
Remember me

The vast majority of injury-related death and disability occurs in low- and middle-income counties (LMIC).1 This burden is projected to climb over the next decade with expanding industrialization.2–4 Cameroon is a lower-middle income country in central Africa with injury death rates 40% higher than in the United States.5–7 Because of provider and resource scarcity, Cameroonian trauma patients do not receive routine follow-up care after hospital discharge. Lack of follow-up trauma care likely contributes to late recognition of complications, treatment delays, and increased long-term physical and economic disability and mortality.6,8 Early identification of patients who would benefit from further care may facilitate prompt treatment for high-risk patients and mitigate complications, disability, and death.
As in many other sub-Saharan African LMIC, mobile telephone penetrance in Cameroon has increased dramatically over the past decade. Cross-sectional injury surveillance suggests that more than 90% of Cameroonian families currently have access to cellular telephones.9 Leveraging this growing prevalence of cellular telephone use has potential to expand follow-up care capacity for Cameroonian trauma patients; however, no protocol for telephone follow-up after injury has been developed or validated in this context. Ideally, an LMIC telephone follow-up program would be time and resource efficient, administered by nonclinicians, and capable of discriminating discharged patients at elevated risk for poor outcomes without further care. A single-center pilot demonstrated promising feasibility of a nonclinician administered mobile health triage survey administered 2 weeks after hospital discharge.10 However, this pilot study did not test associations of individual questions with the criterion standard of a physician examination and lacked generalizability given its single institution design. In this prospective multisite implementation study, we sought to develop and validate a context-appropriate cellular telephone screening tool designed to risk stratify trauma patients in need of further care after hospital discharge in Cameroon.
PATIENTS AND METHODSCameroon is a mixed anglophone-francophone lower-middle income country in central Africa with a trauma burden higher than adjacent central African countries.6,9 The Cameroon Trauma Registry (CTR) is a trauma registry collecting prospective data on injured patients at four trauma hospitals: hospitals A, B, C, and D.6,7 All patients who are admitted or transferred, leave against medical advice, or die from injury at the hospital are included in the CTR, regardless of age or injury severity. Cameroon Trauma Registry patients are followed from emergency department presentation to hospital discharge.
Between June 2019 and August 2022, patient phone numbers were extracted from the CTR. All CTR patients who were discharged after hospital admission for injury were eligible for inclusion in the mobile follow-up program. Research assistants contacted eligible participants by mobile phone at 2 weeks following hospital discharge; participants were contacted at least three times by calling and once by text message over a 1-week interval. Successfully contacted patients or surrogates were asked to complete a telephone survey with 14 candidate triage questions.
Triage questions were developed in collaboration with Cameroonian trauma clinicians and designed to mimic questions asked in a follow-up examination. Potential survey questions were solicited from local experts and compiled from a broad literature review on surgical telephone follow-up, before being reviewed by an expert panel of Cameroonian trauma stakeholders.11–19 Questions were then pretested for acceptability and understandability on a small group of hospitalized patients and family members. Candidate triage questions queried overall well-being, ability to perform activities of daily living (ADLs), barriers to healing, symptoms, and seeking additional care (Table 1). To target triage and improve future implementation, data were also collected on whether the patient had died before survey collection.
TABLE 1 - Candidate Triage Questions Category Candidate question Answer Overall well-being Is the patient currently alive*? Yes/no 1. Since leaving the hospital, how have they been feeling? (general pattern with regard to things like pain, energy, and strength) Better/same/worse 2. Have they been able to return to their normal daily routine? (including work in and out of the home, school, social activities) Yes/some activities/no ADLs 3. Do they need daily help to feed, clothe, bathe, and go to the toilet? Yes/no Caring for self or injury Since leaving the hospital, have they had any problems? Yes/no (each) 4. Getting food or water 5. Taking medicines 6. Caring for the injury/wound as instructed 7. Other Symptoms Have they had the following problems since leaving the hospital? Yes/no (each) 8. Fever 9. Redness/swelling 10. Pain 11. Difficulty moving or feeling 12. Drainage or wound opening 13. Nausea, vomiting, or poor appetite Further care seeking 14. Since leaving the hospital, have they seen another doctor or healer for the injury? (Treatment includes formal or alternative medicine) Yes/no*This question is not used as a candidate triage question but to collect baseline mortality data and assess appropriateness of asking triage questions.
Regardless of survey responses, all contacted patients were asked to return for physician examination. As in the single-study pilot, returning patients were compensated for travel expenses using a need-based sliding scale.10 Based on physical examination findings, physicians rendered a determination of whether the patient (1) was demonstrating an on-trajectory recovery for their age, health status, and injury complex; (2) would benefit from further medical services (i.e., if additional follow-up care, diagnostic, or therapeutic interventions would potentially improve the health of the patient); and (3) whether the patient was at high, moderate, or low risk for a poor outcome without additional intervention using subjective clinical assessment. The absence of objective criteria such as diagnostic laboratories and imaging in the clinical assessment reflects the resource limitations present in the Cameroonian context. While all high-risk patients were advised of the type of medical care required, the decision to reenter care was left up to them given considerable cost barriers. Data were documented on paper forms and entered into Research Electronic Data Capture by research assistants hosted on a secure server.20 In statistical analysis, patients identified as being at moderate to high risk were designated as HR.
The Strengthening the Reporting of Observational Studies in Epidemiology guidelines was used to ensure proper reporting of methods, results, and discussion (Supplemental Digital Content, Supplementary Data 1, https://links.lww.com/TA/D149).21 The primary outcome of the study was the association between candidate triage questions and moderate to high risk for a poor outcome (HR) without additional intervention. Survey questions found not to contribute significantly to prediction were dropped from the final triage tool analysis. To use these data to develop a high-sensitivity model capable of efficiently identifying discharged patients most in need of follow-up care, we evaluated screening characteristics of a prospective weighted additive model. Secondary outcomes included model characteristics (sensitivity, specificity, false negative rate, and discrimination), as well as feasibility metrics including the proportion of contacted patients participating in triage and conventional examination.
A minimum sample size of 10 participants for each predictive variable per potential model outcome (HR considered as a dichotomous outcome) was targeted to adequately power regression analysis. Descriptive statistics are reported as means and SDs for normally distributed data and medians with interquartile ranges for ordinal and nonnormally distributed data. Binary variables are described with percentages. Associations between triage questions and HR were tested using logistic regression; questions with multiple answer levels (overall well-being, return to activities) were statistically evaluated with each answer as a separate variable. An additive scoring model weighting questions by predictive capacity was used to stratify patients into risk categories for HR. Screening characteristics evaluated included sensitivity, specificity, and false negative rates; receiver operating characteristic curves were calculated to evaluate the discrimination (area under the curve [AUC]). An α level of <0.05 was considered significant for all analyses. Statistical analysis was performed using Stata 14 (StataCorp, College Station, TX).22
Research assistants obtained oral consent for study participation from all patients or surrogates; consent for physician examination was confirmed and documented at the time of examination. Approval to conduct this study was granted by the IRB 19-000086 and the 2019/86811/UB/SG/IRB/FHS institutional review boards.
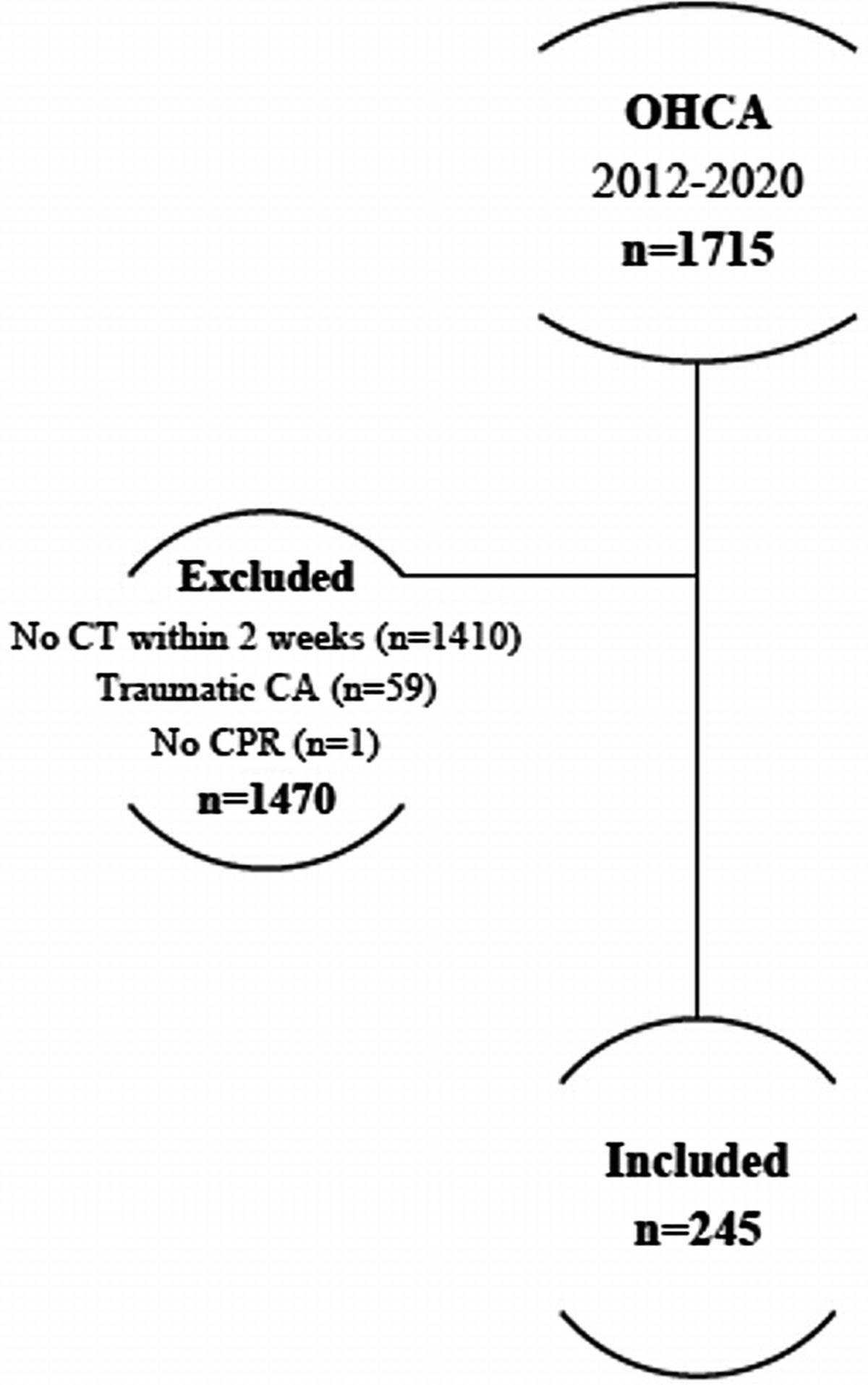
RESULTSBetween June 2019 and August 2022, 5,865 patients enrolled in the registry, and 92.2% (n = 5,406) of patients had access to a cellphone. Of this population, 1,712 patient households were successfully contacted by cellular telephone. Of these, 96% (n = 1643) consented and participated in telephone triage, 28 patients refused consent (1.6%), and 41 patients (2.3%) had died by the 2-week discharge time point (Fig. 1). Notably, 48% of triage surveys (n = 788) were completed by a patient surrogate such as a relative, friend, or caretaker, whereas 46% (n = 756) were completed by the patient themselves, and 6% (n = 99) were completed by a combination of both. The telephone follow-up cohort was representative of a standard young (median age, 32 years; interquartile range, 24–42 years) male predominant trauma population (male, 75%). Road traffic injury was the most common injury mechanism.
 Figure 1:
Figure 1: Enrolled patients for surveyed triage and physical examination.
Although all triaged patients were asked to return for physician examinations regardless of survey findings, only 33% (n = 560) completed physician examination. Leading reasons given for physician examinations not being performed included the patient not being able to get to the hospital (48%), nondisclosed reasons (26%), or the time required (9.6%). Based on physical examination findings, physicians ultimately designated 323 patients (58%) as potentially benefiting from further medical services and 220 (39%) of examined patients as being HR.
Triage Survey ResultsThe vast majority of patients (n = 517 [92%]) reported improved overall well-being since leaving the hospital with only 8% (n = 43) reporting similar or worse clinical status since discharge. Only 20% (n = 114) of patients had resumed their normal daily routine (i.e., performing all baseline daily actions) compared with 8% (n = 56) who had partially resumed their routine and 71% (n = 400) who reported that they had not yet resumed their daily routine. Overall, 36% (n = 350) reported still needing assistance with ADLs including eating, bathing, and going to the toilet. Nearly 30% (n = 167) of patients reported significant barriers to injury recovery in the home, including 2% (n = 10) who reported difficulty obtaining clean food or water after injury, 6% (n = 33) who were unable to afford or access prescribed medicines, and 10% (n = 56) who had difficulty understanding or following discharge instructions for injury care. In addition, 17% (n = 94) reported other barriers to healing not otherwise specified. Nearly 75% (n = 410) of surveyed patients or their surrogates endorsed the patient having one or more concerning symptom including subjective fevers (59 patients [12%]), erythema or swelling of the injured body part (38 patients [7%)], pain (372 patients [66%]), drainage from or opening of a wound or incision (14 patients [3%]), numbness or difficulty moving the injured area (109 patients [19%]), or nausea/vomiting (2 patients [<1%]). By 2 weeks following discharge, just under half of all discharged patients (242 [43%]) had sought a second opinion from a western or traditional healer.
On univariate logistic regression, 8 of 14 candidate triage variables were independently associated with HR (Table 2). Triage questions associated with HR included perceived well-being, difficulty taking medicine, difficulty caring for injury, redness or erythema, pain, inability to move or feel, drainage or opening of the wound or incision, and seeking a second opinion. Positive survey response on the resultant eight question screen yielded 89.2% sensitivity for HR with a 10.8% false-negative rate. Specificity was 18% and overall accuracy was 42%.
TABLE 2 - Univariate Logistic Regression of HR on Candidate Triage Questions OR p 95% Confidence Interval Overall well-being 3.4 <0.01 1.9–6 Same as leaving the hospital 3.3 <0.01 1.7–7 Worse than leaving the hospital 12.7 0.02 1.5–106 Resumed daily routine All actions 0.9 0.82 0.6–1 Some actions 1.2 0.53 0.7–2 ADLs 1.1 0.57 0.8–2 Difficulty with: Obtaining food and water 1.3 0.72 0.4–5 Taking medicine 6.6 <0.01 2.9–15 Caring for the injury 4.3 <0.01 2.4–8 Other 0.8 0.28 0.5–1 Injury symptoms Fever 1.6 0.11 0.9–3 Redness or swelling 7.0 <0.01 3.2–15 Pain 1.5 0.04 1.0–2 Unable to move or feel 2.8 <0.01 1.8–4 Drainage/opening of the wound/incision 7.3 <0.01 2.0–26 Nausea or vomiting 1.9 0.65 0.1–30 Sought second opinion 1.7 <0.01 1.2–2To develop a sensitive model capable of risk stratifying discharged patients for HR, all candidate questions found to associate with HR on univariate regression were weighted by their predictive coefficient and added to generate a triage risk score (TRS) ranging from a minimum score of 0 (lowest risk) to a maximum possible score of 43.9 (highest risk) (Fig. 2). Triage risk score in the examined cohort ranged from a minimum of 0 to a maximum of 41.7. Median TRS was 1.7 (interquartile range, 1.4–4.1). Overall AUC of the resultant receiver operating characteristic curve was 0.68; sensitivity and specificity cutoffs for the additive model are presented in Figure 3. Patients with high TRS were more frequently designated as HR by Cameroonian physicians (Fig. 4). Approximately 60% of patients with TRS in the fourth quartile (TRS, >4.1) were found to be HR, compared with approximately 33% in the second (TRS, 1.4–1.6) and third quartiles (TRS, 1.7–4.0) and 22% in the first quartile (TRS, 0–1.3). We designated patients with TRS of less than or equal to 1.3 as low risk, TRS of 1.4 to 4.0 as moderate risk, and TRS of greater than or equal to 4.1 as high risk. With these scoring cutoffs, 39% of triaged patients screened as low risk, 39% as moderate risk, and 22% as high risk for HR. Using multiple logistic regression, we found likelihood of HR to be significantly greater for patients screening as high (odds ratio, 5.9) or moderate risk (odds ratio, 1.9; both p < 0.01).
 Figure 2:
Figure 2: Triage risk score calculator.
 Figure 3:
Figure 3: Sensitivity and specificity of additive telephone triage model by probability cutoff.
 Figure 4:
Figure 4: Proportion of HR by TRS (n = 560). HR, moderate to high risk; n, sample size.
DISCUSSIONIn this prospective multisite implementation study, we evaluated development of a cellular telephone screening tool to risk stratify trauma patients in need of further care after discharge in Cameroon. Our data demonstrate that cellular telephones can be used to provide follow-up triage of injured patients who is sensitive in identifying patients at risk of poor outcomes as adjudicated by the criterion standard of Cameroonian physician examination. Overall, we validated eight candidate screening questions that positively associated with HR for future use in telephone triage. Widespread implementation of a telephone triage program could allow patients at the highest risk for poor outcomes to be targeted for additional support and resources. Concentrating limited resources toward ensuring these HR patients have access to follow-up care could minimize avoidable morbidity, economic disability, and mortality in this population. By using cellular telephone contact and nonclinician survey administration, this follow-up program has potential to increase trauma care access while minimizing upfront costs and time commitments of both patients and already strained Cameroonian trauma care providers.
Our findings bolster preliminary pilot data suggesting that telephone survey participation is much more feasible than in-person follow-up in the Cameroonian context,10 with 96% of contacted patients willing to participate in telephone triage compared with only 33% of patients who were willing and able to present for in-person follow-up. While more than 30% of eligible registry patients were contacted for follow-up, the primary objective of this study was to validate the association of survey questions with physician examination. Feasibility of cellphone follow-up will be separately addressed in a forthcoming manuscript. These percentages likely still underestimate the discrepancy between telephone and in-person participation, as study participants received travel compensation to present for in-person examination. As cellular telephone access and familiarity continues to expand in this population, we anticipate that participation in telephone triage will continue to increase. However, given the challenges with getting patients to return for physician examination in this context, broad implementation efforts will need to carefully strategize how best to appropriately target care for those found to have additional needs. Patients who are off-trajectory may face the greatest barriers returning to care. Consideration for alternative care approaches, such as home visits by dedicated physician teams, may be needed to reengage patients and deliver care to patients at the highest risk for poor outcomes. Moreover, other centers can implement these findings to facilitate follow-up in other low-resource contexts. However, we recognize that each LMIC is diverse, and generalizability of our follow-up tool would need to be validated in other LMIC settings. It is likely that there will never be a universal follow-up tool that is functional in all low-resource setting since development of a health intervention requires comprehensive consideration of local resources and needs.
Approximately 2% of the contacted population had died by the second postdischarge week. This substantial early mortality highlights a critical need to develop a bidirectional component of the telephone triage program to provide a mechanism for patients who self-identify as being off-trajectory to trigger evaluation for early care reentry. For example, the vast majority of triaged patients reported improved perceived well-being after hospital discharge, even among the HR cohort. However, the minority of patients who did self-identify as having same or worse perceived well-being were highly likely to be designated as HR. Developing a contact protocol for discharged patients with concerns about their clinical progress to engage formal evaluation may facilitate earlier diagnosis and treatment of complications and improve trauma outcomes. Additional studies are underway to attempt to identify CTR predictors of early postdischarge mortality to better target this population for early surveillance and intervention.
Overall, 6 of the 14 candidate triage questions were not statistically associated with HR and will be eliminated from future triage tool iterations for efficiency. Notably, questions that did not contribute to prediction included the ability to return to normal activities and independently complete ADLs. While functional recovery is a key long-term outcome after trauma, we hypothesize that the 2-week postdischarge time point is premature to expect even on-trajectory patients to have resumed normal activities. Similarly, depending on patient age, health status, and injury type and severity, many discharged patients may reasonably expect to still require assistance with ADLs at 2 weeks following discharge even if recovering as expected. Consequently, these questions are likely poor indicators of need for further care.
Prior community-based data demonstrate that Cameroonian patients have high rates of economic and physical disability after injury.9 We hypothesized that, because Cameroon currently does not enforce standardized accommodations for differently abled persons, fulfilling basic needs like completing expected injury care may present considerable barriers to discharged patients. Perhaps unsurprisingly, we found difficulty obtaining medicine and caring for injury to be associated with HR. Although it is not possible to ascertain with certainty why this is the case, we suspect that the inability to complete these tasks leads to a negative feedback cycle where undertreated patients are less able to heal from injury and continue to ongoing difficulty meeting basic needs.
In contrast, the candidate triage question asking if patients encountered other nonspecified difficulties in care was the only question not tested in the initial single-center feasibility pilot.9 The intention of including this question was less to be an independent predictor but rather to develop potential predictors for subsequent iterations of the triage tool. Interestingly, identifying other barriers to care trended toward a negative association with HR, which we speculate may potentially be because meeting baseline metrics of recovery allows patients and families the bandwidth to consider other, but less impactful barriers to reintegration postdischarge. However, this finding did not achieve the specified criteria for statistical significance, and the “other barriers to care” question will be removed from future iterations of the tool.
Among the questions addressing patients' symptoms, erythema/swelling, pain, difficulty moving/feeling, and opening or drainage from the wound/incision associated with HR, while fever and nausea/vomiting did not. This may be in part because certain symptoms are easier for patients to objectively evaluate with the triage prompts (e.g., redness and wound reopening), whereas others, like fever, may be more subjective difficult for patients to assess in the Cameroonian environment with few home thermometers.
Prior qualitative data have established that Cameroonian patients view different care types including formal care and traditional healers as interchangeable and complementary components of care.23 Seeking further care from any of these sources appears to be associated with physician designation of HR. In additional to its capacity as a screening question, leveraging traditional healers may represent an additional access point to reengage care among patients off trajectory post injury.
Because the consequences of a false-positive survey leading to unnecessary patient follow-up are less consequential, whereas false negatives could result in devastating outcomes for missed patients, our approach was to minimize risk and target a highly sensitive test with few false negatives. Although the AUC value for the overall tool falls slightly below the discrimination threshold in this analysis, the primary outcome of this study is the discrimination of each question rather than the whole tool. Future iterations of the tool will seek to maximize overall discrimination and improve specificity while maintaining sensitivity. We found that a weighted additive score gave the best risk stratification for HR. The next steps will be to use this tool to optimally target the limited existing resources in the Cameroonian context to provide additional care to high-risk patients. While still under development, one reasonable approach might be to (1) recommend in-person follow-up for any patients with any positive response on the eight-question screening survey and (2) target early in-home follow-up for patients screening as high-risk by TRS scores. We do recognize that the initial parameters of screening are poorly specific, which will likely lead to a more resource intensive approach at the outset. However, overtriage is desirable early in screening program implementation to establish effectiveness in improving outcomes; we anticipate that specificity will be further optimized with future iterations of the protocol. Additional prospective data on the effectiveness of the model in reducing long-term morbidity will be the target of future studies.
There are several notable limitations to this study. First, by design, this study seeks to repatriate patients who are already engaged informal care. We know that approximately one third of Cameroonians with severe injury failed to present to formal care and this study does not address increasing access for these patients. Furthermore, another limitation is the selection bias of patients who responded to the follow-up survey and presented for a physical examination. It is possible that patients lost to follow-up were either recovering well, too sick to participate in follow-up, or presented to other facilities out of the study follow-up network. Given the resource constraints and significant barriers associated with care utilization, the latter explanation seems less likely in this context. The two former explanations appear more likely as our study determined a portion of patients to be low risk for a poor outcome (i.e., recovering well) and found a substantial postdischarge death rate (i.e., too sick to travel). The patients who stand to benefit cellular follow-up triage include those patients who already have access and facility using cellular telephones, and this may cluster with less vulnerable populations. Our research group plans to conduct an analysis of socioeconomic, clinical, and qualitative factors that influence patient acceptability of the survey tool and implementation of post discharge follow-up. In addition, as previously highlighted in this discussion, the ability to identify patients in need of further care does not guarantee that the Cameroonian health system will be able to reengage or deliver care to this at-risk cohort. Our hospital return rates demonstrate that presenting to formal care is clearly a barrier for Cameroonian patients, even when travel is compensated and ongoing efforts will be needed to optimize care delivery mechanisms. It is also possible that a portion of patients who recover well from injury do not desire to attend a follow-up examination, but this explanation seems less plausible given the large number of barriers that prevent care access in Cameroon. Finally, we acknowledge that there is opportunity to use registry collected data to further enhance the discrimination and targeting of our triage model.
In conclusion, our study found that telephone triage provides sensitive risk stratification of patients in need of further care after hospital discharge in Cameroon. Given low in-person return rates, limited resources should highly prioritize efforts to repatriate patients screening as high risk for poor outcomes. Expanding implementation of cellular telephone follow-up triage is currently underway at 10 hospitals, providing an opportunity for prospective cross-validation of the model developed here and development of a comprehensive bidirectional follow-up program. Later iterations of the follow-up tool will use the larger patient population to increase tool specificity by incorporating trauma registry data into agnostic machine learning techniques. Furthermore, results from a parallel implementation analysis evaluating call timing, contact metrics, and acceptability will be used to optimize triage uptake in the target population. As discussed in the limitations section previously, next steps also include enhancing efforts to target marginalized vulnerable populations with limited cell phone contact and implement care in patients with limited hospital access. Finally, our findings suggest promise for cellular telephone follow-up screening in other health care capacities.
AUTHORSHIPS.A.C., R.O., R.D., A.C.-M., and C.J. participated in study design. M.M., F.D.-D., F.Y., F.E., G.M., S.A.C., A.C.-M., and C.J. participated in data acquisition. S.A.C., R.O., M.Y., A.C.-M., and C.J. participated in analysis and interpretation of study data. Finally, S.A.C., R.O., M.Y., and C.J. participated in drafting and critical revision of the manuscript.
ACKNOWLEDGMENTResearch reported in this publication was supported by the Fogarty International Center of the National Institutes of Health under award number R21TW010956. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
DISCLOSUREThe authors declare no conflicts of interest.
REFERENCES 1. World Health Organization. The Global Burden of Disease: 2004 Update. Geneva: Switzerland; 2008. World Health Organization. Available at: https://apps.who.int/iris/handle/10665/43942. Accessed January 8, 2023. 2. Mock C, Quansah R, Goosen J, Kobusingye O. Trauma care in Africa: the way forward. Afr J Trauma. 2014;3(1):3. 3. World Bank. World Development Report 2011: Conflict, Security, and Development - Overview (English). World development report. Washington, DC: World Bank Group. Available at: http://documents.worldbank.org/curated/en/806531468161369474/World-development-report-2011-conflict-security-and-development-overview. Accessed January 8, 2023. 4. World Health Organization. Injuries and Violence: The Facts 2014. World Health Organization; 2014. Available at: https://apps.who.int/iris/handle/10665/149798. Accessed January 8, 2023. 5. World Health Organization. Mortality and Global Health Estimates: Global Health Observatory Data 2019. World Health Organization. Published 2019. Available at: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates. Accessed January 8, 2023. 6. Juillard CJ, Stevens KA, Ekeke Monono M, Etoundi Mballa GA, Ngamby MK, et al. Analysis of prospective trauma registry data in Francophone Africa: a pilot study from Cameroon. World J Surg. 2014;38(10):2534–2542. 7. Chichom-Mefire A, Nwanna-Nzewunwa OC, Siysi VV, Feldhaus I, Dicker R, Juillard C. Key findings from a prospective trauma registry at a regional hospital in Southwest Cameroon. PloS One. 2017;12(7):e0180784. 8. Leukhardt WH, Golob JF, McCoy AM, Fadlalla AMA, Malangoni MA, Claridge JA. Follow-up disparities after trauma: a real problem for outcomes research. Am J Surg. 2010;199(3):348–352; discussion 353. 9. Christie SA, Dickson D, Mbeboh SN, Embolo FN, Chendjou W, Wepngong E, et al. Association of health care use and economic outcomes after injury in Cameroon. JAMA Netw Open. 2020;3(5):e205171–e205171. 10. Christie SA, Agbor Mbianyor M, Dissak-Delon FN, Tanjong MM, Chichom-Mefire A, Dicker RA, et al. Feasibility of a cellular telephone follow-up program after injury in sub-Saharan Africa. World J Surg. 2020;44(8):2533–2541. 11. Nsagha DS, Lange I, Fon PN, Nguedia Assob JC, Tanue EA. A randomized controlled trial on the usefulness of mobile text phone messages to improve the quality of care of HIV and AIDS patients in Cameroon. Open AIDS J. 2016;10(1):93–103. 12. Hwa K, Wren SM. Telehealth follow-up in lieu of postoperative clinic visit for ambulatory surgery: results of a pilot program. JAMA Surg. 2013;148(9):823–827. 13. Bell KR, Temkin NR, Esselman PC, Doctor JN, Bombardier CH, Fraser RT, et al. The effect of a scheduled telephone intervention on outcome after moderate to severe traumatic brain injury: a randomized trial. Arch Phys Med Rehabil. 2005;86(5):851–856. 14. Bastawrous A, Armstrong MJ. Mobile health use in low- and high-income countries: an overview of the peer-reviewed literature. J R Soc Med. 2013;106(4):130–142. 15. Colaci D, Chaudhri S, Vasan A. mHealth interventions in low-income countries to address maternal health: a systematic review. Ann Glob Health. 2016;82(5):922–935. 16. Fischer K, Hogan V, Jager A, von Allmen D. Efficacy and utility of phone call follow-up after pediatric general surgery versus traditional clinic follow-up. Perm J. 2015;19(1):11–14. 17. Maslowsky J, Valsangkar B, Chung J, Rasanathan J, Cruz FT, Ochoa M, et al. Engaging patients via mobile phone technology to assist follow-up after hospitalization in Quito, Ecuador. Telemed J E Health. 2012;18(4):277–283. 18. Suffoletto B, Wagner AK, Arenth PM, Calabria J, Kingsley E, Kristan J, et al. Mobile phone text messaging to assess symptoms after mild traumatic brain injury and provide self-care support: a pilot study. J Head Trauma Rehabil. 2013;28(4):302–312. 19. Clari M, Frigerio S, Ricceri F, Pici A, Alvaro R, Dimonte V. Follow-up telephone calls to patients discharged after undergoing orthopaedic surgery: double-blind, randomised controlled trial of efficacy. J Clin Nurs. 2015;24(19–20):2736–2744. 20. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. 21. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–1457. 22. StataCorp. Stata Statistical Software: Release 14. College Station, TX: StataCorp LP; 2015. 23. Dickson DC, Christie SA, Chichom Mefire A, Oben E, Embolo FN, Fonje AN, et al. A qualitative study of transitions between health care settings after injury in Cameroon. J Surg Res. 2019;244:528–539.
Comments (0)