
Remember me

A PRISMA diagram for the identification of studies is shown in Fig. 1. After deduplication across databases, 236 studies were screened at the level of title and abstract. A total of 75 studies were evaluated at the full-text level, after the addition of 10 trials resulting from the search performed on ClinicalTrials.gov. A total of 45 studies were excluded at the full-text level; 17 did not include any outcomes of interest, 12 were linked to another publication with more updated data, 7 clinical trials were captured in the database searches, 4 had no primary data, 3 were in vitro or animal studies, and 2 clinical trials had no results available. Thus, a total of 30 studies were included for abstraction. A total of 13 [6, 10, 15,16,17,18,19,20,21,22,23,24,25] of these 30 studies utilized SP347 assays, which have been both validated and subsequently used in the clinical setting in multiple populations [24], to evaluate DLL3 expression and are the focus of this paper. Details about the remaining 17 papers are provided in Additional files 1–7 for purposes of comparability. Additional file 8 contains the supplementary text that corresponds with Additional files 1–7.
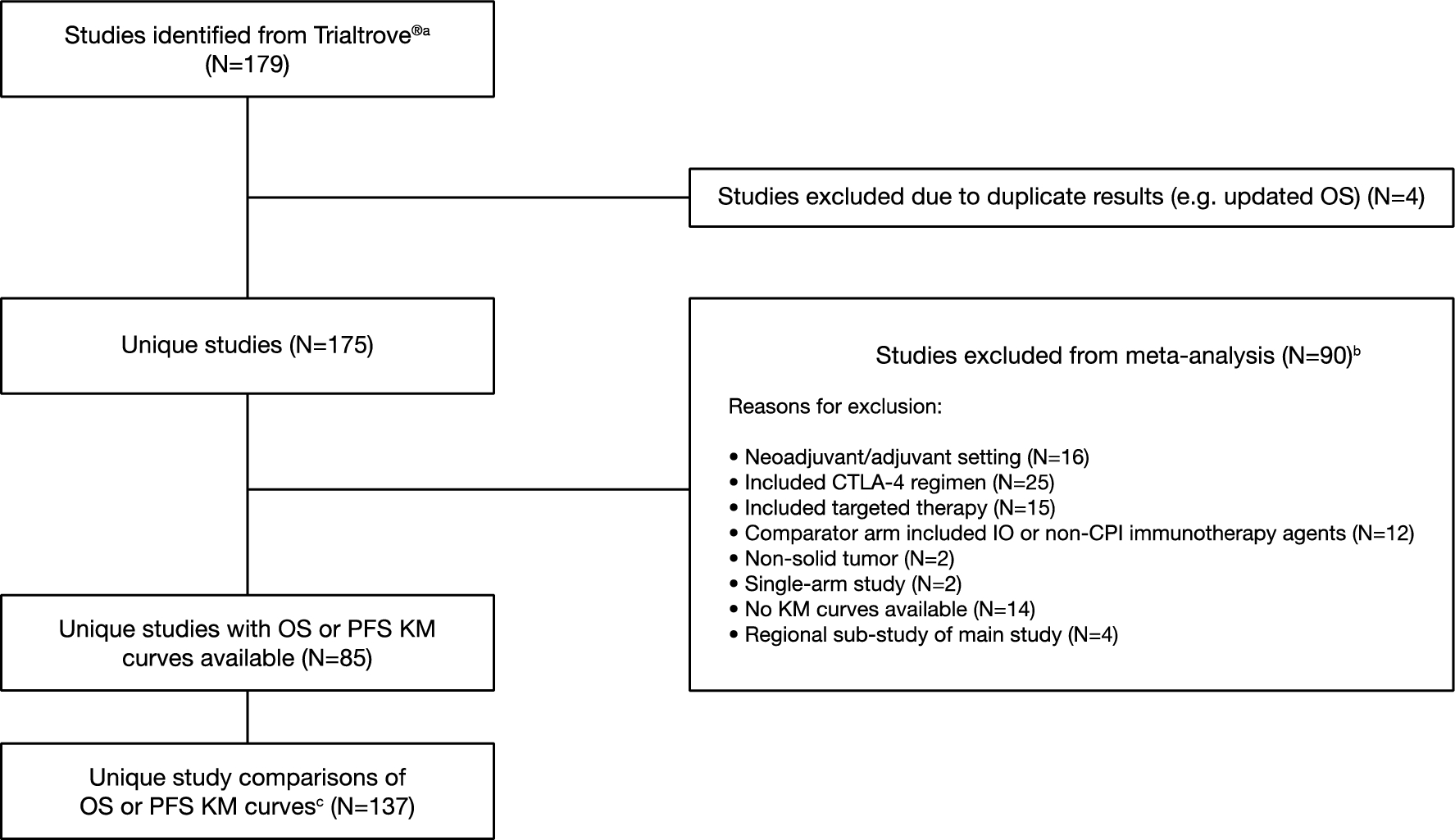
Fig. 1
PRISMA study flow diagram
3.2 Study CharacteristicsThe characteristics of the 30 included studies are presented in Additional file 3. Of the 13 studies using SP347 assays, there were 5 retrospective cohorts [6, 10, 15, 17, 23], 4 cross-sectional studies [16, 21, 24, 25], 2 single-arm trials [20, 22], 1 randomized trial [18], and 1 prospective cohort study [19]. Most (N = 8) studies had less than 100 participants. Study locations were varied; two studies were conducted in the USA [23, 24], two were conducted in Germany [10, 16], two were conducted in Japan [17, 22], and three were conducted in multiple countries [6, 18, 20]. The remaining studies were conducted in Italy [15], Greece [19], Canada [21], and Sweden [25].
3.3 Risk of BiasThe NOS scores of the ten observational studies that used SP347 assays ranged from 3 to 9 with a mean of 6.1 and median of 6. When converted to the AHRQ standards, five studies were scored as good quality [6, 15, 19, 23, 25], three studies were scored as fair quality [16, 21, 24], and two studies were scored as poor quality [10, 17]. When evaluating bias by domain, risk was most apparent in the comparability of cohorts and adequacy of follow-up (Fig. 2A). In the Cochrane RoB scores of the three clinical trials that used SP347 assays, two studies [18, 22] were scored as “high risk” and one study [20] had “some concerns.” Risk was most apparent in the randomization process (Fig. 2B). Details about the remaining 17 papers are provided in Additional file 7.
Fig. 2
Summary of risk of bias scores in A observational studies and B clinical trials. A Risk of bias in observational studies (Newcastle–Ottawa Scale) using SP347 assay (N = 10). B Risk of bias in clinical trials (Cochrane Risk of Bias Tool) using SP347 assay (N = 3)
3.4 Patient and Treatment CharacteristicsPatient and treatment characteristics varied across the studies using the SP347 assay (Additional file 3). The distribution of sex was reported in ten studies, with males ranging from 43% [25] to 84.3% [19]. One study reported race/ethnicity, with 82% of the study population being white [18]. Three studies reported smoking status [6, 15, 17], of which most patients were current/former smokers (range: 85.2% [17] to 100% [15]). Eastern Cooperative Oncology Group (ECOG) performance status was reported in six studies, with the majority of patients having an ECOG status of 1 or 0 in most studies [6, 18, 20, 22, 25]. Six studies reported tumor stage at diagnosis as limited or extensive [6, 15, 19] and/or by tumor, node, metastasis (TNM) stage [15, 17, 18, 20]. Patients with extensive disease at diagnosis ranged from 0% in an Italian cohort of 32 patients with SCLC from 2007–2019 [15] to 63% in a large (N = 1073) multicountry retrospective cohort (2008–2017) [6]; patients with TNM stage III–IV at diagnosis ranged from 11.6% in a retrospective Japanese cohort of 95 patients with SCLC (2003–2013) [17] to 84% in the phase III MERU trial (2017–2019) [18].
DLL3 positivity was determined by the percentage of tumor cell positivity in 13 studies [6, 10, 15,16,17,18,19,20,21,22,23,24,25] and/or H-score in two studies [10, 15]. The threshold for tumor cell positivity ranged from 1–25% and was often classified as “high” or “low” with cut-offs at 50% or 75% of positive tumor cells. The H-score threshold for “high” DLL3 expression was consistent in both studies at 150. All 13 studies reported DLL3 prevalence as an outcome. Other endpoints assessed in the studies included stratification of DLL3 expression by demographic or clinical factors (N = 5), OS (N = 8), progression-free survival (PFS) or disease-free survival (DFS) (N = 5), and treatment response (N = 3).
3.5 Prevalence of DLL3 Expression in SCLC3.5.1 Positive Versus Negative DLL3 ExpressionAll 13 studies using the SP347 assay evaluated the prevalence of DLL3 expression (Table 1). Additional file 4 describes the prevalence of DLL3 expression (N = 15) among non-SP347 assay studies. DLL3 expression was categorized as positive or negative in nine studies using the SP347 assay [6, 10, 16, 17, 20,21,22, 24, 25] and ten non-SP347 studies [26,27,28,29,30,31,32,33,34,35] (Additional file 4). One cross-sectional US study reported 76.4% of patients with SCLC were DLL3-positive, defined as reactivity > 0% [24]. Among four studies using a threshold of ≥ 1% to define DLL3 positivity [10, 17, 21, 25], patients that were DLL3-positive ranged from 80.0% among chemo-relapsed German patients (time period not specified) [10] to 93.5% in patients who had completed at least one cycle of chemotherapy between 2008 and 2015 in Sweden [25]. Of the four studies that used a 25% threshold [6, 16, 20, 22], the prevalence of DLL3 positivity ranged from 58.3% in a cohort of German chemo-naïve surgically resected samples from 1996–2012 [16] to 91.1% in an international clinical trial of 339 adult patients with advanced stage SCLC from 2016 to 2017 [20].
Table 1 Prevalence of DLL3 expression in the tissue of patients with SCLC using SP347 assay (N = 13)3.5.2 High Versus Low DLL3 ExpressionDLL3 expression was broadly categorized as “high” or “low” in 12 SP347 studies [6, 10,
Comments (0)