
Remember me



The coronavirus disease 2019 (COVID-19) pandemic, which began in the United States in early 2020, brought unprecedented challenges to the solid-organ transplantation community worldwide.1 Kidney transplant activity in the United States decreased initially, but quickly recovered with gradual increases in utilization of organs from donors with COVID-19.2–7 Early experience revealed the safety of transplanting organs from donors who had recovered from COVID-19.8–10 Clinical practice in many centers soon evolved toward transplanting kidneys from severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) RNA-positive donors and from those who died of COVID-19.11–17 To date, despite evidence suggesting that SARS-CoV-2 infects not only the lung but also extrapulmonary organs,18–21 no COVID-19 transmission has been reported from infected donors to negative recipients of non-lung solid-organ transplants.
In addition to the reported safety of transplanting kidneys from donors with COVID-19, case reports and series have provided some evidence for good short-term recipient outcomes.11–16 Moreover, large-scale studies using the US Organ Procurement and Transplantation Network database have revealed graft and patient survival of recipients of kidneys from SARS-CoV-2 RNA-positive donors that were comparable with those from SARS-CoV-2 RNA-negative donors.4–6,22 However, a more recent single-center retrospective study revealed acceptable but worse short-term graft function for recipients of kidneys from SARS-CoV-2 RNA-positive donors with COVID-19–related cause of death compared with those from SARS-CoV-2 RNA-negative donors.23 Post-transplant follow-up in this single-center study was limited to <6 months, and potential confounders were not sufficiently addressed in these analyses, indicating the need for comparative studies with well-matched controls to better elucidate outcomes. We, therefore, established the multicenter COnsortium to study SARS-CoV-2 VIrus–infecteD DONOR kidney transplants to prospectively evaluate transplant outcomes for recipients of kidneys from SARS-CoV-2–infected donors compared with highly similar kidney recipients from SARS-CoV-2–negative donors. We hypothesized that short-term outcomes, including 6-month post-transplant eGFR, are similar between the groups.
Methods CohortThis multicenter, prospective observational cohort study was designed to assess the safety, potential complications, and short- and long-term outcomes of kidney transplantation from SARS-CoV-2–infected deceased donors. The three participating transplant centers are University of Utah; University of Tennessee Health Science Center, Methodist University Hospital; and Virginia Commonwealth University. This study included recipients aged 18 years or older. We prospectively collected SARS-CoV-2–infected deceased-donor data, including SARS-CoV-2 nucleic acid amplification test results, chest X-ray and computed tomography findings, vaccination status, COVID-19 symptoms and treatments, history of venous thromboembolism, hepatitis C virus nucleic acid tests, and length of hospital stay. We collected clinical information for the recipients of those kidneys, including SARS-CoV-2–related data (SARS-CoV-2 nucleic acid test, anti-spike IgG, vaccination status, prophylaxis, history of COVID-19, post-transplant COVID-19, and venous thromboembolism) and transplant-related data (e.g., induction and maintenance immunosuppression; preexisting donor-specific antibody; graft type; multiorgan transplantation; and history of diabetes, hypertension, cancer, peripheral vascular disease, coronary artery disease, and cerebrovascular disease). Data were extracted from electronic medical records and local transplant datasets and were managed/stored in the Research Electronic Data Capture tool hosted by the University of Utah.
The Institutional Review Board for each participating center approved the study (IRB_00147596). Informed consent was obtained from all participants before enrollment. The research was conducted in accordance with the Declaration of Helsinki.
Data Source and Study PopulationThis study also used each participating center's Standard Transplant Analysis and Research files, which are patient-identified datasets containing information about transplant recipients, deceased and living donors, and waiting-list candidates at individual transplant centers. To compare post-transplant outcomes between recipients of kidneys from SARS-CoV-2–infected and noninfected donors, we extracted deceased-donor kidney transplant data for recipients at each center from January 1, 2016, to May 15, 2022 (Figure 1). Donor/kidney data included age, sex, history of diabetes and hypertension, cause of death, donation after cardiac death, Kidney Donor Profile Index (KDPI) referenced to the 2021 Organ Procurement and Transplantation Network donor population,24 use of kidney hypothermic machine perfusion, terminal serum creatinine, and glomerulosclerosis at organ recovery by biopsy reports. The following recipient data were also collected: age, sex, race, body mass index, previous solid-organ transplantation, dialysis duration, cause of kidney failure, calculated panel reactive antibody (cPRA), human leukocyte antigen mismatch, and cold ischemia time.
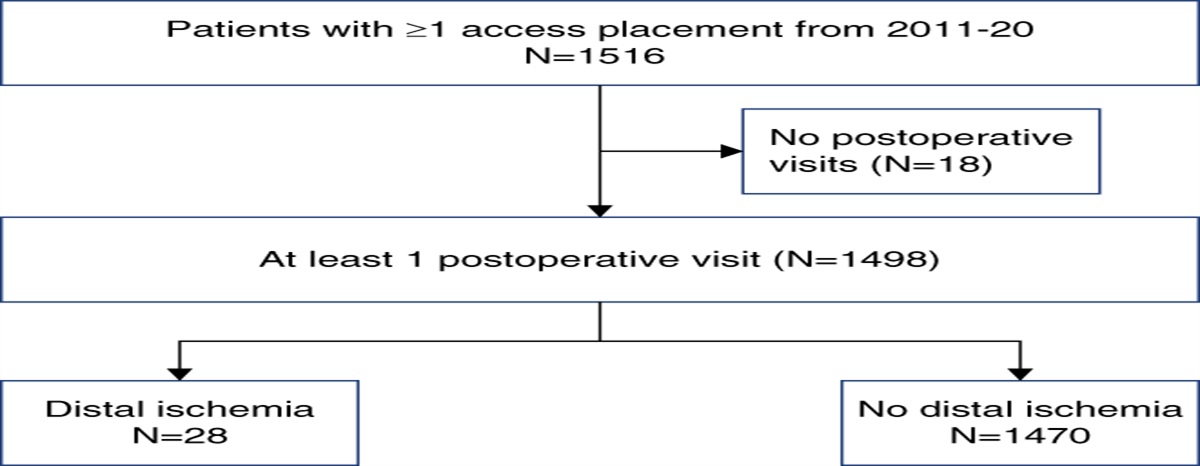
 Figure 1:
Figure 1: Flow chart for matching. COVID-19, coronavirus disease 2019; COVID-death donor, a donor who died of COVID-19; non-COVID–death donor, a donor who died of causes other than COVID-19; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
Donor/Recipient Selection Criteria and Protocols for Transplanting Kidneys from SARS-CoV-2–Infected Deceased DonorsThis observational study did not stipulate selection criteria or protocols for participating center practice; each center followed its own clinical procedures and policies for accepting and transplanting kidneys from SARS-CoV-2–infected deceased donors (Supplemental Methods). Briefly, University of Utah initially only considered deceased donors with SARS-CoV-2 nucleic acid test cycle threshold values >30 and death from causes other than COVID-19. After the first few successful transplants, University of Utah stopped excluding donors because of specific COVID-19 histories. Virginia Commonwealth University only considered asymptomatic SARS-CoV-2 nucleic acid test–positive donors for the first few cases, but thereafter also accepted symptomatic donors. University of Tennessee only considered donors who had not died of active COVID-19. In all centers, kidneys from SARS-CoV-2–positive donors were transplanted only for recipients who at least verbally consented to receive such kidneys and had completed a primary COVID-19 vaccine series. All kidney recipients from donors with positive SARS-CoV-2 nucleic acid tests were eligible for this study. All centers used their standard transplant procedures and immunosuppression protocols. University of Utah and University of Tennessee used rabbit antithymocyte globulin for induction immunosuppression. Virginia Commonwealth University initially only used basiliximab for induction in the first several transplants and followed their standard induction protocols thereafter (rabbit antithymocyte globulin or basiliximab). Standard triple maintenance immunosuppression was used by all centers and consisted of calcineurin inhibitors, mycophenolic acid/mycophenolate mofetil, and prednisone. University of Utah used belatacept instead of calcineurin inhibitors according to its protocol, regardless of donor COVID-19 status (i.e., belatacept was administered to recipients of kidneys from donors who were considered at high risk of severe acute tubular necrosis on the basis of certain conditions [terminal serum creatinine >2 mg/dl, donation after cardiac death, off-pump kidney graft, and/or cold ischemia time >24 h]). University of Utah administered apixaban postoperatively for 1 month because of concern about the higher risk of thromboembolism reported in recipients of kidneys from donors with COVID-19.16
Exposure VariablesThe primary exposure was deceased-donor SARS-CoV-2 infection status. SARS-CoV-2–infected status was determined by nucleic acid amplification testing obtained during the usual care of the donor by the organ procurement organization. A donor was considered SARS-CoV-2–infected if at least one SARS-CoV-2 nucleic acid test result was positive during the donation hospital stay. For matched analyses, donors were defined as SARS-CoV-2–noninfected if they never had SARS-CoV-2 nucleic acid test positivity. All potential donors received testing for SARS-CoV-2.
Outcome VariablesThe primary outcome was 6-month recipient eGFR by the serum creatinine–based Chronic Kidney Disease Epidemiology Collaboration 2021 equation.25 Secondary outcomes were delayed graft function, defined as any dialysis within the first week after transplant, length of hospital stay, 6-month graft and patient survival, rejection within 6 months, donor-to-recipient SARS-CoV-2 transmission, and thromboembolic events in recipients of kidneys from SARS-CoV-2–infected donors. Donor-to-recipient SARS-CoV-2 transmission was defined as a positive nucleic acid test/development of COVID-19 within 10 days after transplant.
Matching ProcessUsing optimal matching methods, we matched every patient (“donor SARS-CoV-2–infected”) to three comparators (“donor SARS-CoV-2–negative”) within each center (Figure 1). Matching was performed in an iterative process to ensure that patients and matched comparators were highly similar. A propensity score model was first built using all variables in the matching algorithm. We then built a Mahalanobis distance matrix for important continuous variables (age, KDPI, cold ischemia time, and cPRA), and finally, bipartite cardinality matching was performed to identify optimal pairs. The matching process included recipient factors (age, sex, race, dialysis vintage, cause of kidney failure, history of prior transplant, and cPRA), donor factors (donation after cardiac death, KDPI, and kidney pumped), and transplant factors (human leukocyte antigen mismatch and cold ischemia time). We used mean constraint to balance continuous variables and fine-balance to match categorical variables. Balance was assessed using absolute standardized differences (cutoff <0.1) and visual inspection of distribution plots. Study outcomes were examined only after balance was assessed by study investigators (V.P., M.Z.M., I.E.H., and J.Y.) and the match was finalized. Optimal matching and balance assessment was performed using R statistical software (R Foundation for Statistical Computing version 4.2.2, and packages “designmatch” and “cobalt”).
Statistical AnalysisBaseline characteristics are presented as mean and SD or median and interquartile range for continuous variables and number and percentage for categorical variables, as appropriate. We used the generalized Wilcoxon–Mann–Whitney rank-sum test to compare recipient 6-month eGFR between the matched SARS-CoV-2–infected and negative donor groups. As a subgroup analysis, we also compared recipient 6-month eGFR by primary exposure stratified by donor death either directly caused by COVID-19 (COVID-death) or other causes (non-COVID–death). Differences in donor and recipient characteristics between the COVID-death and non-COVID–death donor groups were analyzed using t-tests or Mann–Whitney U tests for continuous variables and Fisher exact tests for categorical variables. P values were two-sided and considered statistically significant when <0.05 for all analyses. All analyses, except matching, were conducted using STATA version 17 (STATA Corporation, College Station, TX).
Results Description of Kidney Transplantation from SARS-CoV-2–Infected DonorsWe enrolled 61 recipients of kidneys from 52 SARS-CoV-2–infected donors (Table 1). The median (interquartile range) donor age was 38 (29–51) years, 15 recipients (29%) were female, and 13 (25%) had died of COVID-19. Median KDPI and terminal serum creatinine were 42 (25–65) and 0.9 (0.5–1.3) mg/dl, respectively. COVID-19 symptoms that were reported in donors included cough (25%), fever (14%), and dyspnea (20%); 45% of donors had no symptoms. Two donors (4%) developed pulmonary embolism after COVID-19 onset. Median time from COVID-19 symptom onset to organ procurement was 26 (17–32) days. SARS-CoV-2 cycle threshold was available in 28 donors, with the median lowest value of 33.4 (28.5–37.3) and range of 12.5–44.8. Typical chest X-ray and computed tomography changes consistent with COVID-19 were observed in 71% and 51% of these donors, respectively. Compared with SARS-CoV-2–infected but non-COVID–death donors, COVID-death donors were older (33 [21–46] versus 53 [48–54] years) and more likely donated after cardiac death (21% versus 69%; Supplemental Table 1). Median KDPI was higher in COVID-death donors (37 [19–66] versus 46 [39–57]). The degree of glomerulosclerosis was 0%–5% in 34 of 38 biopsy reports (89%; 85% [11/13] and 92% [23/25] in COVID-death and non-COVID–death donors, respectively).
Table 1 - Baseline characteristics of severe acute respiratory syndrome coronavirus 2–positive donor kidney transplant Donor Characteristic Total (n=52) Age, yr 39 (29–51) Sex, n (%) Male 37 (71) Female 15 (29) Race, n (%) Black 7 (13) White 37 (71) Others 8 (15) Diabetes, n (%) 5 (10) Hypertension, n (%) 9 (18) Positive HCV nucleic acid test status, n (%) 7 (13) Kidney Donor Profile Index, % 42 (25–65) COVID-19 as the cause of death, n (%) 13 (25) Cause of death, n (%) Anoxia 27 (52) Cerebrovascular/stroke 7 (13) Head trauma 14 (27) Others 4 (8) Recovery type, n (%) Donation after cardiac death 17 (33) Donation after brain death 35 (67) Donor kidney on pump 34 (65) Terminal serum creatinine, mg/dl 0.9 (0.5–1.3) Length of hospital stay, d 4 (2–10) Glomerulosclerosis in kidney biopsy at organ recovery, n (%)a 0%–5% 34 (89) 6%–10% 3 (8) 11%–15% 1 (3) COVID-19 symptoms, n (%) Cough 13 (25) Fever 7 (14) Dyspnea 10 (20) No symptoms 23 (45) Unknown 9 (18) Time since symptom onset to donation, db 26 (17–32) Treatment for COVID-19, n (%) Remdesivir 3 (6) Steroids 2 (4) None 30 (59) Unknown 15 (29) History of venous thromboembolism 2 (4) Type of venous thromboembolism Pulmonary embolism 2 (100) Time since venous thromboembolism to donation, d 10, 22 SARS-CoV-2 nucleic acid amplification testc Lowest cycle threshold 33.4 (28.5–37.3) Source of sample, n (%) Nasopharyngeal 24 (86) Bronchoalveolar lavage 4 (14) Typical chest X ray changes for COVID-19 (opacities/infiltrates), n (%) 36 (71) Typical chest CT changes for COVID-19 (opacities/infiltrates), n (%)d 24 (50) Prior COVID-19 vaccination, n (%) No 9 (17) Yes 7 (13) Unknown 36 (69) Recipient Characteristic Total (n=61) Age, yr 53 (44–63) Sex, n (%) Male 40 (66) Female 21 (34) Body mass index, kg/m2 29.9 (24.9–34.0) Race, n (%) Black 32 (52) White 19 (31) Others 10 (16) Cause of kidney failure, n (%) Diabetes 24 (39) Hypertension 15 (25) Glomerulonephritis 8 (13) Cystic disease 2 (3) Others 12 (20) Pretransplant Dialysis, n (%) Preemptive 9 (15) ≤ 1 yr 4 (7) 1–3 yr 19 (31) 3–5 yr 19 (31) >5 yr 10 (16) Length of dialysis, m 42 (22–56) Prior transplant, n (%) 3 (5) Multiorgan transplant, n (%) 2 (3) Diabetes, n (%) 34 (56) Hypertension, n (%) 60 (98) Cancer, n (%) 7 (11) Peripheral vascular disease, n (%) 9 (15) Coronary artery disease, n (%) 16 (26) Cerebrovascular disease, n (%) 3 (5) Calculated PRA 0 (0–0) Human leukocyte antigen mismatch, n (%) 0 1 (2) 1 0 (0) 2 2 (3) 3 9 (15) 4 22 (36) 5 19 (31) 6 8 (13) Preexisting donor-specific antibody, human leukocyte antigen class I, n (%) 0 (0) Preexisting donor-specific antibody, human leukocyte antigen class II, n (%) 3 (5) Cold ischemia time, h 23 (18–30) Graft type, n (%) Single 55 (90) Dual 1 (2) En bloc pediatric 3 (5) Other 2 (3) Induction immunosuppression, n (%) Antithymocyte globulin 54 (89) Basiliximab 7 (11) Maintenance immunosuppression at discharge, n (%) Tacrolimus 51 (84) Cyclosporine 1 (2) Mycophenolate 59 (97) Steroids 59 (97) Belatacept 9 (15) COVID-19–related, n (%) History of COVID-19 infection 6 (10) Pretransplant COVID-19 vaccination 61 (100) Vaccine dose, n (%) 1 2 (3) 2 29 (48) 3 28 (46) 4 2 (3) Anti-spike IgG, positive, n (%)e 34 (94) COVID-19 prophylaxis after transplant, n (%) Remdesivir 30 (49) Tixagevimab/cilgavimab 40 (66)Values are expressed as median (interquartile range) or number (%). HCV, Hepatitis C virus; COVID-19, coronavirus disease 2019; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; CT, computed tomography; PRA, panel reactive antibody.
aData for glomerulosclerosis were available in 38 SARS-CoV-2–positive donor kidneys. As a reference, 100 kidney biopsy reports of 183 SARS-CoV-2–negative donors (matched control in this study) were available. The degree of glomerulosclerosis was 0%–5% in 76 (76%), 6%–10% in 17 (17%), 11%–15% in five (5%), and 16%–20% in two (2%) kidneys.
bData for time since symptom onset to donation were available in 19 donors.
cData for lowest cycle threshold and source of sample were available in 28 donors.
dData for typical chest CT changes for COVID-19 were available in 48 donors.
eData for anti-spike IgG were available in 36 recipients.
The median recipient age was 53 (44–63) years, 34% recipients were female, 52% were Black, and 31% were White (Table 1). Two of the 61 recipients (3%) underwent simultaneous kidney–pancreas transplant; all others received kidney-only transplants. The median cold ischemia time was 23 (18–30) hours. Antithymocyte globulin induction was used in 89%; 11% received basiliximab. At discharge, 84% received tacrolimus for maintenance immunosuppression, 2% (one recipient) received cyclosporine, and 15% initiated belatacept. Compared with recipients from non-COVID–death donors, those from COVID-death donors were less frequently administered tacrolimus (91% versus 60%) and more frequently administered belatacept (7% versus 40%), reflecting more frequent donations after cardiac death, higher KDPI, and longer cold ischemia time (Supplemental Table 1). Ninety-seven percent of recipients were also discharged on mycophenolate and steroids. All 61 recipients had been vaccinated against SARS-CoV-2 before transplant, with 97% having received at least two doses of mRNA vaccines. Thirty-four of the 36 recipients (94%) tested positive for anti-spike IgG during their transplant hospitalization. Remdesivir was used prophylactically in 49%. Tixagevimab/cilgavimab was administered after transplant in 66% of recipients.
Mean 6-month eGFR was 55±21 ml/min per 1.73 m2 and was lower in recipients of kidneys from COVID-death donors than from non-COVID–death donors (46±17 versus 58±22 ml/min per 1.73 m2; Table 2 and Supplemental Table 2). Delayed graft function occurred in 22 recipients (36%), and median length of hospital stay was 5 (4–6) days. There were no death-censored graft losses by 6 months after transplant, although one recipient (2%) died with a functioning graft 42 days after transplant because of respiratory failure secondary to volume overload, pneumonia, and procedure-associated tachyarrhythmia. One recipient (2%), who received tacrolimus, experienced acute antibody-mediated rejection. Nine recipients (15%) subsequently developed COVID-19; however, all cases occurred beyond 10 days after transplant and were determined not to be donor-derived. One recipient (2%), who did not have COVID-19, developed pulmonary embolism 52 days after transplant. Of 45 recipients who underwent SARS-CoV-2 nucleic acid testing within 30 days after transplant, only one, who notably had a positive test before transplant, tested positive 6 days after transplant. This recipient was confirmed negative 12 days after transplant and never experienced COVID-19 symptoms. Except for 6-month eGFR (see below), post-transplant outcomes were similar between recipients from COVID-death donors and those from non-COVID–death donors.
Table 2 - Recipient outcomes of severe acute respiratory syndrome coronavirus 2–positive donor kidney transplantation Recipient Outcome Total (n=61) eGFR at 6 mo, ml/min per 1.73 m2 55 (21) Delayed graft function, n (%) 22 (36) Length of hospital stay, d 5 (4–6) Graft loss within 6 mo, n (%) 0 (0) Death within 6 mo, n (%) 1 (2) Rejection within 6 mo, n (%) 1 (2) Post-transplant COVID-19 infection, n (%) 9 (15) Donor-derived COVID-19 infection, n (%) 0 (0) Post-transplant venous thromboembolism, n (%) 1 (2) Type of venous thromboembolism, n (%) Pulmonary embolism 1 (100) Time since transplant to venous thromboembolism, d 52 SARS-CoV-2 nucleic acid amplification test within 30 d after transplant, n (%)a Positive 1 (2) Negative 44 (98) Time since transplant to testing, d 7 (3–10) Source of sample, n (%) Nasopharyngeal 38 (84) Blood 3 (7) Saliva 4 (9)Values are expressed as mean (SD), median (interquartile range), or number (%). COVID-19, coronavirus disease 2019; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
aData for SARS-CoV-2 nucleic acid amplification test within 30 days after transplant were available in 45 recipients.
Figure 1 shows the cohort generation. In the prematched cohort, 61 recipients of kidneys from SARS-CoV-2–infected donors were similar in age, race, and preemptive transplantation compared with 2517 recipients from SARS-CoV-2–negative donors (Table 3). Recipients in the SARS-CoV-2–infected donor group had lower cPRA and prior transplant frequency. KDPI was similar between groups; however, the SARS-CoV-2–infected donor group had a higher proportion of cardiac death and longer cold ischemia time. After matching, all adjusted characteristics were very well balanced with small standardized mean differences and similar distribution plots (Supplemental Figure 1).
Table 3 - Distribution of covariates used in the matching algorithm Characteristics Pre-Match Post-Match Standardized Difference Donor SARS-CoV-2–Positive (n=61) Donor SARS-CoV-2–Negative (n=2517) Donor SARS-CoV-2–Positive (n=61) Donor SARS-CoV-2–Negative (n=183) Pre-Match Post-Match Recipient variables Age, yr 54 (13) 52 (13) 54 (13) 54 (13) −0.09799 0.00041 Female, n (%) 21 (34) 1022 (41) 21 (34) 63 (34) 0.12733 0 Race—Black, n (%) 32 (53) 1363 (54) 32 (53) 96 (53) 0.03379 0 Transplant center, n (%) Center 1 20 (33) 631 (25) 20 (33) 60 (33) −0.17004 0 Center 2 9 (15) 823 (33) 9 (15) 27 (15) 0.43015 0 Center 3 32 (53) 1063 (42) 32 (53) 96 (53) −0.20501 0 Duration on dialysis, n (%) Preemptive 9 (15) 370 (15) 9 (15) 27 (15) −0.00152 0 <1 yr 4 (7) 160 (6) 4 (7) 12 (7) −0.00813 0 1–3 yr 19 (31) 576 (23) 19 (31) 57 (31) −0.18604 0 3–5 yr 19 (31) 594 (24) 19 (31) 57 (31) −0.16912 0 >5 yr 10 (16) 817 (33) 10 (16) 30 (16) 0.37938 0 Cause of kidney failure, n (%) Diabetes 24 (39) 879 (35) 24 (39) 72 (39) −0.09122 0 Hypertension 15 (25) 734 (29) 15 (25) 45 (25) 0.10284 0 Glomerulonephritis 8 (13) 236 (9) 8 (13) 24 (13) −0.11797 0 Cystic disease 2 (3) 138 (6) 2 (3) 6 (3) 0.10749 0 Other/missing 12 (20) 530 (21) 12 (20) 36 (20) 0.03425 0 Prior transplant 3 (5) 252 (10) 3 (5) 9 (5) 0.1
Comments (0)