
Remember me
This prospective cohort study included all radiocephalic fistulas created at Wujin Hospital Affiliated with Jiangsu University from January 1, 2018, to December 31, 2020. The inclusion criterias were as follow. Patients had the indications and conditions for establishing autogenous AVF according to KDOQI Clinical Practice Guideline for Vascular Access [15]. Radiocephalic AVF was established at the wrist of the forearm for the first time.
The exclusion criteria were as follows: (1) patient < 18 or > 75 years of age, (2) artery size < 2 mm, (3) vein size < 2 mm, (4) stenosis of the arterial system exist, (4) stenosis of the central vein, implantation materials of the central vein, (5) heart failure and other serious cardiovascular diseases, (6) cooperate with difficulty, (7) skin infection, (8) abnormal blood coagulation function.
Surgical procedures and groupingBefore the operation, the sizes of arteries and veins were measured by ultrasound, the shape of arteries and veins was marked, and the distance between arteries and veins was measured. Surgical operations of the fistula were performed by a same experienced surgeon under local anesthesia. After separating the arteries and veins, the anastomosis angle was designed according to the vessel length, size, shape and especially distance of the vein from the artery. Anastomosis method was functional ETS anastomosis using side-to-side anastomosis with distal vein ligation. The length of anastomosis usually reached 10–12 mm. A tension-free anastomosis was performed with a continuous suture of 7–0 suture line. When the anastomosis was complete, the protractor was used to measure the anastomotic angle precisely. Grouping was according to AVF anastomosis angle, dividing into groups of 30 ≤ angle ≤ 50°, 50 < angle ≤ 70°, and 135°smooth obtuse angle (Fig. 2). The grouping was not random, but was based on vascular anatomy.
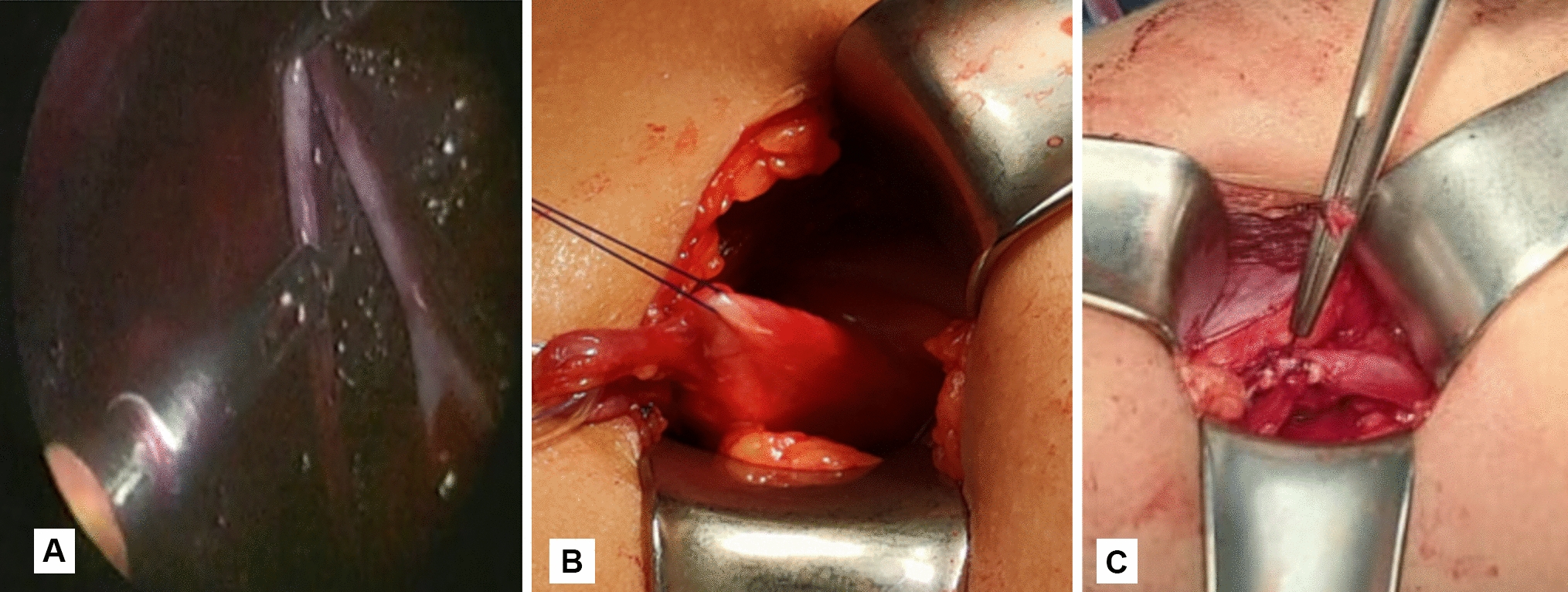
Fig. 2
A Functional ETS anastomosis with 30–50° anastomosis angle; B Functional ETS anastomosis with 50–70° anastomosis angle; C Functional ETS anastomosis with 135° smooth obtuse angle
Follow-upNephrologists track the access through clinical examinations and access flow monitoring monthly during hemodialysis. The first examination of ultrasound is performed at 4 weeks after surgery to measure vessel diameter and access flow and then every 2–3 months typically. If access shows sign of dysfunction, suspicious stenosis or thrombus, we use ultrasound or angiography to diagnose. Endovascular intervention and open surgery are used for treatment of access dysfunction, thrombus and stenosis. The follow-up time was 1 year.
Outcomes and definitionsThe end points were the primary patency rate(PPR) and the secondary patency rate(SPR). Primary patency is the interval from the time of access placement until any intervention designed to maintain or reestablish patency, access thrombosis, or the time of measurement of patency. Secondary or cumulative patency was calculated from the time of vascular access creation until permanent access failure, regardless of the number of procedures required to maintain access patency for dialysis [16]. The other end point was the cumulative rate of reintervention close to 4 cm vein of anastomotic segment [17, 18]. Chinese guideline defined access as functional when natural blood flow > 500 ml/min, the pump controlled blood flow during dialysis was greater than 200 ml/min maintained for 4 h [19].
Statistical analysisWe performed the data analysis using spss 22 statistical software. Categorical variables were expressed as the number and percentage of patients. Differences between categorical variables were determined by the Pearson χ2 test. Continuous variables were expressed as the mean ± standard error. Differences between continuous variables were determined by the One-way analysis of variance. Kaplan–Meier analysis was used to calculate the curves of patency rate and the cumulative rate of reintervention near anastomotic venous segment, with curves compared using log-rank analysis. The Cox proportional hazards regression model was used to control potentially confounding factors. Values of P < 0.05 was considered statistically significant.
Comments (0)