
Remember me


This prospective randomized study was conducted at Benha university hospital, urology department in the period from February 2022 to February 2023. All patients applied written informed consent and our local ethical committee approval was obtained (MD.9.2.2022). The inclusion criteria involved patients aged ≥ 18 years with single large impacted upper ureteric stones (located just below PUJ and above the lower limit of the fourth lumber vertebra) ≥ 1.5 cm in maximum dimension. Patients with kidney stones, obstruction distal to the stone, active UTI and pregnant females were excluded.
Patients were randomly divided into two groups using a closed-envelopes method.
Group A: included 31 patients who treated by antegrade FURS procedure and holmium laser fragmentation.
Group B: included 30 patients who treated by retrograde FURS procedure and holmium laser fragmentation.
All patients subjected to complete history taking, physical examinations. Urine analysis, urine culture, serum creatinine, complete blood count, hepatitis marker and coagulation profile were assessed as preoperative laboratory investigations. Patients with positive urine culture received the specific antibiotic up to the urine culture registered negative. while patients with negative urine culture received a single dose of first generation cephalosporin for operation. Radiological investigations for all patients were done, including pelvic-abdominal ultrasonography (us), plain radiograph of the kidneys, ureters and bladder (KUB) and non-contrast CT to determine stone criteria.
Operative techniqueAll procedures carried out by two consultants and experienced endourologist.
Group A: Antegrade flexible ureteroscopy procedure (Antegrade FURS)Under spinal anesthesia, patients were moved to Supine Modified Galadako Valdiva Position as this position permitted simultaneous antegrade and retrograde access so the patients were drapped once and repositioning was not required. Cystoscopy was performed and 6 fr ureteric catheter was inserted into targeted ureter just below the stone, as passage of ureteric cathter in ease considered as a marker of no significant distal obstruction and also, act as a landmark when appear in the field that the stone is completely fragmented, then cystoscope removed and 16 fr bladder catheter was inserted which fixed to the distal end of ureteric catheter. While the patients in the same position and under the ultrasound guidance the collecting system was punctured through the lower calyx. After confirming the safe placement of the needle into the collecting system by free urine flow, the contrast agent was injected through the needle to opacify the collecting system under fluoroscopy. After which a guidewire (0.038) was inserted into the collecting system through the needle and skin incision was made then the needle removed. Dilatation of the tract up to 14 fr was done using amplatz dilators followed by introduction of ureteral access sheath (UAS) (Navigator 13/11 F, 46 cm: Boston Scientific) over the guide wire (Fig. 1a). Through the access sheath, we inserted another guidewire into the collecting system (Fig. 1b). The access sheath was then removed, one of the two guidewires was used as safety wire while the second was used to introduce the access sheath again into the collecting system(Fig. 1c) then removed to introduce the flexible URS (9.5 Fr The LithoVue™ System Boston Scientific) through access sheath until reach the stone (Fig. 1d). The stone was fragmented using the holmium laser (Lumenis® Pulse™30H) with energy 0.8–1 J per pulse and repetition rate 6–10 HZ. At the end of the procedure, the JJ stent was inserted in antegrade manner and the access sheath removed without inserting a nephrostomy tube.
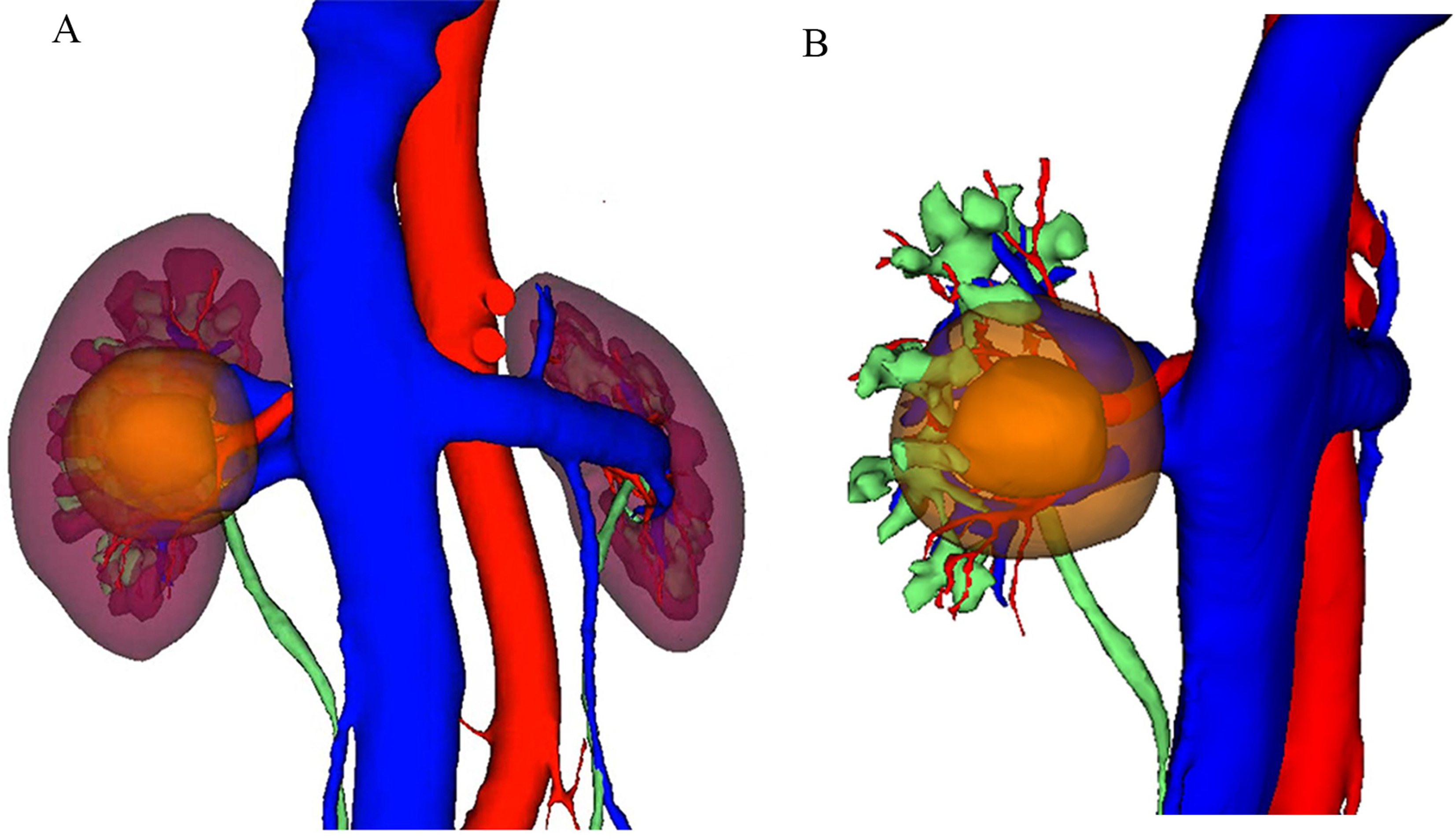
Fig. 1
a Introduction of ureteral access sheath over the guide wire. b Another guide wire insertion through access sheath. c Safety guide wire and access sheath inside collecting system. d Flexible URS reaching the stone
Group B: Reterograde flexible ureteroscopy procedure (Retrograde FURS)Under spinal anesthesia, patients were put in the dorsal lithotomy position. Cystoscopy was performed and two guidewire were inserted in the targeted ureter. One of them was used as safety wire while the other was used for advancing the flexible URS upto the stone. Before the reterograde FURS maneuver, ureteral dilatation was done by balloon dilator if needed. Flexible URS was performed with a 9.5 Fr The LithoVue™ System-Boston Scientific. The stones were fragmented with the same laser device and settings as in group A. At the end of the procedure JJ stent was inserted in a reterograde manner.
In both groups, the irrigation flow depended on gravity- based irrigation using saline and fragments were left for spontaneous passage after fragmentation into very tiny fragments.
Both groups were compared as regard preoperative data (Age, Sex, stone characteristics), intra-operative data (Operative Time, Lithotripy time, Fluroscopy time, complications), and postoperative outcomes (stone free rate, complications, need for auxiliary procedure).
Operative time was defined in both groups as the time from cystoscopy until JJ stent insertion. Two weeks after the procedure in both groups, all patients undergone non contrast CT before JJ stent removal to assess SFR which was defined as absence of residual fragment ˃ 3 mm.
The primary endpoint of the present study was the SFR at 2 weeks. The secondary endpoint included intraoperative data (operative time, time for lithotripsy and fluoroscopy) and postoperative complications.
Statistical analysisThe Statistical package for Social Science (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp.) was used for data management and analysis. Descriptive statistics were presented as Mean, Standard deviation (± SD) or numbers and percentages. Chi-Square test was used to assess the relationship between two qualitative variables. Student T Test was used to detect the statistical significance of the difference of the parametric variable between two study group means. Fisher’s exact test was used to estimate the relationship between two qualitative variables. The P value is considered significant if < 0.05.
Comments (0)