neonatal practice within each cell (total number of infants within each cell). Missing data on antenatal corticosteroids (n=693, 0.8%) and surfactant use (n=4778, 5.7%).
Overall, 6307 infants received PNC, increasing from 5% in 2010 to 11% in 2020 (figure 1C). The most commonly used PNCs were dexamethasone (4448 (5%) infants), followed by hydrocortisone (1629 (2%) infants), budesonide (1184 (1%) infants) and methylprednisolone (40 (0.05%) infants). A total of 928 (1%) infants received more than one type of PNC (online supplemental figure 1). Dexamethasone use increased, especially in extremely premature infants born below 28 weeks GA, from 11% in 2010 to 18% in 2020. The use of hydrocortisone remained between 3% and 4% from 2010 to 2016 before increasing to 12% by 2020 in extremely premature infants. Similarly, the use of budesonide increased from 1% to 3% in the first half of the study period to 8% by 2020 in extremely premature infants (online supplemental table 3 and figure 2).
Hydrocortisone was commenced at the earliest chronological age at a median (IQR) of 20 (4–42) days, followed by dexamethasone at 28 (19–43), budesonide at 42 (23–70) and methylprednisolone at 117 (88–156) days old (online supplemental figure 3). Across the birth years, dexamethasone was commenced at an increasingly earlier chronological age from a median (IQR) of 32 (22–49) days in 2010 to 27 (19–39) days in 2020 (p<0.0001). Similarly, hydrocortisone and budesonide were started at 28 (14–51) and 70 (46–119) days, respectively, in 2010 to 4 (1–23) and 34 (14–52) days, respectively, in 2020 (p<0.0001) (online supplemental table 4). In infants receiving dexamethasone, the percentage of infants receiving another PNC type increased from 6% in 2010 to 17% in 2020 (p<0.0001) (online supplemental table 4).
Neonatal outcomesOverall, mortality reduced from 10.1% in 2010 to 8.5% in 2020 (15% relative decrease) with the adjusted OR (aOR) decreasing to 0.70 (95% CI 0.60 to 0.82) in 2020. Conversely, there was an increase in the percentage of infants with BPD across the birth years from 28% to 33% (19% relative increase) and severe BPD from 12% to 17% (37% relative increase). A similar trend was found for the composite outcome of death and/or BPD as well as death and/or severe BPD with increases in incidence from 35% to 39% (11% relative increase) and from 21% to 24% (15% relative increases), respectively. The proportion of infants discharged on respiratory support increased from 13% to 17% (32% relative increase), with increasing CGA at discharge from a median (IQR) of 37+1 (35+5–39+1) to 37+1 (36+0–39+2) (p<0.0001). There was no statistically significant trend for the composite outcome of death or respiratory support requirement on discharge across the birth years (figure 2, online supplemental table 3 and figure 4). The increasing incidence of these poor respiratory outcomes matches the increasing aOR seen across the birth years (figure 3, online supplemental table 5). A total of 11 684 (16%) infants who required respiratory support at discharge were born earlier, more likely to be male, of lower birth weight and small for GA (table 1).
 Figure 2
Figure 2 Relative percentage of change for key neonatal practices and the incidence of outcomes from 2010 to 2020 in 83 463 preterm infants born below 32 weeks gestation, 26 098 extremely preterm infants born below 28 weeks gestation and 57 365 very preterm infants born between 28 and 31 weeks of gestation. Missing data on antenatal steroid course (n=693, 0.8%), surfactant use (n=4778, 5.7%), bronchopulmonary dysplasia (BPD) (n=414, 0.5%), severe BPD (n=414, 0.5%), discharge on respiratory support (n=725, 0.9%) and respiratory pressure support at discharge (n=725, 0.9%).
 Figure 3
Figure 3 Adjusted OR with 95% CI of the neonatal outcomes of (A) mortality, (B) bronchopulmonary dysplasia (BPD), (C) severe BPD, (D) any respiratory support requirement at discharge from the neonatal unit and (E) respiratory pressure support at discharge and their respective composite outcomes with death in (B–E) in 83 463 preterm infants born below 32 weeks gestation from 2010 to 2020. Missing data on mortality (n=251, 0.3%); BPD (n=492, 0.6%); BPD and/or death (n=661, 0.8%); severe BPD (n=492, 0.6%); severe BPD and/or death (n=661, 0.8%); discharge on respiratory support (n=801, 1.1%); discharge on respiratory support or death (n=970, 1.2%); respiratory pressure support at discharge (n=801, 1.1%) and discharge on respiratory pressure support or death analyses (n=970, 1.2%).
Table 1Clinical characteristics of preterm infants born below 32 weeks gestation included in the study
Similar improving mortality trend over the birth years (20% to 15%, p=0.004) was seen in the subgroup of 6307 infants who received PNC. However, no statistically significant trend was seen for the respiratory outcomes and the composite mortality and respiratory outcomes in these infants (online supplemental table 6 and figure 5).
Over the study period, the percentage of preterm infants who required invasive ventilation at 36 weeks CGA remained unchanged. However, the percentage of infants who required non-invasive ventilation at 36 weeks CGA and discharge increased from 10% to 15% and 1.1% to 1.4%, respectively (online supplemental tables 8,9 and figures 6,7).
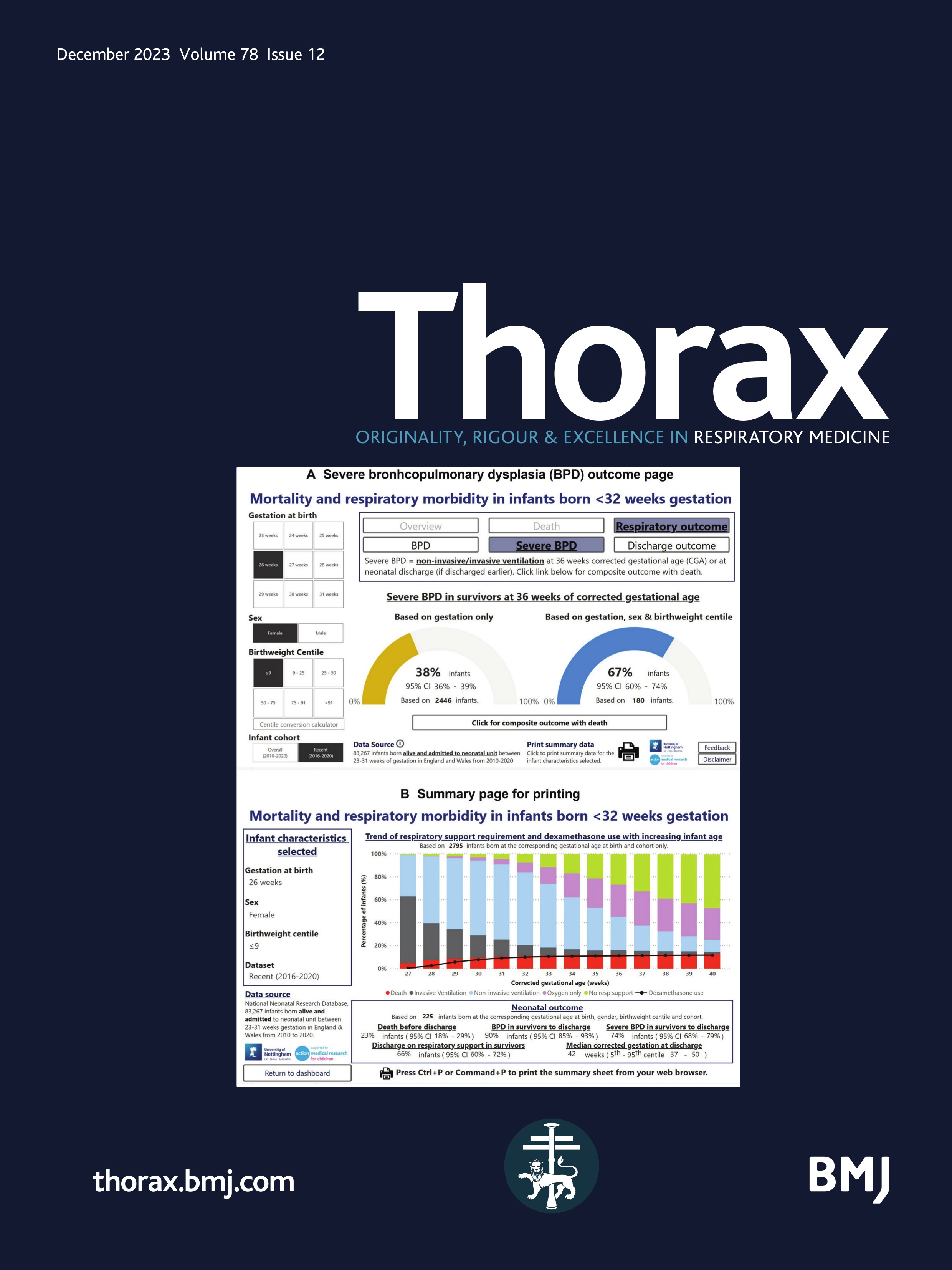
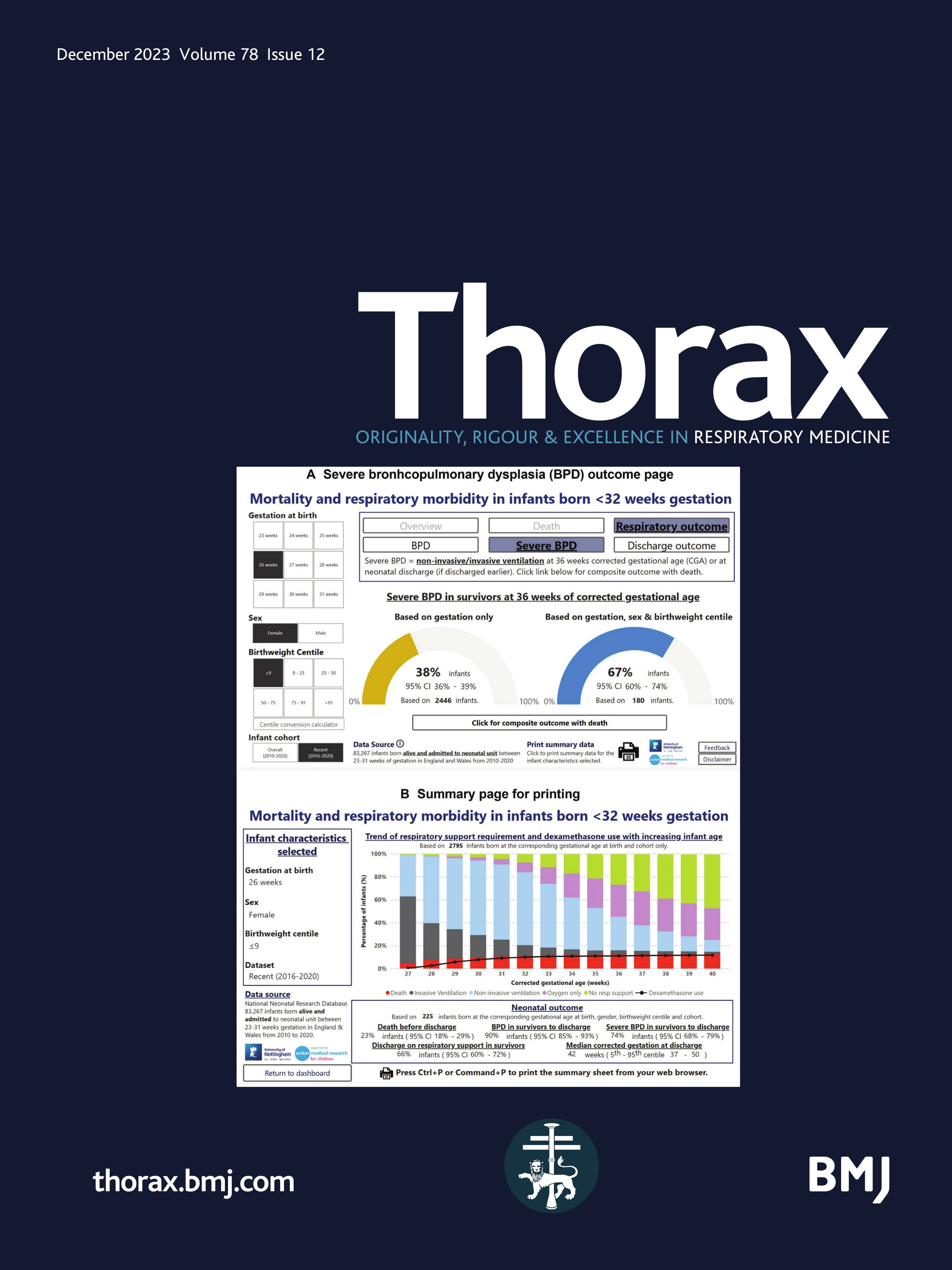
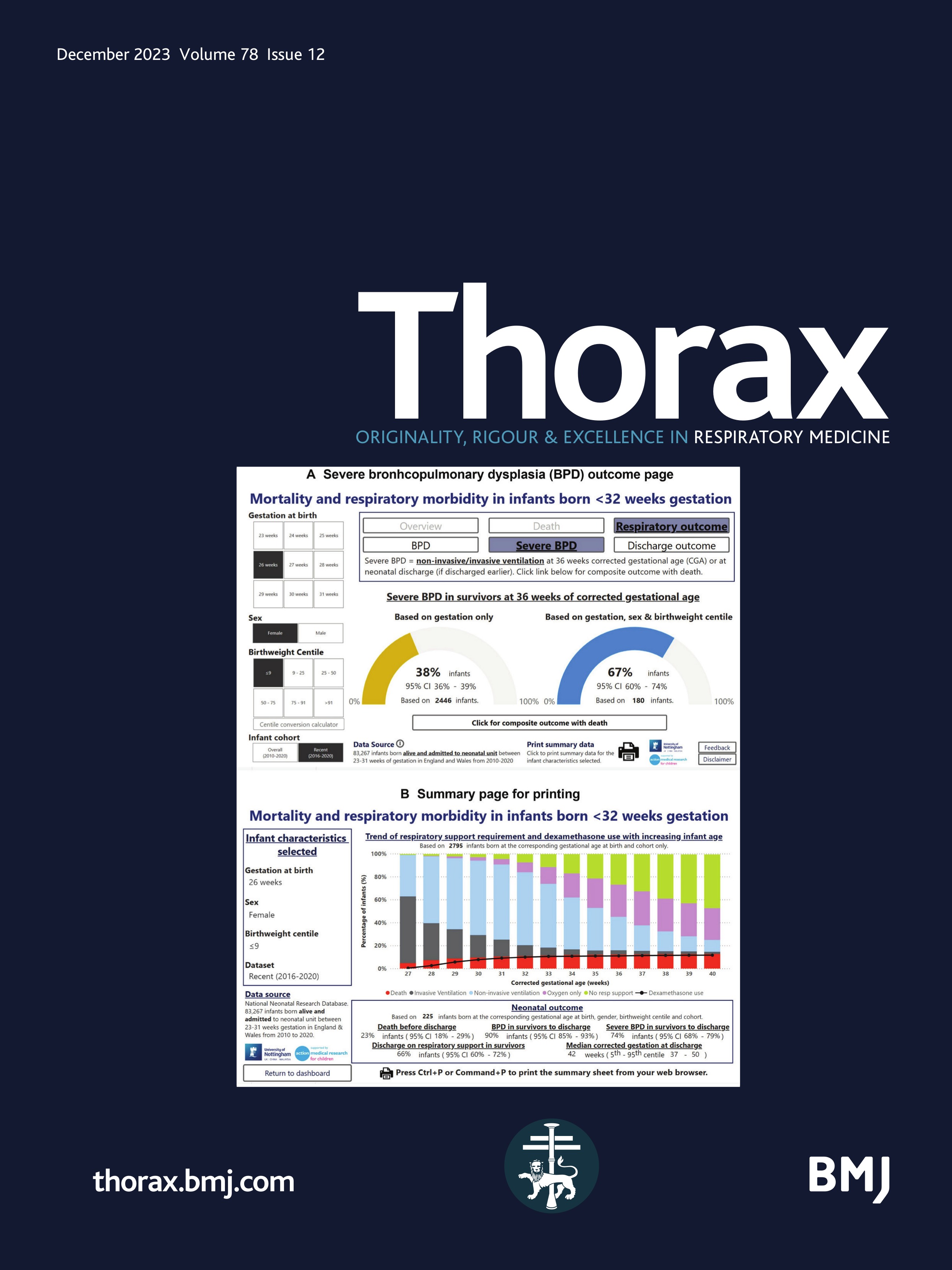
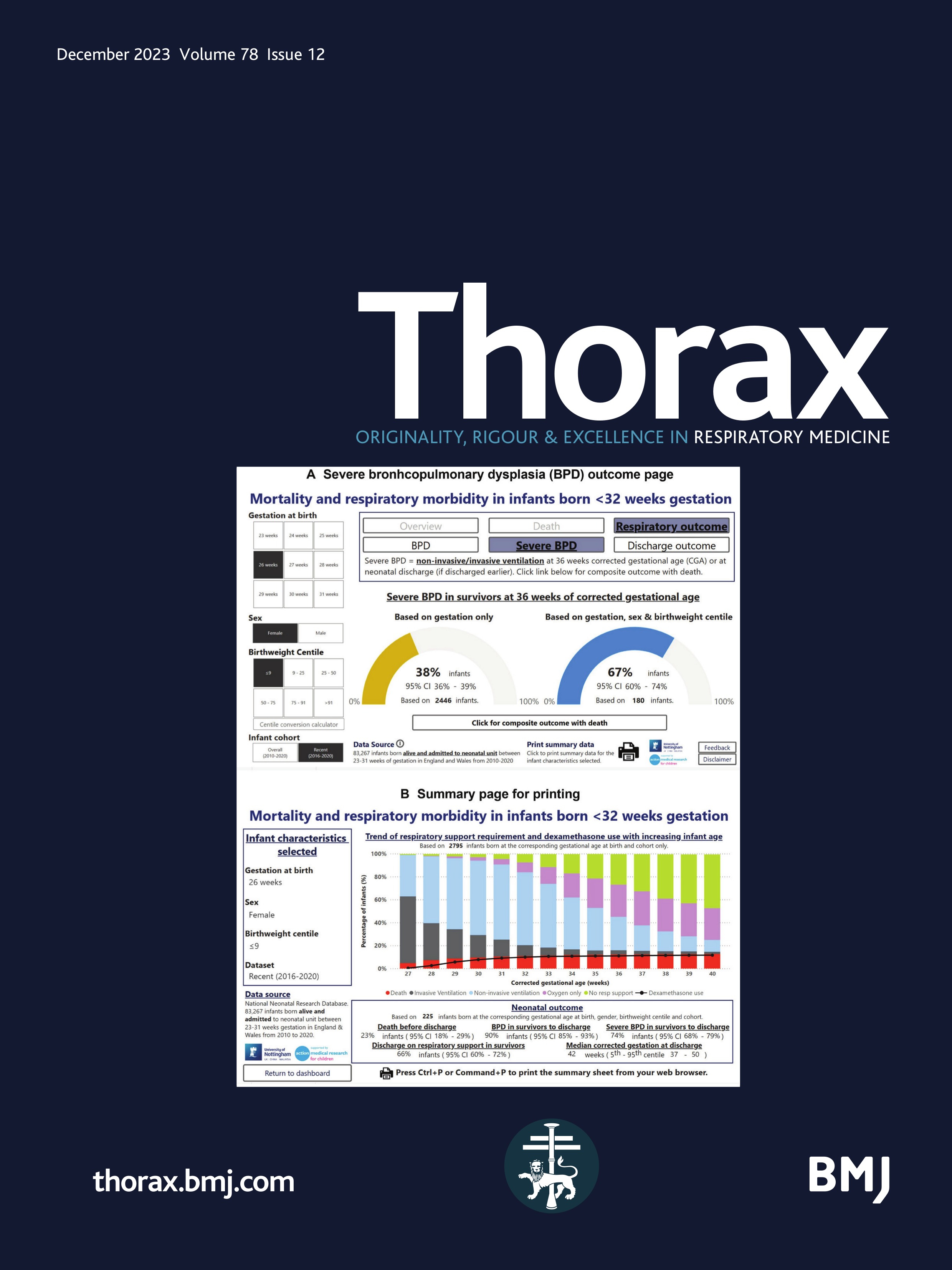
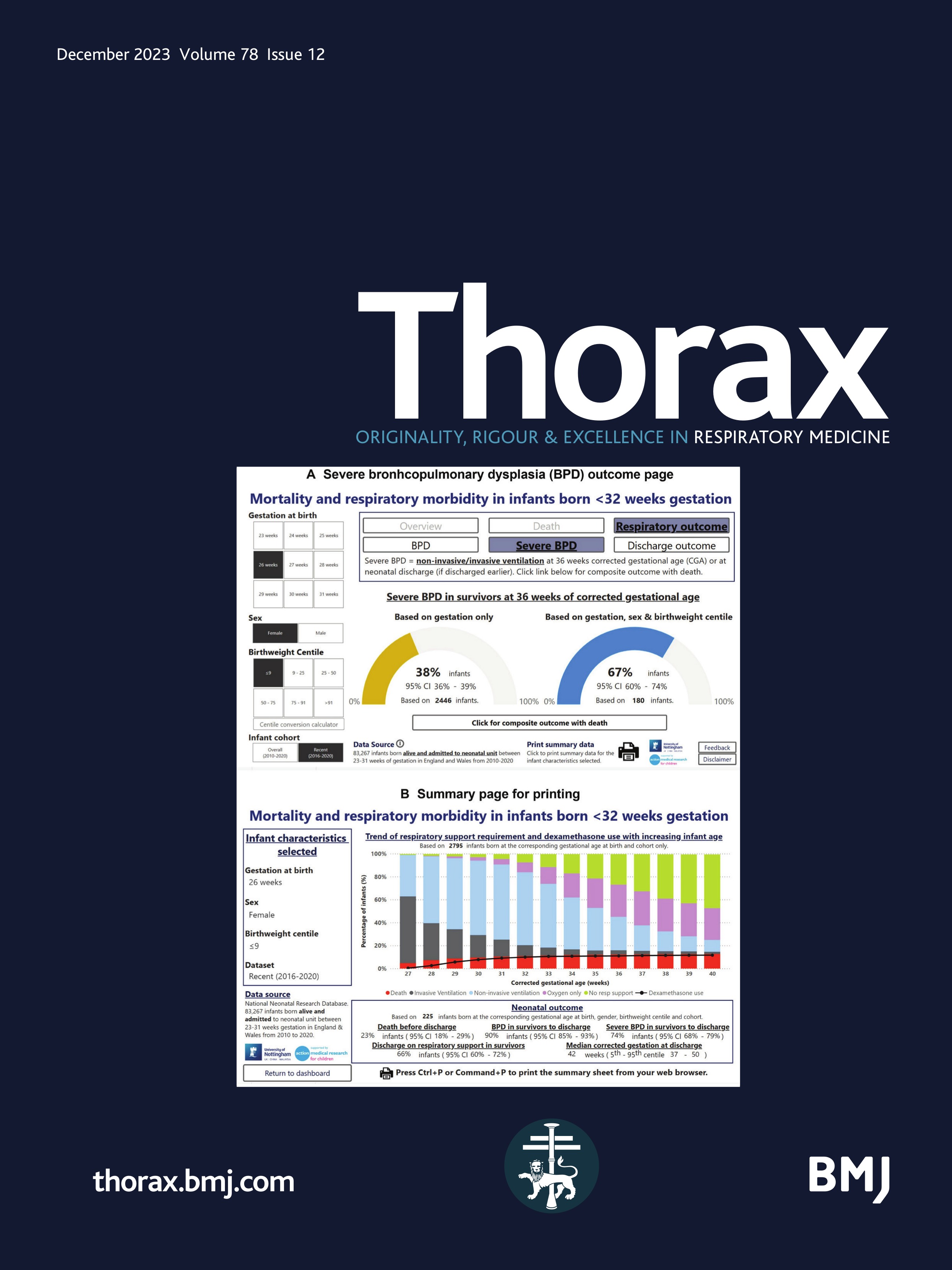
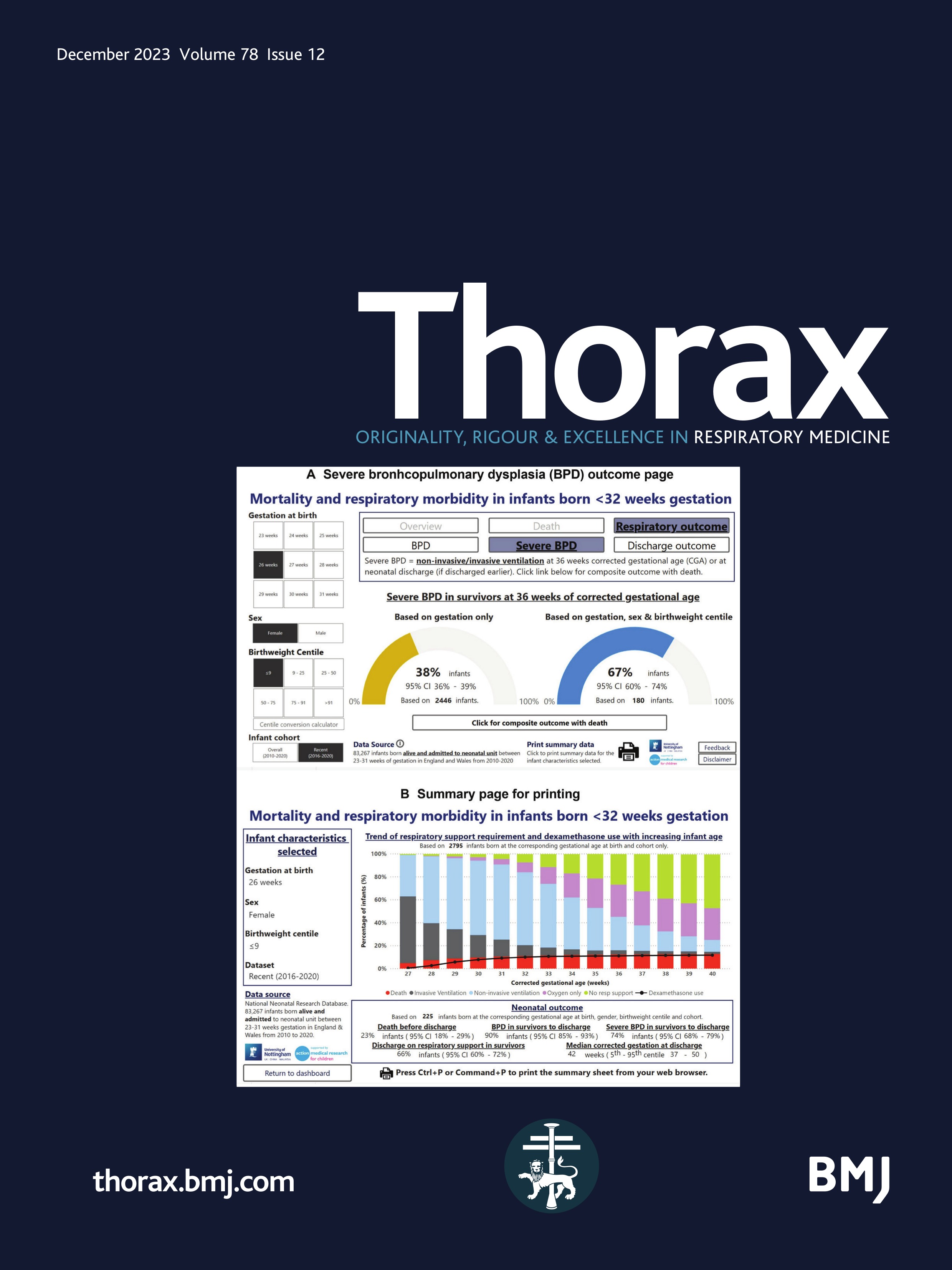
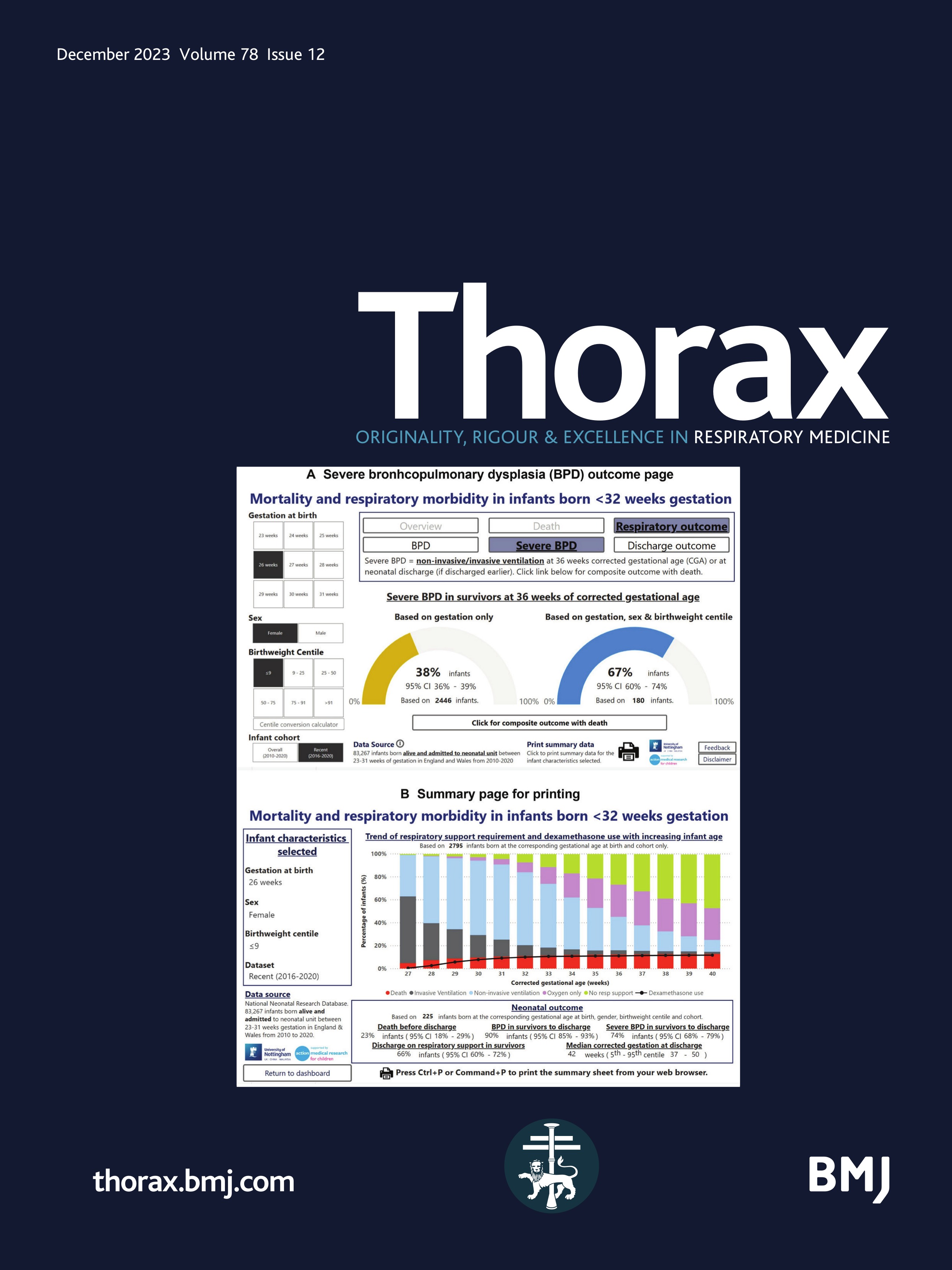
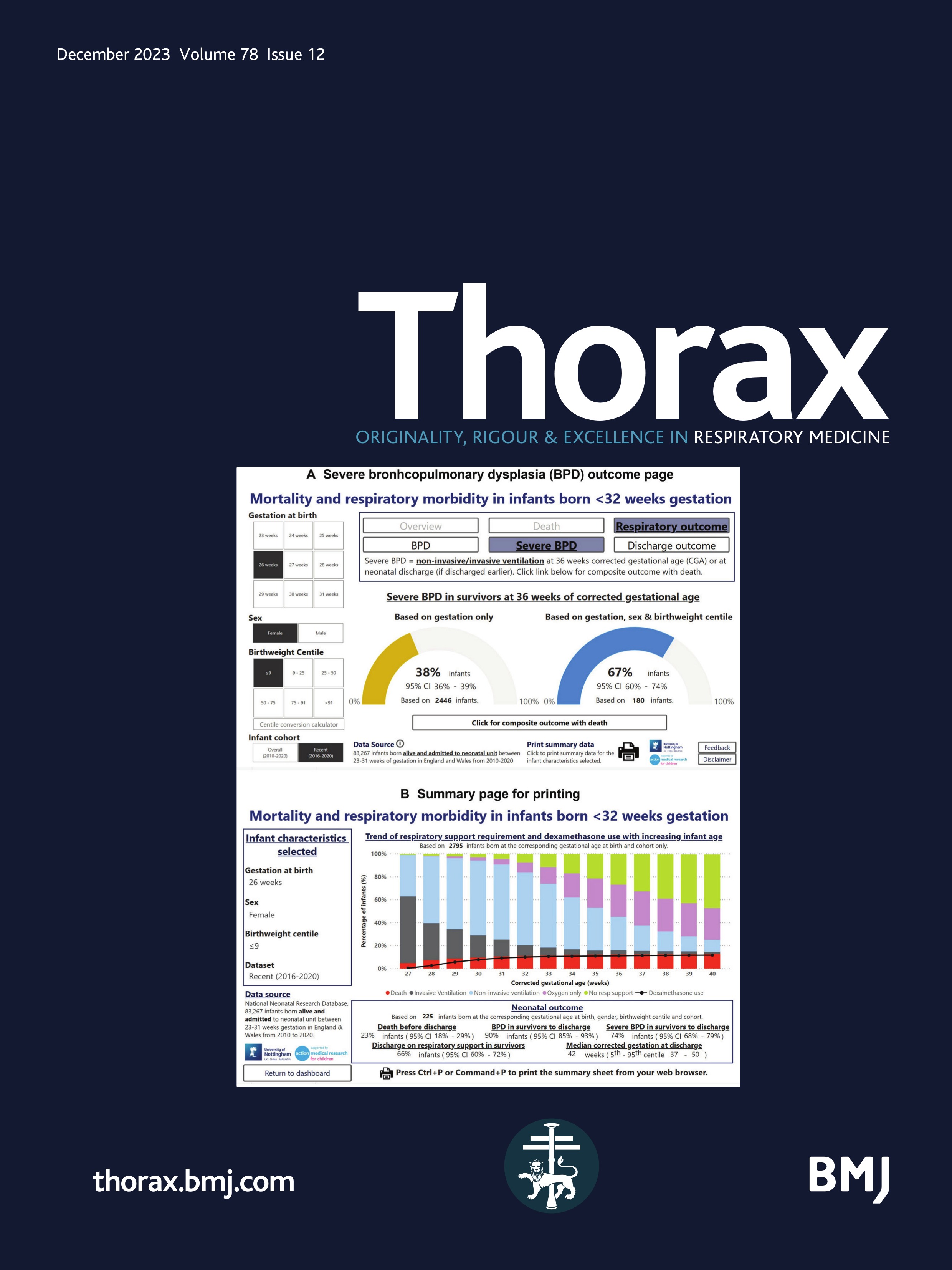
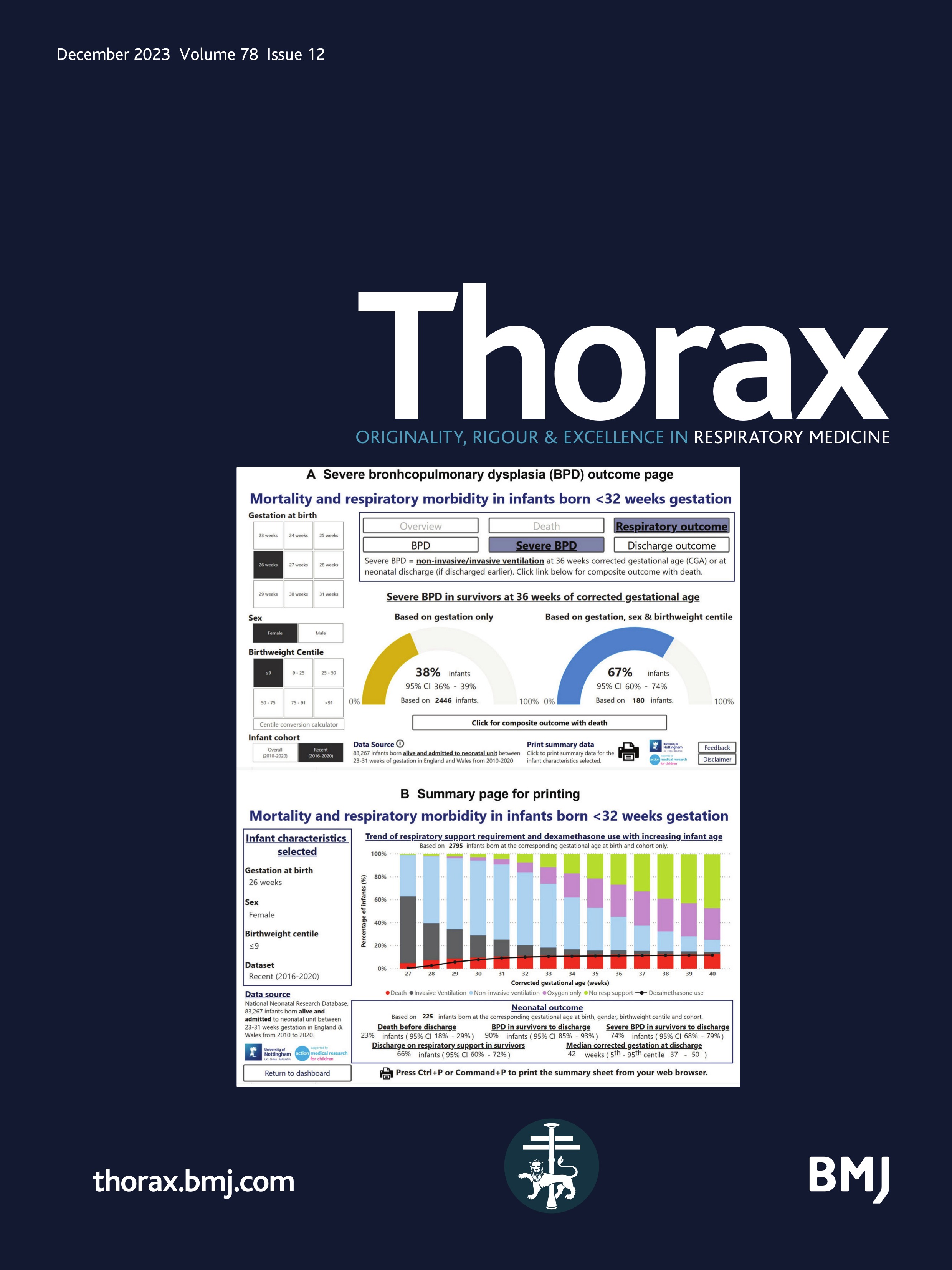
Mortality and respiratory outcome chartsGestation, sex and birthweight centile heat maps were produced for the 2010–2015 and 2016–2020 cohorts, depicting the incidence of mortality, BPD, severe BPD, postdischarge respiratory support and postdischarge respiratory pressure support requirement (online supplemental figures 8–12). Incidence of these outcomes varied based on birthweight centile and sex, alongside GA at birth. Despite born at the same GA, infants with extreme birthweight centile (≤9th or >91st centiles) generally have poorer outcome, demonstrating a U-shaped relationship. Similarly, male infants have poorer outcome than female infants. An electronic version of the charts, the preterm outcome dashboard (POD), was produced in an online dashboard accessible on (https://premoutcome.github.io/) with example screenshots shown in figure 4.
 Figure 4
Figure 4 Screenshots depicting the online dashboard displaying the incidence of mortality and respiratory outcomes in premature infants born between 23 and 31 weeks gestation. (A) Demonstrates severe bronchopulmonary dysplasia (BPD) outcome in surviving infants born at 26 weeks gestation, whereby the addition of sex and birthweight centile into the dashboard significantly worsens the outcome from 38% to 67%. (B) Complete respiratory outcome dashboard with data available on a weekly basis until 40 weeks of corrected gestational age (CGA) including those treated with postnatal steroids.
DiscussionThis national study is one of the largest using a contemporary high-risk preterm population of over 83 000 infants. It highlights the changing perinatal respiratory management,7 improving survival and increasing BPD rates. Importantly, we found increasing rates of more severe respiratory outcomes with a 37% increase in severe BPD, a 32% increase in respiratory support requirement after discharge and a doubling of PNC use especially dexamethasone. These findings have important implications for preterm infants with BPD as they may be subjected to a ‘double hit’ of neurodevelopmental impairment associated with both severe BPD and dexamethasone treatment.22 Furthermore, there is evidence suggesting the negative impact of dexamethasone on lung development into adulthood.23 Of concern, despite the increasing PNC use, 43% of extremely preterm infants in 2020 had severe BPD and required ongoing respiratory support at discharge, impacting paediatric intensive care services and ongoing respiratory physician follow-up. The development of POD, a preterm respiratory management and outcome dashboard, could help clinical teams to consider treatment options, care pathway planning and parental discussions, alongside international comparisons across populations.
Neonatal practiceAntenatal corticosteroids are known to reduce preterm mortality.24 The significant increase in mothers receiving antenatal steroids, especially in infants born below 24 weeks GA, may have contributed to the improvement in neonatal mortality seen and may reflect the change in practice among perinatal healthcare professionals in actively treating infants at increasingly earlier gestations.25
Optimal early respiratory care can significantly impact outcomes of very preterm infants, particularly respiratory health. Current preterm respiratory management aims to minimise mechanical ventilation,7 reserving it for infants where other methods of respiratory support, such as non-invasive ventilation, have failed.26 However, we found increased use of mechanical ventilation in extremely preterm infants, which may be partly explained by the increase in the proportion of infants born below 24 weeks GA being admitted. Surfactant use remained almost universal in infants born below 25 weeks GA across the study period in keeping with published guidance.26 However, in infants born above 25 weeks GA, its use appeared to be decreasing, perhaps with a switch to non-invasive ventilation strategies.26 This observation has some support from our recent report on the increasing use of early caffeine especially in extremely preterm infants during the same period.27 The increasing popularity of less invasive surfactant administration28 in more recent years may alter these patterns in the future, making these data useful for comparison.
Postnatal corticosteroidsDexamethasone is the most used PNC to aid extubation and prevent BPD in preterm infants with its use almost doubling over the study period despite lacking good quality evidence on the safety, optimal timing and dosage.29 Current UK guidance suggests considering giving dexamethasone after 8 days of life,7 but in this study period, it was commenced at a median age of 28 days, which may reflect clinicians’ anxieties about using it and difficulty in identifying which infants to treat. Overall, 29% and 17% of infants who received dexamethasone in 2020 required repeated courses of dexamethasone or another PNC type, respectively. The POD allows clinicians to understand GA-specific ventilation status and treatment with PNC across a whole population and so may provide benchmarking of their own care for infants in their hospitals.
From 2017 onwards, hydrocortisone use doubled and was commenced at an increasingly earlier age. This is likely due to the recent publication of the PREMILOC clinical trial16 and guidelines17 on prophylactic hydrocortisone use in extremely preterm infants. Nearly a quarter of infants receiving hydrocortisone in 2020 required another PNC course. Budesonide use has also increased in the latter half of the study period despite lacking evidence supporting its use and possibility of increased mortality.15 30
Neonatal outcomesOverall, around 2000 infants developed BPD annually with a 19% relative increase in rates during the study period. These trends are seen in some, but not all, high-income countries.31 Similar studies32 across large populations have not reported such detailed respiratory outcomes, particularly relating to BPD severity, and how these link with key infant characteristics. During the study period, nearly 12 000 very preterm infants (over 30% relative increase) had severe BPD and required respiratory support at neonatal discharge, both important outcomes for parents.5
This rising BPD rates, particularly severe forms, are likely to be multifactorial including the increasing number of extremely premature infants admitted to neonatal units and surviving. In addition, the role of changing respiratory management, such as higher oxygen saturation targets following the BOOST33 and SUPPORT34 trials, may have had an effect as these are associated with an increase in BPD rates.
Rates of severe BPD and postdischarge respiratory support will likely continue to increase as many countries, including the UK,25 consider active management of infants born from 22+0 weeks. This could have a significant impact not only on neonatal capacity and healthcare costs, but also on paediatric and adult healthcare services. Infants with BPD, particularly those requiring respiratory pressure support or home oxygen, have increased healthcare use,4 ongoing community care, respiratory syncytial virus vaccination,35 more hospital readmissions and longer hospital stays.3 As early respiratory health is linked to longevity, these infants may also have premature mortality as adults.36
Outcome charts and POD online dashboardEven large tertiary neonatal intensive care units still see relatively small numbers of preterm infants requiring treatment with dexamethasone or postdischarge positive pressure ventilatory support. To better inform on outcomes in this population, we have developed contemporaneous charts and an online dashboard depicting the incidence of mortality and key respiratory outcomes stratified by sex, gestation and birthweight centiles. The variation of the incidence of outcomes based on these key characteristics highlights a need to move away from the ‘one-size-fits-all’ approach in managing preterm infants based on just their GA at birth. Instead, a holistic approach comparing other key infant characteristics is needed, although this needs to focus on key characteristics so avoiding patient numbers being too small and hence CIs large. These updated mortality and respiratory outcome charts are the largest and most recent to date. Previous outcome charts37 have not detailed important respiratory outcomes in such a large population. More recent data visualisation tools provide useful mortality data but do not offer individualised detailed incidence of the type of respiratory support requirement, postnatal dexamethasone use or outcome information at weekly intervals during the whole neonatal stay depicted in our online dashboard (figure 4B), something parents and clinicians are keen to understand.38 The POD dashboard could aid clinicians in tracking the progression of the respiratory outcomes in the infants they care for on a weekly basis with the anticipated outcomes from a national population. The visualisation of the incidence of respiratory outcomes in this manner may help difficult discussions with parents and support the decision-making process on a targeted approach for high-risk treatments such as dexamethasone, especially as good prediction models for BPD are still lacking.39 The charts also provide clinicians and researchers with more recent data on the incidence of important outcomes when designing research studies, planning care pathways and resource allocation, and considering the needs of these children as they grow and transition into adult services. We anticipate updating the POD data every 2 years with the next update being in mid-2023 once all infants admitted in 2021/2022 are discharged.
StrengthsOur large cohort represents almost all neonatal admissions of infants born below 32 weeks gestation in England and Wales. To the best of our knowledge, our study is one of the largest national cohort studies to investigate the recent trends in the incidence and severity of BPD, respiratory support requirements and mortality. By using nearly 5 million contemporaneous point-of-care electronic daily records, we analysed the respiratory support over a 3-day period at 36 weeks CGA to facilitate an up-to-date assessment of BPD and respiratory support requirements. We have also focused on important outcome measures beyond BPD, which are crucial to healthcare professionals and parents, and align with ongoing respiratory morbidity. The novelty of our study is the data visualisation approach used to demonstrate the variation of the incidence of detailed respiratory outcomes based on key infant characteristics and visualisation of outcomes at weekly intervals.
LimitationsWe do not have the true denominator of total live births across whole study period. Hence, this needs to be considered when interpreting these data. This is particularly the case for infants below 24 weeks GA where many may not be admitted for neonatal care and so would not be registered in this database. However, this is unlikely to alter our findings significantly on the trend of neonatal practices and outcomes across the study period as the discrepancy between the number of infants born below 24 weeks GA in our cohort as compared with the number of registered live births10 remained at around 70% over the study period.
As a retrospective study, we cannot quantify the impact of the evolving clinical practices individually on neonatal outcomes and so causal effects cannot be drawn. Additional changes in practice, such as delayed cord clamping, oxygen saturation targeting or ventilation advances (eg, volume ventilation), cannot be accounted for in this dataset. Although the dose and indication of PNC were not available from the dataset, the definition of PNC was based on the current clinical practice,12 ensuring that the PNC was intended to prevent BPD. Data are recorded in the database during clinical care so input inaccuracies and missing items could not be controlled for. Caution is required when interpreting some of the heat map cells with small numbers, particularly at the extremes of gestation and birth weight.
ConclusionAcross a national health service, we continue to see improvements in the perinatal care and survival of very preterm infants. However, this is associated with the need for more potentially hazardous treatments, such as PNC, and longer pressure-assisted ventilatory support in high-risk, extremely preterm infants. Importantly, these trends continue with significantly more infants being diagnosed with severe BPD and requiring respiratory support after discharge. These findings have important implications for healthcare professionals and policy-makers as this will require greater resources for neonatal and paediatric respiratory and intensive care services. The burden of medium-term and long-term respiratory morbidity and neurodevelopmental issues will also impact educational and adult healthcare services. There is a need for robust clinical trials in this high-risk population to evaluate the effectiveness of early respiratory care, better targeting and timing of preventative treatments, and postdischarge studies to improve long-term outcomes.
Comments (0)