
Remember me




The term assisted fall is a relatively new name for an old phenomenon. In U.S. health care settings, it refers to a patient fall event in which “any staff member (whether a nursing service employee or not) . . . attempt[s] to minimize the impact of the fall by slowing the patient's descent” to the ground or another stable surface.1 Several secondary data analyses have demonstrated that, compared to unassisted falls, assisted falls are associated with reduced patient injury and injury severity.2, 3 But other research suggests that assisted falls may contribute to occupational injuries among staff, especially musculoskeletal injuries.4 While there is a body of literature on the risk to staff during other forms of patient handling such as lifts and transfers,5, 6 scant research exists concerning patient and staff injury outcomes specifically related to assisted falls. Thus, there is limited evidence-based guidance to help staff assess the risks of assisting falling patients. Given that most patient falls are unwitnessed and unassisted,2, 7-9 it's likely that firsthand accounts of staff-assisted patient falls could provide insight into common fall scenarios and contributing factors.
Beginning in 2020, the Veterans Integrated Services Network 8 Patient Safety Center of Inquiry conducted a quality improvement (QI) project aimed at improving guidance for staff concerning the risks of assisting falling patients in Veterans Affairs (VA) health care facilities, where one-third of all witnessed falls are assisted.10 This article presents the project's qualitative findings regarding the experiences of health care staff with assisted falls.
BACKGROUNDPatient falls are multifactorial and associated with many well-known intrinsic factors (such as comorbidities, functional and cognitive impairments, medication side effects) and extrinsic factors (such as environmental hazards, inadequate use or lack of safe patient handling and mobility [SPHM] equipment).11-16 Although there is an extensive body of literature on patient falls, relatively few studies have specifically explored the phenomena and outcomes of assisted falls. Moreover, those few studies have reached disparate conclusions about the injury risks to patients, with even less known about the injury risks to health care staff. For example, Krauss and colleagues found that assisted falls were associated with decreased risk of patient injury.8 Similarly, Staggs and colleagues found that assisted falls were associated with decreased risk of, and decreased severity of, such injury.2 Conversely, Venema and colleagues found that, absent the use of a gait belt, assisted falls were more likely to result in patient injury.16 These contradictory findings, as well as the lack of evidence about what prompts staff members to intervene with a falling patient (such as a sense of duty to protect the patient or a fear of blame if no action is taken), warrant further qualitative inquiry.
METHODSProject aims. This QI project had three aims, which were to 1) identify common scenarios in reported descriptions of assisted falls that involved VA staff and patients in order to better understand contributing factors, 2) document VA staff members' firsthand experiences of assisted falls and their perceptions of the safety risks to themselves and their patients, and 3) explore factors that influenced VA staff members' perceptions about assisted falls, including their definitions of such falls and their beliefs about their facility's fall-related policy.
Design. This project was based in grounded theory. Primary data (from interviews with VA staff) and secondary data (from clinical documentation of assisted falls in VA facilities) were analyzed comparatively to identify patterns that could provide insight into VA processes and clarify areas for improvement. The project was determined to be a QI evaluation by the VA research and development committee at the authors' facility, with a focus on improving facility operations, and as such was exempt from review by the institutional review board.
Data collection and analysis. Secondary datasets. Before 2020, VA facilities were not required to track assisted falls, although many did. At the start of this project, a general call was issued in April 2019 to a national Veterans Health Administration (VHA) patient safety workgroup, asking that tracked assisted fall–related QI data be shared. Two VA facilities reported having such data. Retrospective data from October 1, 2007, through September 30, 2018, were then gathered by patient safety managers at the two facilities. The final patient injury dataset included 63 narrative descriptions of assisted falls and documented resulting patient injuries and injury severity. The final employee injury dataset included 132 records of employees injured during an assisted fall. Each dataset included fall narratives and related variables.
Three evaluators (MC, JL, BB) compared deidentified data from the patient injury dataset and the employee injury dataset to identify commonly documented variables and discern the common characteristics of assisted falls that had resulted in patient or staff injury. Narrative data were organized using an Excel spreadsheet to create a qualitative data matrix.17 Two evaluators (MC, JL) coded these matrix rows independently, using a word or phrase to represent the essential meaning of the text, then compared coding. Discrepant codes were discussed in large team meetings with clinical and patient safety experts until consensus was reached. Qualitative code frequencies were calculated to clarify the prevalence of a given theme within the total dataset. This information was also helpful to us in creating the interview guide.
Interviews. Purposive convenience sampling was used to find eligible participants. The SPHM coordinators at 179 VA facilities nationwide were asked to recommend employees who met the following criteria: employed at a VA health care facility; employed as a nurse, physical or occupational therapist, or health technician; and experienced an assisted fall at any point in their career. Thirteen facilities responded, recommending a total of 24 individuals. These potential participants received an initial email invitation and up to three follow-up emails over the course of one month.
The interview guide consisted of semistructured questions that were developed by trained evaluators with backgrounds in social, behavioral, and clinical research (MC, JL). The purpose of the interviews was to learn more about the circumstances surrounding assisted falls from the perspective of VA staff with firsthand experience, including their actions, thoughts, feelings, and decision-making processes. Staff were also asked about practice recommendations for assisted falls. The interview guide was pilot tested with nursing staff at the authors' facility, resulting in added questions about facility protocols and previous assisted falls training or education. The final interview guide and an electronic audiovisual consent form were emailed to participants prior to interviews. (For the guide, see Interview Guide for Assisted Falls.) Participants were informed that audio recordings would be kept in a secure folder behind the VA firewall and destroyed after the project concluded. They also completed a short online demographics survey via REDCap, a secure data management methodology.
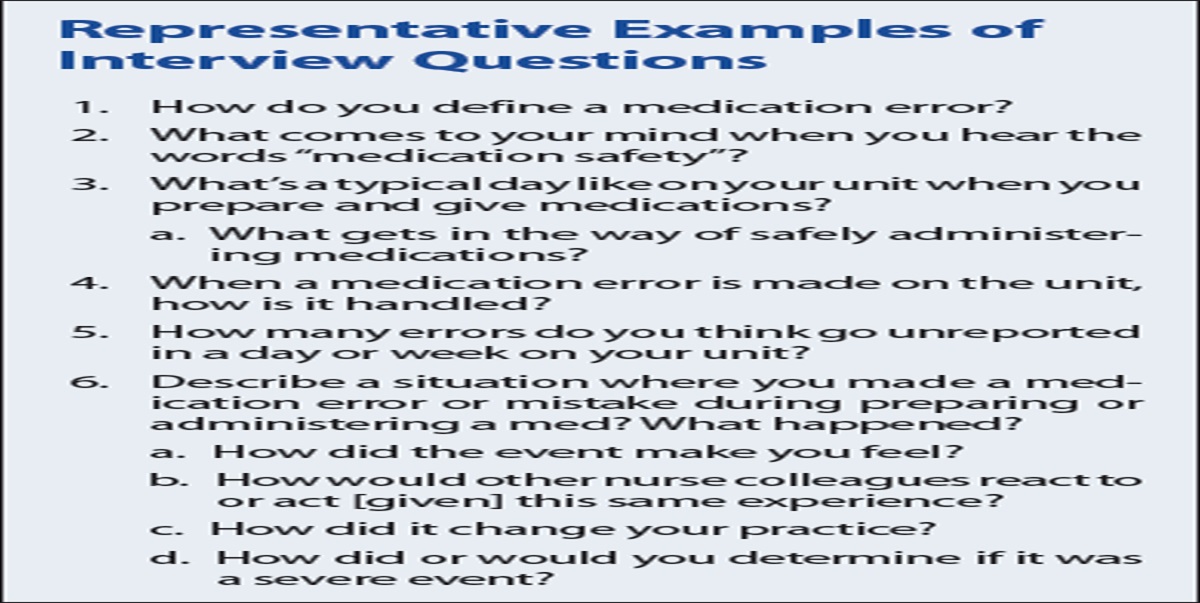
 Box 1:
Box 1: Interview Guide for Assisted Falls
Interviews were conducted during September and October 2020. Because of the ongoing COVID-19 pandemic, these were held virtually, using videoconferencing technology and following recommendations identified in the literature.18-20 Three of us (MC, SEB, JL) conducted the interviews in teams of two, taking turns as facilitator (asking questions per the interview guide) and cofacilitator (taking notes using a note-taking template). Each interviewer asked clarifying questions as needed. At the end of the interview, the cofacilitator verbally summarized the key messages and asked the interviewee to confirm or build on the summative understanding. Qualitative data saturation was reached at 16 interviews, when primary themes were consistent across the interviews and no new themes emerged.21
Written transcript summaries were created after each interview.22, 23 The cofacilitator reviewed their notes against the audio recording and edited the text for accuracy. Direct quotes deemed most relevant to the project purpose were also transcribed verbatim and added to the summary. Lastly, the facilitator and a third evaluator reviewed the transcript summary against the recording and made any final edits as necessary. A thematic content analysis of transcript summaries was conducted using ATLAS.ti version 8.4 software. The qualitative evaluators (MC, SEB, JL) then reviewed and refined the codes and emergent themes. Code frequencies were calculated to clarify the prevalence of a given theme within the total dataset.
RESULTSInterviewee characteristics. A total of 16 staff members from 13 VA facilities across the United States were interviewed. Most were in nursing roles (75%). A majority (62.5%) had received training on assisted falls in the past, and nearly one-third (31.3%) reported receiving regular or recurrent training on assisted falls. (For more details, see Table 1.)
Table 1. - Interviewee Demographics, Clinical History, and Experience Characteristic n (%) Gender Female 12 (75) Male 4 (25) VA professional role RN 5 (31.3) CNA 3 (18.8) NP 2 (12.5) LPN 2 (12.5) Physical therapist 2 (12.5) Health technician 1 (6.3) Occupational therapist 1 (6.3) VA unit assignment Acute care ICU 1 (6.3) Acute care medical–surgical 4 (25) Long-term care/rehabilitation 5 (31.3) ED 2 (12.5) Specialty clinica 2 (12.5) Facility level SPHM coordinator 1 (6.3) Acute psychiatric unit 1 (6.3) Assisted falls training frequency Received assisted falls training in the past 10 (62.5) Receives assisted falls training regularly 5 (31.3) Never received assisted falls training 1 (6.3) Training location (selected all that applied) Current VA facility 7 (43.8) Another VA facility where previously employed 1 (6.3) Current VA unit 3 (18.8) Another VA unit where previously assigned 2 (12.5) Outside VA 8 (50) Training modality (selected all that applied) In-service training 8 (50) Face-to-face demonstrations 9 (56.3) Simulations 6 (37.5) Online education 5 (31.3)CNA = certified nursing assistant; SPHM = safe patient handling and mobility; VA = Veterans Affairs.
aSpecialty clinic included the ambulatory procedure unit and program management and education.
Aim 1: Identify common assisted falls scenarios and illuminate contributing factors. Secondary datasets. Common assisted falls scenarios emerged from thematic analysis of the secondary patient injury dataset and employee injury dataset. Most documented assisted falls occurred in patient rooms, especially bathrooms. Most such falls occurred when a patient was ambulating or transferring and became unsteady or unable to bear weight. Another common scenario involved a patient slipping during a wheelchair transfer. The causes of patient unsteadiness varied, with “dizziness” emerging most frequently. In most scenarios, the patient had a documented cognitive impairment or psychiatric diagnosis (89%) or had altered mobility status (94%). Less frequently, patients became unsteady because they lost consciousness or had a seizure.
In general, for assisted falls recorded in the datasets, documentation indicated that a staff member had eased the falling patient to the ground or a nearby surface. Occasionally, it was reported that the patient grabbed onto a nearby staff member to steady themselves as they began to fall. In the employee injury dataset, records for the 132 assisted falls staff injuries showed that knee, shoulder, neck, and back injuries (usually the lower back) were common. Of the 63 assisted falls narratives included in the patient injury dataset, one fall resulted in a major patient injury, 10 resulted in minor patient injuries, and 52 resulted in no patient injuries. Frequently reported patient injuries included bruising and skin tears.
Interviews. The assisted falls experiences recounted by interviewees described similar fall incident locations and assist mechanisms. As in the patient injury dataset fall narratives, interviewees described that assisted falls most commonly took place in a patient's room or bathroom. They also said that patients were often ambulating or transferring when their legs gave out or they lost balance, precipitating a fall. The interviewees described assisting these falls by grabbing the patient, holding the patient with or without the use of a gait belt, and using their own body to brace or steady the patient. In most cases, the staff member lowered or guided the patient to the floor. Notably, in 70% of the assisted falls described during interviews, the patients who fell had no known history of falls, weakness, or imbalance (although many had other fall risk factors, most often psychotropic medication use). Many interviewees described using an “arm under arm” method for stabilizing patients and assisting them to the ground, which for some staff resulted in shoulder and lower back injuries. In some cases, when acute onset of an illness precipitated the fall, staff reported using their legs to brace the patient before easing them to the ground or another surface.
Four of the 16 interviewees said they had been injured while assisting a fall. Three described their injuries as serious, although only two said they missed work because of the injury. Three interviewees reported that the patient had sustained minor injuries during the assisted fall. Across the sample, the most common assisted fall–related injury sites were, for staff and patients respectively, the lower back and the legs.
For an illustration depicting these findings, see Figure 1.
 Figure 1.:
Figure 1.: Project Findings: Patient and Staff Injury Sites Resulting from Assisted Falls
Aim 2: Document staff experiences of assisted falls and their perceptions of risks. Interviewees were asked when, in their experience, staff should assist a falling patient. Most (75%) stated that staff members should try to assist a fall if they could do so safely both for the patient and for themselves. Interviewees were also asked what they believed to be the safest way to assist a fall. Some based their response on their experiences with assisted falls, while others based it on training they had received. Thirteen interviewees (81%) said they learned through formal training that the safest way was to use “proper body mechanics” (for example, holding the patient close to the body, bending the knees, and keeping the back straight). They also described being educated about using proper equipment when handling and moving patients and protecting the falling patient's head. Other suggestions included using a wall or the bed to stabilize their own body during the assist, which was often learned through experience.
Nearly two-thirds of the interviewees (63%) said that if staff were not in the proper position or location relative to a falling patient and would have to reach out to make contact, then they should not try to assist. More than half (56%) said that staff should not assist a fall if the patient was significantly larger than they were. Some interviewees (38%) noted that staff should not assist a fall if the patient was combative or seriously disoriented (such as in cases of dementia) because such patients can be unpredictable. Many interviewees reiterated that, in deciding whether they could safely assist a fall, they must consider the clinical context and assess the injury risk both to the patient and to themselves. As one RN said,
“You have to keep yourself safe first, so if you can help assist the patient that's great, but the primary goal is that you don't get hurt.”
Interviewees were asked whether they would have done anything differently during the recounted assisted falls. Reflecting on these experiences, some staff believed that patients would have been injured or patient injuries would have been more serious if they had not assisted. Half (50%) also said they would have done something differently. These sentiments included using SPHM equipment, getting another staff member's assistance, improving communication with the patient to describe the transfer process, and checking the patient's medical chart more closely or consulting with other staff regarding the patient's clinical condition before the fall occurred.
Aim 3: Explore factors that influenced staff perceptions. Definitions and documentation. The way interviewees defined an assisted fall affected how they documented such falls. Most interviewees (75%) defined it as a fall in which a staff member intervenes by using physical contact to aid the patient's descent to the floor. For example, one NP defined an assisted fall as
“a fall where a patient is falling, and a nurse has a hand on that patient to help the patient into a safe position that protects the patient from physical injury on their way down to the floor.”
Interviewees agreed that in such cases, a fall incident report would be recorded because the patient ended up on the floor. But in cases when the patient was assisted to another location like a chair or bed, their views diverged. Just over half the interviewees (56%) considered this type of fall incident to be a “near miss” instead of an assisted fall. But several others felt that using physical contact to help a patient's descent to any stable location, including a chair or bed as well as the floor, qualified as an assisted fall. One RN offered this broader definition of an assisted fall, saying,
“[it's] when a patient unexpectedly ends up somewhere they didn't want to be, and staff find a way to help them go down more softly or assist them to another position so that they don't get injured. It doesn't matter if it's the floor, chair, or bed, as long as it was somewhere unintended.”
Perceptions of facility policy. None of the interviewees reported that their facility had an official policy concerning assisted falls. Seventy-five percent reported that their facilities had no official policy, and the remaining 25% were unsure whether an official policy existed. But nearly all interviewees (94%) indicated that there was an unofficial “shared understanding” in their facility about assisting falls, although these unofficial protocols were inconsistent.
For half of the interviewees (50%), the shared understanding at their facility was that staff should assist a falling patient only if they judged that they could do so safely. Regardless, many interviewees described feeling a strong sense of obligation to intervene when they see a patient falling. For example, one LPN said, “Nurses have an instinct to catch a falling patient.” A health technician noted that for staff, seeing a patient fall without intervening “goes against their core values because they are there to protect their patient.” Several interviewees felt that if they had not intervened when a patient fell, that patient would have sustained a major injury or perhaps even died.
In contrast, 44% of interviewees perceived that at their facility the unofficial protocol was to “let the patient fall,” because intervening could result in staff or patient injury; instead, they were to focus on securing the environment (such as by moving furniture or equipment out of the way or throwing pillows under the falling patient). Despite this perception of hands-off policies at some facilities, many interviewees acknowledged that if they witnessed a patient falling and thought they could prevent patient injury by assisting, they would try. Several interviewees (44%) explained that they were told that assisting falls was inconsistent with a VHA directive cautioning staff against lifting more than 35 pounds.24
Almost all of the interviewees (88%) felt that regular training in assisted falls would benefit staff. One RN explained that because assisted falls are “high risk, low frequency” events, staff need regular training to ensure that they know how to react appropriately in the moment. Several interviewees felt strongly that simulations or videos depicting common assisted falls scenarios would improve training.
DISCUSSIONCharacteristics of assisted falls. Our findings about factors that contribute to fall incidence and outcomes align with findings from previous research on the subject. Prior studies found that patient rooms and bathrooms were common sites for unwitnessed12 as well as assisted and unassisted falls,16 making these sites important for preventive interventions. Those studies also found that higher fall and fall injury risk activities included ambulating and transferring (such as from bed to wheelchair or wheelchair to toilet).
In our project, patient status was a key factor in assisted falls, as was evident in the data from the secondary datasets and interviews. Specifically, we found cognitive status to be a contributing factor, as most of the patients whose falls were documented or discussed had a psychiatric illness or cognitive impairment, and many were on psychotropic medications for these conditions. These findings are consistent with those of earlier studies that found psychiatric illness or cognitive impairment,14, 25 as well as the use of psychotropic drugs,13, 26, 27 to be associated with increased risk of falls and fall injuries. In our project, mobility status was another contributing factor, as almost all of the patients in the secondary datasets had altered mobility. This too is consistent with prior research identifying mobility impairment as a major fall risk factor.14 These findings highlight the importance of comprehensive patient assessment in order to ensure that adequate safeguards are taken to prevent patients at high fall risk from falling and to avoid the need for fall assistance.
Staff perceptions of safety risks. Previous research on assisted falls has produced conflicting conclusions about whether assistance should be encouraged or discouraged. For example, studies by Krauss and colleagues and Staggs and colleagues determined that, compared with assisted falls, unassisted falls were associated with increased patient risk of fall injury.2, 8 Both studies recommended promoting the use of fall assistance to reduce patient fall injuries. In contrast, Venema and colleagues found that assisted falls that did not incorporate use of a gait belt actually increased the odds of patient injury.16 They concluded that improved staff training in how to assist a fall was essential. Notably, none of these studies considered staff injury in their evaluations.
A majority of interviewees in our project believed that patient falls should be assisted when doing so is possible without staff or patient injury. While they proposed different methods for mitigating such risk in staff and patients, in general they believed that there are safe (or safer) ways to assist falls. Our analysis of both the employee injury dataset and interview narratives showed that staff injury can and does occur, even among experienced staff. It may not be possible to ensure that injury can always be prevented during assisted falls. Indeed, previous studies investigating the use of body mechanics in other forms of patient handling have shown that such approaches alone are not effective in reducing staff injuries.5, 6
The interviewees in our project were aware of various techniques that could reduce the incidence of patient falls, such as direct observation and purposeful rounding. But they reported that, in practice, the complexity of patient care created barriers to using these techniques, a finding similar to those of Grealish and colleagues.28 Moreover, there are scenarios in which staff cannot prevent assisted falls, such as when a falling patient grabs onto them.
Interviewees also mentioned feeling an “instinct” or sense of “moral obligation” that arose when they witnessed a falling patient and could physically intervene to prevent harm to that patient, even if doing so might result in personal injury. An unpublished report on QI work at our hospital found that the concept of “nurses' duty to patient” was a significant factor in causing staff to disregard their own safety in order to protect a falling patient.29 Studies of moral injury and moral distress among nurses have shown that guilt and shame are commonly experienced after an injurious patient safety incident.30, 31 Often, nurses feel that they could have done more to prevent the incident. In a literature review of moral distress among nurses, Oh and Gastmans found that nurses felt such distress when pressed by circumstances to act against a patient's best interest, and that such experiences contributed to developing burnout.30 For this reason, the relationship between staff members' sense of moral obligation to assist a falling patient and their beliefs about the risks to their own safety in doing so warrants further investigation.
This project contributes new information about the patient and staff injury outcomes of assisted falls that occur during toileting, transfers, and ambulation. Findings showed that staff commonly sustained neck, shoulder, and back (especially lower back) injuries during an assisted fall, whereas patients, if injured at all, experienced bruising or other skin injuries, most often on the legs. The findings further demonstrate the complicated influence of individual staff members' perceptions on this topic, with some continuing to view assisted falls as safe, even when they had experienced injury in the past. A related assisted falls project used virtual reality simulations of patient falls to test staff risks for lower back injury, and found that staff members remained at risk for such injury despite using ergonomic techniques.4
Taken together, this project's findings may support the conclusion reached by others that assisted falls can decrease patient injury risk,2, 8, 32 with the added understanding that staff injury risk may increase. These findings have important implications for staff guidance on assisted falls, but further research is needed to better understand the relative risks of staff versus patient injury during an assisted fall.
Assisted falls definitions and facility policies. Although most interviewees had received some relevant training, they described a lack of official directives, policy, or guidance related to assisted falls. In the absence of official policy, individual units or facilities adopted a “shared understanding” that was communicated person-to-person among staff or championed by SPHM leaders. Definitions for what constitutes an assisted fall also varied. In some facilities, interviewees reported that an assisted fall meant helping the falling patient to the floor, specifically, while in others the patient could also be helped to another surface. Such varying definitions result in differences in how assisted falls are documented and perceived. Most interviews wanted more regular staff training on assisted falls. This would be beneficial, as would more education on a standardized definition of an assisted fall, and would allow researchers to compare the rates of assisted falls and assisted fall–related injuries across facilities.
Implications for practice. Understanding the characteristics, drivers (social, behavioral, structural, and environmental), and staff perceptions of assisted falls can help health care professionals prevent and manage falls effectively in clinical practice and potentially reduce the injury risk. Beyond implementing interventions that reduce fall risk in general (such as providing patients with assistive devices and instruction in use, and conducting standard intentional rounding), implementing additional measures may mitigate the risks associated with assisted falls. Based on this project's findings, we recommend the following:
Mobility screening. While assisted falls can reduce the injury risk for patients, they may increase that risk for staff. The use of mobility screening tools can guide staff in choosing the most appropriate SPHM technology, thus lowering the risk of an assisted fall happening during care tasks. Risk assessment. Regular and repeated fall and fall injury risk assessments are vital, not only to identify those patients who may be at higher risk, but also to monitor patients for changes in risk status so that preventive interventions can be applied. Such assessments must include a thorough medication review in order to identify patients whose medications could increase their fall risk even if they have no other risk factors. Communication. Communicating with staff about the definition of and risks associated with assisted falls will help to prevent such falls, as well as promote appropriate follow-up and documentation when assisted falls do occur. Clear documentation is essential so that the causes and outcomes of assisted falls can be better understood and prevented or managed. There must also be ongoing communication among staff members about individual patient fall risk.Limitations. At the time of this project, VA facilities were not required to track assisted falls, and only two VA facilities reported capturing information on such falls. Thus, we were limited to data in the secondary employee and patient injury datasets kept by these two VA facilities. Documentation was unique at each facility and the types of data captured varied between the datasets. For these reasons, our findings may not be generalizable to other VA (or non-VA) facilities. The length of time between an assisted fall event and the assisting staff member's recruitment and participation in our interviews also varied. Some interviewees had assisted in a patient fall just weeks before their interview, while others had done so years ago; it's possible that in some cases, the time gap affected recall accuracy. That said, it's worth noting that there is some evidence that stressful events lead people to form detailed and long-lasting memories,33 and most interviewees appeared to have strong recall of their assisted fall experiences.
CONCLUSIONSThis project's findings provide valuable insight into assisted falls, including common contributing factors, patient and staff injury outcomes, and the sociocultural and behavioral influences that may determine those outcomes. The use of qualitative methods allowed us to document staff experiences with and perceptions of assisted falls and to illuminate the complexity that surrounds these falls. Although the literature is mixed regarding the advisability of assisting a falling patient, our results indicate that there may be no safe way to do so without risking injury to staff. Official policies regarding assisted falls, as well as directives for sufficient staff education and training, may be absent or limited, and staff may have misconceptions about their ability to assist patient falls safely. The common belief that staff members have a moral duty to assist a falling patient regardless of the risk to themselves further complicates the issue. This barrier to creating a culture of safety must be recognized and addressed. For these reasons, institutional assisted fall policies should be developed collaboratively, with the lived experiences of staff given due weight. Further efforts to identify effective assisted fall strategies and provide clear guidance to staff are also warranted.
REFERENCES 1. National Database of Nursing Quality Indicators (NDNQI). Patient falls—ambulatory indicator: guidelines for data collection and submission. South Bend, IN: Press Ganey Associates; 2021 Aug. 2. Staggs VS, et al. Assisted and unassisted falls: different events, different outcomes, different implications for quality of hospital care. Jt Comm J Qual Patient Saf 2014;40(8):358–64. 3. Turner K, et al. Patient falls and injuries in U.S. psychiatric care: incidence and trends. Psychiatr Serv 2020;71(9):899–905. 4. Broderick V, et al. Staff low back injury risk during assisted falls virtual reality simulations. Workplace Health Saf 2023;71(6):304–10. 5. Nelson A, et al. Myths and facts about back injuries in nursing. Am J Nurs 2003;103(2):32–40. 6. Nelson A, et al. Development and evaluation of a multifaceted ergonomics program to prevent injuries associated with patient handling tasks. Int J Nurs Stud 2006;43(6):717–33. 7. Hitcho EB, et al. Characteristics and circumstances of falls in a hospital setting: a prospective analysis. J Gen Intern Med 2004;19(7):732–9. 8. Krauss MJ, et al. Circumstances of patient falls and injuries in 9 hospitals in a midwestern healthcare system. Infect Control Hosp Epidemiol 2007;28(5):544–50. 9. Lee JE, Stokic DS. Risk factors for falls during inpatient rehabilitation. Am J Phys Med Rehabil 2008;87(5):341–50. 10. Friedman Y, et al. Witnessed and assisted falls in the Veterans Health Administration: prevalence and patient injury outcomes [poster abstract]. J Am Geriatr Soc 2022;70(Suppl1):S39–S40. 11. de Jong LD, et al. Exploring hospital patient sitters' fall prevention task readiness: a cross-sectional survey. J Eval Clin Pract 2020;26(1):42–9. 12. Hignett S, et al. Exploring the contributory factors for un-witnessed in-patient falls from the National Reporting and Learning System database. Age Ageing 2011;40(1):135–8. 13. Lee A, et al. Using root cause analysis to reduce falls with injury in the psychiatric unit. Gen Hosp Psychiatry 2012;34(3):304–11. 14. Schwendimann R, et al. Characteristics of hospital inpatient falls across clinical departments. Gerontology 2008;54(6):342–8. 15. STEADI, Stopping Elderly Accidents, Deaths, and Injuries. Risk factors for falls. Atlanta, GA: Centers for Disease Control and Prevention; 2017. Fact sheet; https://www.cdc.gov/steadi/pdf/STEADI-FactSheet-RiskFactors-508.pdf. 16. Venema DM, et al. Patient and system factors associated with unassisted and injurious falls in hospitals: an observational study. BMC Geriatr 2019;19(1):348. 17. Averill JB. Matrix analysis as a complementary analytic strategy in qualitative inquiry. Qual Health Res 2002;12(6):855–66. 18. Allen MD. Telephone focus groups: strengths, challenges, and strategies for success. Qual Soc Work 2014;13(4):571–83. 19. Krueger RA, Casey MA. Telephone and internet focus group interviewing. In: Krueger RA, Casey MA, editors. Focus groups: a practical guide for applied research. 5th ed. Thousand Oaks, CA: SAGE Publications; 2015. p. 205–22. 20. Musselwhite K, et al. The telephone interview is an effective method of data collection in clinical nursing research: a discussion paper. Int J Nurs Stud 2007;44(6):1064–70. 21. Fusch PI, Ness LR. Are we there yet? Data saturation in qualitative research. Qual Rep 2015;20(9):1408–16. 22. Beebe J. Rapid assessment process: an introduction. Walnut Creek, CA: AltaMira Press; 2001. 23. Beebe J. Rapid qualitative inquiry: a field guide to team-based assessment. 2nd ed. Lanham, MD: Rowman and Littlefield; 2014. 24. U.S. Department of Veterans Affairs, Veterans Health Administration. Safe patient handling and mobility program. Washington, DC; 2008 Mar 23 (amended Jul 16, 2020). VHA directive 1611. 25. Kobayashi N, Sugai Y. Witnessed and unwitnessed falls among the elderly with dementia in Japanese nursing homes. Jpn J Nurs Sci 2006;3:31–41. 26. Johnell K, et al. Psychotropic drugs and the risk of fall injuries, hospitalisations and mortality among older adults. Int J Geriatr Psychiatry 2017;32(4):414–20. 27. Landi F, et al. Psychotropic medications and risk for falls among community-dwelling frail older people: an observational study. J Gerontol A Biol Sci Med Sci 2005;60(5):622–6. 28. Grealish L, et al. Caring for the older person with cognitive impairment in hospital: qualitative analysis of nursing personnel reflections on fall events. J Clin Nurs 2019;28(7-8):1346–53. 29. Trainor B. Looking for synergy: between the culture of patient and nursing safety [unpublished report]. 2016. 30. Oh Y, Gastmans C. Moral distress experienced by nurses: a quantitative literature review. Nurs Ethics 2015;22(1):15–31. 31. Stovall M, et al. A critical review: moral injury in nurses in the aftermath of a patient safety incident. J Nurs Scholarsh 2020;52(3):320–8. 32. Johnson M, et al. Analysis of falls incidents: nurse and patient preventive behaviours. Int J Nurs Pract 2011;17(1):60–6. 33. Martijena ID, Molina VA. The influence of stress on fear memory processes. Braz J Med Biol Res 2012;45(4):308–13.
Comments (0)