
Remember me

Based on a post-positivist paradigm, this quantitative, experimental study compared two teaching techniques for their effectiveness. The hypotheses state that the blended approach will be non-inferior to the traditional approach in terms of skill performance, skill retention, student and teacher satisfaction and additionally will need less face-to-face teaching time compared to the traditional technique.
The sample size was calculated based on previous skill performance score distributions of checklist ratings [6, 11] combined with the insights of five ETC instructors regarding current pelvic binder application criteria. The study was designed to identify a 4-point score difference (25% of total score) between two groups, with 80% power, a 0.05 alpha level, and a common standard deviation of 6. The resulting sample size required was 35 for each group.
The study population was made up of ETC candidates. Centres in England (Birmingham, Manchester, Stafford) and Belgium (Antwerp, Ghent) were selected for participation based on course availability, willingness to participate and researchers' travel duration. All candidates were contacted via email one month before their course. Prior exposure to any form of pelvic binder instructions was not counted as an exclusion criterion as the majority of ETC candidates work in trauma care and are expected to have had some exposure to pelvic binder application.
The standard ETC Master Data File (MDF) on Microsoft Excel 2016 was used to randomly allocate participants to one of the two study groups. Participant information and consent forms kept details about the study hypotheses and teaching techniques confidential, blinding participants to these aspects. Instructors were manually assigned to the teaching sessions by a blinded course director. Double blinding was not possible due to the need for instructors to be informed about both teaching techniques to safeguard teaching consistency during the course.
DesignSettingThe study occurred over five courses, each lasting 2.5 days. Pelvic binder teaching sessions took place on the first day, with 2 to 4 instructors teaching groups of 4 candidates. Sessions for control and research groups were conducted simultaneously in different rooms, and instructors taught the same session three times.
Procedure for the control – and research groupFigure 1 illustrates the distinct teaching approaches for the control and research group.
Fig. 1
Study design. Two groups received skills training for pelvic binder application; a face-to-face 4-step approach for the control group and a blended modification for the research group. Both groups were assessed for their performance immediately after the teaching session and 2 days later (retention). Further outcome measurements were the time needed for teaching and learner/teacher satisfaction
Self-study for both groupsCandidates were expected to read the ETC course manual's pelvic binder instructions, before the course.
Online module for research groupThe research group received an additional online module two weeks before the course, including theoretical content, videos showing step 1 and 2, online activities for step 3, and self-assessment questions.
All instructors received the online module, with the instructors for the control group instructed to teach the skill as shown in the online module to standardise teaching.
Face-to-face teachingStep 1 for both groups was a real-time demonstration of pelvic binder application during a simulated trauma scenario, aligning with the concept of contextual learning [12].
Steps 2–4 for the control group involved a detailed explanation, followed by candidates guiding each other through the application with corrective feedback from the instructor and further time to practice.
The research group, having completed steps 2 and 3 online, immediately performed step 4 with corrective feedback from the instructor and practice time.
Instructors measured the time required to teach pelvic binder application. The control group's time covered steps 2 to 4, while the research group's time only included step 4. Step 4 was deemed complete when candidates felt competent to perform the skill. Although the control group had more steps, the effectiveness of the online module in preparing the research group was uncertain, possibly leading to a much longer step 4 for the research group due to more corrections and questions.
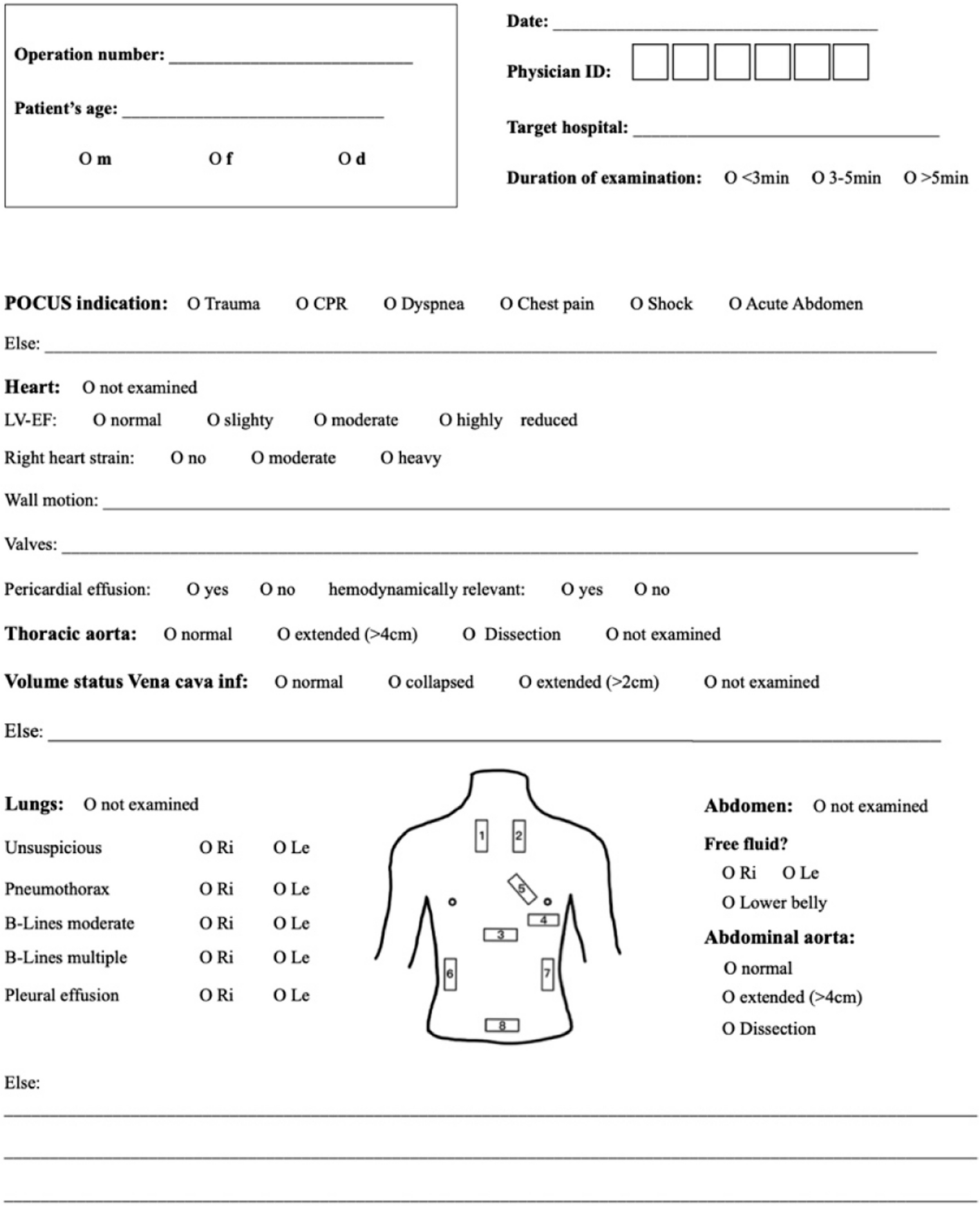
AssessmentAfter step 4, instructors assessed candidates' skill performance using a standardised checklist, which was based on the regular ETC criteria and the European Trauma Course Manual [13] and modified after consultation with 10 experienced ETC instructors for content and face validity (Additional file 1). Like prior studies [6, 14], a trinary scoring scale was used.
EvaluationAfter the teaching session, candidates were asked to rate their satisfaction with the teaching technique on a 5-point Likert scale, covering the aspects of explanation, feedback, practice time, and assessment objectivity (Additional file 2). For the research group, this included both online and face-to-face teaching. Additional questions covered prior training exposure and time spent on the online module.
Instructors also rated their satisfaction on a 5-point scale, focusing on time for feedback and practice, objectivity of assessment, and comparing blended learning to the standard technique if in the research group (Additional file 3).
RetentionAll candidates completed a second performance assessment (retention assessment) on day three in a separate room with an assessor, a research assistant and a manikin.
Comments (0)