
Remember me



Organ transplants save lives and improve quality of life for patients who receive them.1 Along with recognizing these benefits, it is equally important to recognize that not receiving a transplant has profound negative effects on waitlisted candidates with low allocation priority. Candidates who spend an extended time on transplant waiting lists are at risk of death or delisting before transplantation, and even those who ultimately receive transplants may have inferior post-transplant outcomes attributable to delayed transplantation.2,3 The zero-sum features of organ allocation policy require trade-offs between the ends of equity, utility, urgency, feasibility, efficiency, and cost, with additional efforts to reduce disparities in transplant access while balancing these factors.
A particularly challenging topic in US organ allocation is the allocation of organs for use in multiorgan transplantation. Patients with multiorgan failure may be clinically ineligible for a single-organ transplant but eligible to receive two or more organs from the same deceased donor, such as a patient with advanced heart failure and end-stage kidney disease who is deemed a medically unsuitable candidate for either a heart or kidney transplant in isolation but may be a candidate to receive a combined heart–kidney transplant. Multiorgan transplant eligibility criteria vary by organ combination and transplant center. In the absence of strict policies defining multiorgan listing criteria, patients with mild kidney impairment (e.g., eGFR 50–59 ml/min per 1.73 m2) may be listed for multiorgan transplants in anticipation of early post-transplant kidney failure if a single-organ transplant were to be performed. Optimizing the multiorgan allocation policy requires maintaining access to transplant for patients for whom single-organ transplantation is truly clinically inappropriate while avoiding overutilization of combined-kidney transplantation in ways that unfairly compromise organ access for kidney-alone candidates. Reaching a consensus on how to strike this balance is currently an Organ Procurement and Transplantation Network (OPTN) policy priority that has received a wide range of public comments to date.4
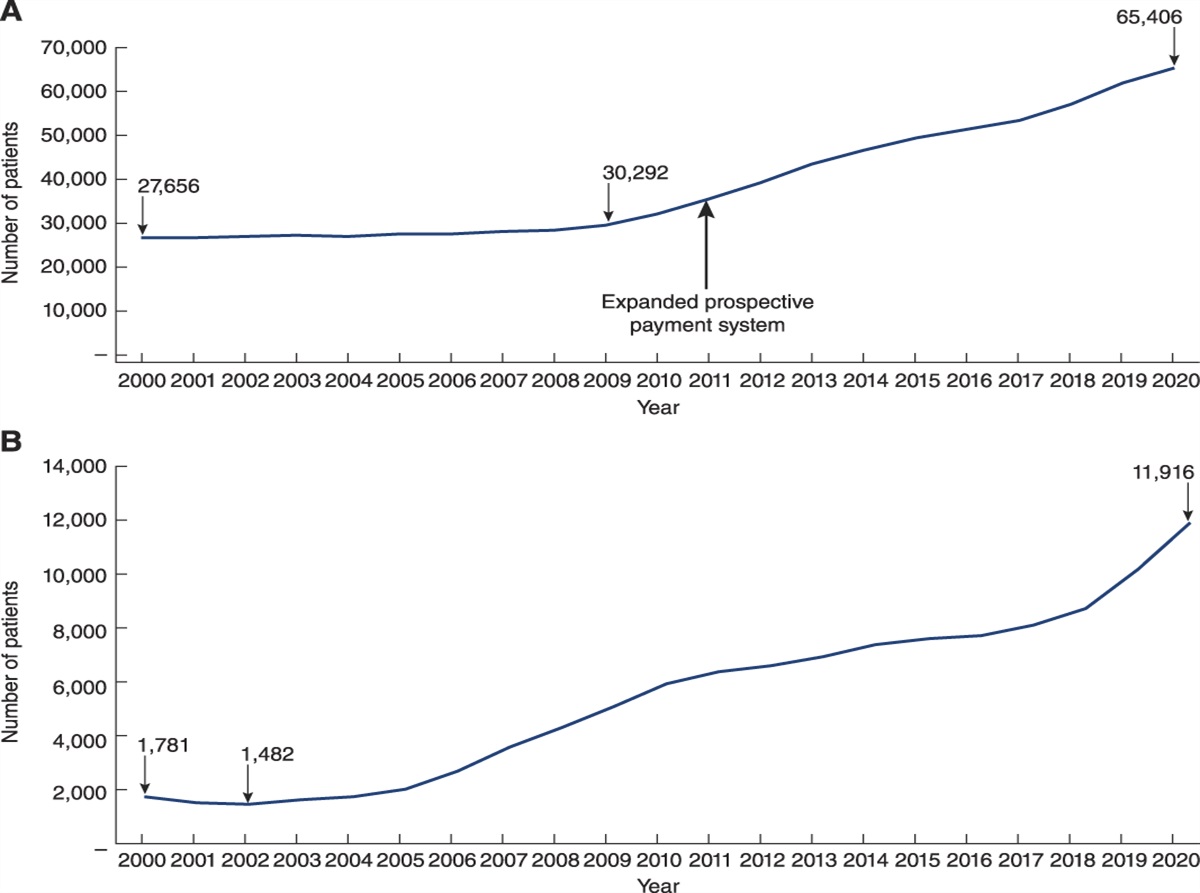
Growth in Multiorgan Transplantation Involving KidneysThe growth in multiorgan transplantation involving kidneys has outstripped the growth in kidney transplantation over the past two decades. OPTN data show a doubling of annual deceased donor kidney transplant volume from 2000 to 2020, but a six-fold increase in multiorgan transplants involving kidneys (Figure 1A). In the post–Kidney Allocation System (KAS) era, thoracic–kidney multiorgan transplants (Figure 1B) have grown faster proportionally than abdominal organ–kidney multiorgan transplants (Figure 1C). This rapid and disproportionate growth merits additional monitoring to ensure appropriate organ utilization and allocation. Pancreas–kidney transplantation has historically, and appropriately, been excluded from descriptions of multiorgan transplants because the criterion for kidney candidacy for pancreas candidates is the same as that for kidney transplant alone, unlike for liver–kidney candidacy (higher GFR eligibility threshold) or lung–kidney/heart–kidney candidacy (GFR threshold unestablished). In this context, pancreas–kidney transplantation did not significantly increase despite kidney–pancreas allocation changes in 2014 favoring increased pancreas transplantation, suggesting that more efforts are needed for these kidney–pancreas candidates.5
 Figure 1:
Figure 1: Multiorgan transplantation in the United States. There has been a continuous rise in the use of multiorgan transplants involving kidneys over the past two decades that has increased out of proportion to deceased donor kidney transplantation (A). The period after the implementation of the KAS has seen a sharper proportional rise in two-organ transplants involving kidneys with thoracic organs (B) compared with kidneys with abdominal organs (C). Furthermore, although recipients of deceased donor kidney transplants have several sociodemographic disadvantages over recipients of multiorgan transplants involving kidneys since the implantation of KAS (D), kidney-only deceased donor transplants have a lower risk of death or graft failure when considering transplants using kidneys with either KDPI ≤20% (E) or KDPI >20% (F). KAS, Kidney Allocation System; KDPI, Kidney Donor Profile Index.
Several factors likely contribute to the rise in multiorgan transplantation. AKI is increasingly common among non-kidney transplant candidates. The extended waiting time for most candidates on the kidney waiting list increases the appeal of multiorgan listing to mitigate the perceived risk if a patient has incomplete recovery of kidney function and develops advanced kidney disease soon after non-kidney organ transplant. Apart from liver transplant candidates for whom an expedited access safety-net pathway to kidney-after-liver transplantation was established for patients left with advanced kidney disease in the first post-liver transplant year, non-kidney solid organ transplant recipients who develop a need for a kidney transplant are likely to spend several years on the waiting list in the absence of an available living donor. Importantly, however, even the implementation of the kidney safety net was not followed by a sustained decrease in the number of liver–kidney transplants performed (Figure 1C), perhaps related to higher MELD scores—and, therefore, liver allocation priority—resulting from elevated creatinine in liver–kidney candidates. In addition, the exclusion of multiorgan transplants from transplant center performance metric cohorts creates an unintended incentive favoring increased utilization of multiorgan transplants by removing the potentially adverse contribution of some high-risk patients to program-specific reports.6
Multiorgan Allocation and Transplant of KidneysCurrent deceased donor kidney allocation policies explicitly prioritize multiorgan candidates over kidney-alone candidates stating,
“If a host OPO procures a kidney along with other organs, the host OPO must first offer the kidney according to one of the following policies before allocating the kidney to kidney alone candidates according to Policy 8: Allocation of Kidneys:
▪Policy 5.10.C: Other Multi-Organ Combinations
▪Policy 9.9: Liver-Kidney Allocation
▪Policy 11.4.A: Kidney-Pancreas Allocation Order”
This prioritization scheme allocates kidneys in a manner inconsistent with the priorities of kidney-alone allocation, which favors transplantation for patients with longer waiting times, pediatric candidates, highly sensitized candidates, and prior living donors.6,7 In contrast to kidney-alone recipients, recipients of multiorgan transplants are more likely to be White and privately insured (Figure 1D), an outcome inimical to the goal of ameliorating health inequities. Recent OPTN policy proposals pertaining to multiorgan allocation involving kidneys have not included data studying which kidney-alone candidates are most affected by current/proposed multiorgan policies. Although fewer than 10% of deceased donor kidney-only transplants since 2015 have been to preemptive recipients, multiorgan transplant recipients frequently have little or no pretransplant dialysis, including that most of the lung–kidney and heart–kidney recipients never received dialysis before kidney transplantation (Figure 1D). Because multiorgan allocation is driven by the non-kidney organ, these disparities are attributable to demographic differences in kidney versus non-kidney candidates.
There has been insufficient study of the outcomes of multiorgan kidney transplant recipients that could be used to understand the effect of the growth in multiorgan transplantation on transplant system utility. Multiorgan transplants typically use higher-quality kidneys, with Kidney Donor Profile Index ≤20% of kidneys used in approximately half of thoracic–kidney transplants and over one third of liver–kidney transplants, yet their recipients have a higher rate of death or kidney allograft failure than recipients of kidney-alone transplants (Figure 1, E and F). These inferior outcomes attenuate the overall utility of deceased donor kidneys. Furthermore, reduced access to high-quality kidneys for young kidney-alone recipients may increase their future need for kidney retransplantation.6,7 Finally, multiorgan prioritization is asymmetric and always driven by the non-kidney organ, so multiorgan candidates with a higher priority for a kidney are not prioritized to receive a heart, lung, or liver from a matched kidney donor even if their non-kidney organ dysfunction makes a kidney-only transplant infeasible or unsafe. The frequency of primary graft dysfunction and early mortality among thoracic transplant recipients also supports increased reliance on safety-net kidney allocation for stable thoracic recipients with persistent post-transplant kidney dysfunction over multiorgan allocation.8
Data Needs for Potential SolutionsThe elimination of multiorgan transplantation is neither desirable nor justified because multiorgan transplant is the only possible treatment for some patients with multiple end-stage organ diseases. However, given increasing utilization, updated allocation policies are needed to ensure balance in transplant access for kidney-alone versus multiorgan candidates. To this end, several proposed solutions that have been repeatedly suggested by the kidney transplant community deserve further consideration but require improved data reporting for adequate study.6,7,9,10 These data can inform future OPTN proposals to define priorities for kidney multiorgan allocation.
First, the OPTN should report the quantity of kidney-alone candidates passed over during multiorgan allocation, including the frequency with which children, highly allosensitized candidates, or prior living donors lose priority for kidneys that are instead allocated for multiorgan transplants. Such data can inform proposals to prioritize these special groups above multiorgan recipients in the allocation sequence for all or a subset of kidneys.6,9 Formal criteria for eligibility for thoracic–kidney transplants should replace subjectivity in listing, especially as safety-net kidney waitlisting for heart and lung recipients has been proposed. Determining appropriate criteria will require OPTN reporting of dialysis-dependent AKI, GFR trajectory, kidney failure, and death after non-kidney transplantation in recipients with varying degrees of pretransplant kidney dysfunction, perhaps through integration with the United States Renal Data System and large observational data consortia. These data can also reassure centers that thoracic transplant candidates not meeting multiorgan listing criteria are at low risk of kidney-related adverse events. Given that initial eligibility criteria will be developed in the absence of high-quality evidence, ongoing prospective monitoring of the proportion of candidates who use safety-net allocation and kidney function for single-organ and multiorgan recipients must be collected to allow iterative refinement of these thresholds. The identification of excessively permissive multiorgan eligibility criteria may be challenging absent simple methods of ascertaining native kidney function recovery and will likely rely on comparing observed post-transplant kidney function and kidney graft survival to modeled values expected in the absence of native kidney function improvement. Finally, the OPTN/Scientific Registry of Transplant Recipients must develop ways to appropriately incorporate multiorgan recipients into center performance evaluations.6 Although such evaluations may be challenging because of the small number of multiorgan transplants each center performs, using Bayesian analyses tailored to low-volume programs—as has been performed for kidney transplant programs—might be a first step toward remedying this omission. Regardless, improving the reporting of such data is the first step toward ensuring balance in access to deceased donor kidneys for both kidney-alone and multiorgan candidates.
DisclosuresP.M. Anand reports consultancy for CareDx, Natera, and Veloxis; stock in CareDx; research funding from CareDx and Natera; honoraria from Calliditas, CareDx, Natera, and Veloxis; advisory or leadership roles for Natera and Veloxis; and speakers bureau for Caredx, Natera, and Veloxis. R.D. Bloom reports consultancy for Veloxis Pharmaceuticals; ownership interest in Gilead Pharmaceuticals; research funding from CareDx, CSL Behring, Natera, and Veloxis; honoraria from Nephrosant, Paladin Labs, and Veloxis; royalties from UpToDate; advisory or leadership roles for Nephrosant, Paladin Labs, and Veloxis; and role on the Editorial Board of the American Journal of Kidney Diseases. B. Hippen reports serving as Senior Vice President for Transplant Medicine and Emerging Capabilities, Global Medical Office, Fresenius Medical Care; reports ownership interest in Interwell Health; and reports serving as a Scientific Advisory Board member for eGenesis Bio (uncompensated). S.A. Husain reports research funding from Nelson Family Foundation and honoraria from Fresenius. K.L. Lentine reports consultancy for CareDx, Inc., ownership interest in CareDx, Inc., and speaker honoraria from Sanofi. K.L. Lentine is a Senior Scientist of the SRTR, receives research funding related to transplant from the National Institutes of Health (R01DK120551), and is supported by the Mid-America Transplant/Jane A. Beckman Endowed Chair in Transplantation. K.L. Lentine is chair of the AST Living Donor Community of Practice, a member of the ASN policy and Advocacy Committee, and a member of the National Kidney Foundation Transplant Advisory Committee. R.F. Parsons reports ownership interest in AMZN, CRM, and DIS. N. Singh reports employment with Willis Knighton Health System, Shreveport, LA; research funding from CareDx and Transplant Genomics; honoraria from Mallinckrodt, Natera, and Veloxis; advisory or leadership roles as AST KPCOP Co-Chair and OPTN Pancreas Committee Member; and speakers bureau for Mallinckrodt, Natera, and Veloxis Pharmaceutics. The remaining author has nothing to disclose.
FundingThis work was supported by NIDDK from K23 DK133729 and Nelson Family Foundation from Faculty Development Grant (S.A. Husain).
AcknowledgmentsThis manuscript is a work product of the American Society of Transplantation's Kidney Pancreas Community of Practice Public Policy Working Group.
The data reported here have been supplied by the United Network for Organ Sharing as the contractor for the Organ Procurement and Transplantation Network. The interpretation and reporting of these data are the responsibility of the author(s) and in no way should be seen as an official policy of or interpretation by the OPTN or the US Government.
The content of this article reflects the personal experience and views of the author(s) and should not be considered medical advice or recommendation. The content does not reflect the views or opinions of the American Society of Nephrology (ASN) or CJASN. Responsibility for the information and views expressed herein lies entirely with the author(s).
Author ContributionsConceptualization: Prince Mohan Anand, Roy D. Bloom, Benjamin Hippen, S. Ali Husain, Krista L. Lentine, Ronald F. Parsons, Neeraj Singh.
Data curation: S. Ali Husain.
Formal analysis: S. Ali Husain.
Writing – original draft: Prince Mohan Anand, Roy D. Bloom, Benjamin Hippen, S. Ali Husain, Krista L. Lentine, Ronald F. Parsons, Neeraj Singh.
Writing – review & editing: Prince Mohan Anand, Roy D. Bloom, Benjamin Hippen, S. Ali Husain, Krista L. Lentine, Ronald F. Parsons, Neeraj Singh.
References 1. Wolfe RA, Ashby VB, Milford EL, et al. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med. 1999;341(23):1725–1730. doi:10.1056/nejm199912023412303 2. Mange KC, Joffe MM, Feldman HI. Effect of the use or nonuse of long-term dialysis on the subsequent survival of renal transplants from living donors. N Engl J Med. 2001;344(10):726–731. doi:10.1056/nejm200103083441004 3. Sokas C, Cooper Z, Salim A, Rodrigue JR, Adler JT. Wait expectations: the impact of delisting as an outcome from the kidney transplant waitlist. Clin Transplant. 2021;35(5):e14250. doi:10.1111/ctr.14250 4. Organ Procurement and Transplantation Network. Identify Priority Shares in Kidney Multi-Organ Allocation. Accessed April 17, 2023. https://optn.transplant.hrsa.gov/policies-bylaws/public-comment/identify-priority-shares-in-kidney-multi-organ-allocation/ 5. Parsons RF, Matar A, Lentine KL, et al. Pancreas transplantation perceptions and practice: results from a national US survey. Clin Transplant. 2021;35(10):e14432. doi:10.1111/ctr.14432 6. Reese PP, Veatch RM, Abt PL, Amaral S. Revisiting multi-organ transplantation in the setting of scarcity. Am J Transplant. 2014;14(1):21–26. doi:10.1111/ajt.12557 7. Westphal SG, Langewisch ED, Robinson AM, et al. The impact of multi-organ transplant allocation priority on waitlisted kidney transplant candidates. Am J Transplant. 2021;21(6):2161–2174. doi:10.1111/ajt.16390 8. Khush KK, Hsich E, Potena L, et al. The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: thirty-eighth adult heart transplantation report—2021; focus on recipient characteristics. J Heart Lung Transplant. 2021;40(10):1035–1049. doi:10.1016/j.healun.2021.07.015 9. Westphal SG, Langewisch ED, Miles CD. Current state of multiorgan transplantation and implications for future practice and policy. Adv Chronic Kidney Dis. 2021;28(6):561–569. doi:10.1053/j.ackd.2021.09.012 10. Cheng XS, Reese PP. Incorporating kidney-related multi-organ transplants into the kidney allocation sequence. Am J Transplant. 2021;21(7):2614–2615. doi:10.1111/ajt.16542
Comments (0)