
Remember me



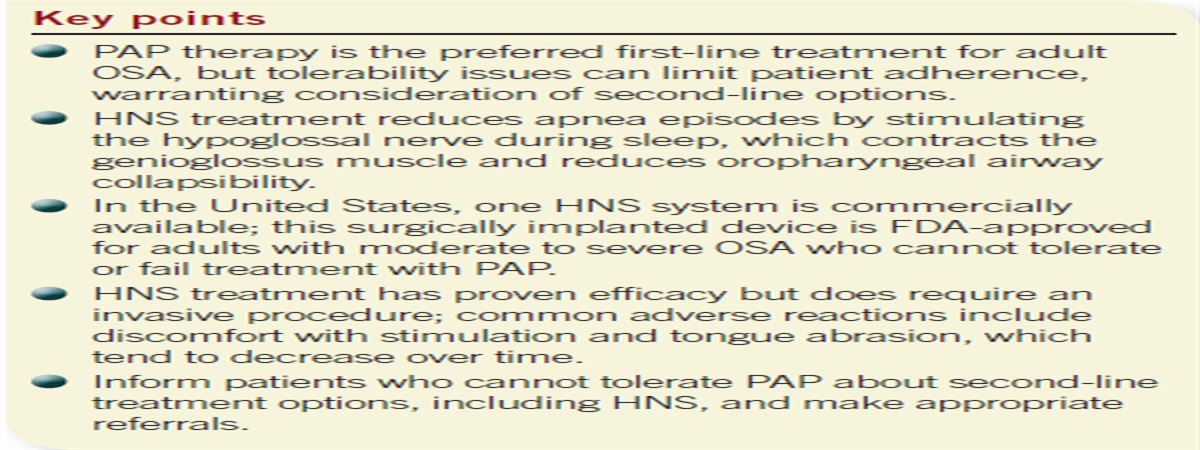

Access to mental health resources for physician associates/assistants (PAs) is an important topic. Although considerable literature on mental health and access to care exists for physicians and RNs, data on PAs and allied health professionals are scarce. Multiple studies found that about half of physicians were experiencing burnout—and that was before the COVID-19 pandemic.1 Burnout is associated with a variety of unfavorable patient outcomes, as well as increased unhealthful use of alcohol and suicidal ideation among physicians.1 Burnout in PAs is also well established and occurs at a rate similar to that of physicians, but minimal data exist on other facets of the mental health of PAs.2-4 A 2021 study found that 6% of PA respondents met screening criteria for depression, and an additional 12.6% met screening criteria for moderate or severe anxiety (N = 880).4 Another recent study identified suicidal ideation in about 4% of PAs (N = 322) and 10% of PA students (N = 728).5 Although peer-reviewed studies about the prevalence of substance use issues among PAs are lacking, research has found that 8% to 15% of physicians experience substance use disorder (SUD).6 Despite high rates of burnout and mental illness among clinicians across these healthcare professions, concerns about perceived stigma, lack of time, probing licensure questions (such as Have you ever been diagnosed with chemical dependency or addiction?), and confidentiality often are cited as barriers to seeking appropriate care.7
To address these barriers, the American Academy of Physician Associates (AAPA) policy manual contains a section on PA impairment and wellness, with recommendations for PA licensing boards concerning questions about mental health. The AAPA suggests that licensing boards “share information about provider health programs (PHPs), services offered through professional societies, and any other relevant programs.”8 PHPs are confidential support programs for clinicians experiencing impairment due to physical or mental health issues and/or SUD. The policy manual recommends that licensing boards provide information about PHPs.8 These recommendations are largely derived from research, policies, and organizations for physicians (for example, the Federation of State Medical Boards).9 Peer-reviewed studies on PHPs are sparse but have found that PHPs are effective, with about 75% of participants having favorable outcomes at 5 years, as well as lower risk of malpractice claims.10,11
Recent studies have shown that only 18 states follow guidance from the Federation of State Medical Boards for questions about mental health on initial and/or renewal licensure applications, and that PAs in states that ask probing mental health questions are less likely to seek help for mental health issues or SUD.12,13 With so few states in compliance with guidance on best practices for licensure questions, there is cause for concern that many states will not adequately support PAs who may experience impairment. Given the scope of both burnout and mental health issues in the PA profession, this is an important target for advocacy efforts.
No literature is available on the prevalence of PHPs for PAs. Further, the landscape of accessible information about PHPs has not been studied. This study sought to assess the availability of PHPs as well as the accessibility of information about these resources through state licensing board and PA constituent organization websites.
METHODSData were collected through audits of the websites of the PA licensing board and state/district constituent group for each state and the District of Columbia from October to November 2022. Information from the Federation of State Physician Health Programs and additional Internet searches were used to ascertain whether a state had a PHP. This audit consisted of one researcher reviewing the websites in their entirety to identify whether information about a PHP for PAs was provided. Instances where this information was limited or unclear were clarified with discussion between the two researchers and (where necessary) a telephone call and/or email to the organization in question. The data collection scheme is shown in Table 1, along with the results for each item.
TABLE 1. - Data collection scheme with frequency of results collected regarding PHPs across all states and the District of Columbia Variable Data Frequency (%) Is there a PHP serving PAs? Yes 50 (98%) No 1 (2%) Does the PHP use physician-centered language? Yes 19 (38%) No 31 (62%) Is PHP information on the website of the state's constituent organization? Yes 9 (18%) No 41 (82%) Is PHP information on the website of the state's PA licensing agency? Yes 23 (46%) No 27 (54%)All 50 states and the District of Columbia were included in this study and are called states in this study for ease of readability. Every state except Massachusetts has a PHP that serves PAs. Of the 50 PHPs, 19 (38%) provide information using physician-centric language such as physician health program. Review of the 51 respective PA licensing board websites revealed that 23 states (45.1%) list PHP information (Figure 1); 9 states (17.6%) list PHP information on state PA constituent organization websites (Figure 2).
 FIGURE 1.:
FIGURE 1.: Availability of information about the state's PHP on the state's PA licensing agency website. Washington, D.C., is not shown on the map. Its licensing agency website does not share PHP information. Massachusetts, which does not have a PHP, is counted as a no.
 FIGURE 2.:
FIGURE 2.: Availability of information about the state's PHP on the state's constituent organization website. Washington, D.C., is not shown on the map. Its constituent organization website shares PHP information. Massachusetts, which does not have a PHP, is counted as a no.
DISCUSSIONAt the time of data collection, all but one state had a PHP in place that served PAs. Massachusetts, the one outlier, passed a law in 2022 mandating the creation of a PHP to serve nonphysician healthcare providers, but it had not been established at the time of data collection. Overall, PHPs are (or will soon be) available to virtually all PAs in the United States.
Unfortunately, most states fail to make the information about their PHP readily available to interested parties on the websites of licensing boards and constituent organizations. This represents an important (and easily addressed) potential barrier to PAs locating and accessing the services of their state's PHP, because PAs experiencing actual or potential impairment may fail to locate the PHP and may conclude that no services exist for them. This concern is augmented by the pervasive stigma surrounding mental health issues and SUD. Some PAs may be reluctant to inquire about resources, often multiple times, to organizations that may have the ability to influence their professional licensure. Making information about PHPs easily accessible on the websites of licensing boards and constituent organizations and clearly stating policies about confidentiality are simple steps to improve awareness and use of these important services.
Another potential barrier is the use of physician-centric language. Renaming organizations that serve various clinical groups using more inclusive language, such as provider health program, would clarify their scope and allow potential clients to identify them more readily as places to seek help.
Beyond the titles of programs and website information, the experience of researching these organizations offered additional findings that may inform future research on factors influencing PA participation in PHPs. One of these variables is the responsiveness of the PHP. Some PHPs responded quickly to questions with personal outreach and earnest attempts to engage the researchers as people potentially in need of help. By contrast, others failed to respond to multiple messages by telephone and email before eventually replying days or weeks later.
One concept that is also included in the AAPA's policy manual is safe haven non-reporting, which protects the confidentiality of participants by allowing clinicians who are receiving treatment for mental health issues or SUD to be licensed without having to disclose their diagnosis or treatment to the licensing board. The review of websites for this study revealed highly varying language on confidentiality, with some states using language that was inviting and supportive, and others being more legalistic or impersonal (Appendix 1,https://links.lww.com/JAAPA/A16). Exploration into how these differences in syntax can improve or diminish the experience of a person exploring the program, and potentially affect use of services, is an important area for future research.
Other elements on websites were a video with information and testimonials from past participants (Tennessee, Utah), a free self-screening tool for healthcare professionals who may be experiencing impairment (Tennessee), and language stating that PA students may use the PHP (Kansas). Many programs also include a list of outside websites and resources as well as contact information for suicide hotlines and other emergency resources. These features and responsive staff are likely to increase the usefulness of these websites for people searching for information and/or help through these organizations.
The results of this study indicate that PHPs for PAs are widely available. However, the broad availability of PHPs is countered by the lack of accessible information about these programs in many states. Efforts to improve this should include prominently displaying information, using PA-inclusive language, and including confidentiality policies on the websites of licensing boards and constituent organizations. Further studies are needed to understand the actual use of PHPs by PAs, the subjective experience of prospective and actual PHP participants, and the place of these programs in the larger context of clinician well-being.
LIMITATIONSWebsites are highly variable in formatting and navigation. The researchers (despite their best efforts) may have failed to find or recognize relevant information on some websites. In some cases, policies may be in place, but the websites have not been updated or the policies or language changed after our review.
CONCLUSIONSPHPs are available for almost all PAs, but most states do not provide information about them on websites for licensing boards or constituent organizations. Improving the accessibility of information about these programs is as simple as updating websites with existing information. This will make it easier for PAs with physical or mental health issues and/or SUD to locate and access help, reducing one known barrier to accessing care.
REFERENCES 1. West CP, Dyrbye LN, Shanafelt TD. Physician burnout: contributors, consequences and solutions. J Intern Med. 2018;283(6):516–529. 2. Coplan B, McCall TC, Smith N, et al. Burnout, job satisfaction, and stress levels of PAs. JAAPA. 2018;31(9):42–46. 3. Essary AC, Bernard KS, Coplan B, et al. Burnout and job and career satisfaction in the physician assistant profession: a review of the literature. NAM Perspect. https://nam.edu/burnout-and-job-and-career-satisfaction-in-the-physician-assistant-profession-a-review-of-the-literature. Accessed July 25, 2023. 4. Blackstone SR, Johnson AK, Smith NE, et al. Depression, burnout, and professional outcomes among PAs. JAAPA. 2021;34(9):35–41. 5. Smith NE, Sierra T, Brown H. Acknowledging suicidal ideation, depression, and anxiety in PAs. JAAPA. 2022;35(12):1. 6. Vayr F, Herin F, Jullian B, et al. Barriers to seeking help for physicians with substance use disorder: a review. Drug Alcohol Depend. 2019;199:116–121. 7. Zaman N, Mujahid K, Ahmed F, et al. What are the barriers and facilitators to seeking help for mental health in NHS doctors: a systematic review and qualitative study. BMC Psychiatry. 2022;22(1):595. 8. American Academy of PAs. 2023-2024 Policy Manual. www.aapa.org/download/116915/?tmstv=1690405277. Accessed August 28, 2023. 9. Federation of State Medical Boards. Physician wellness and burnout: report and recommendations of the Work Group on Physician Wellness and Burnout. www.fsmb.org/siteassets/advocacy/policies/policy-on-wellness-and-burnout.pdf. Accessed July 25, 2023. 10. Brooks E, Gendel MH, Gundersen DC, et al. Physician health programmes and malpractice claims: reducing risk through monitoring. Occup Med (Lond). 2013;63(4):274–280. 11. McLellan AT, Skipper GS, Campbell M, DuPont RL. Five year outcomes in a cohort study of physicians treated for substance use disorders in the United States. BMJ. 2008;337:a2038. 12. Nettesheim E, Neary S, Roman C. Do PA licensure questions violate the Americans with Disabilities Act. JAAPA. 2021;34(3):46–48. 13. Roman C, Neary S, Nettesheim E, Zorn J. PA licensure questions, the Americans with Disabilities Act, and seeking medical care. JAAPA. 2022;35(1):49–52.
Comments (0)