
Remember me

Rectal trauma occurs infrequently,1 which has obscured the determination of its optimal diagnosis and treatment. There are also anatomic nuances to the rectum, divided into intraperitoneal and extraperitoneal components based on the peritoneal reflection. These anatomic distinctions guide injury management.2,3 Injuries to the extraperitoneal rectum are most common (roughly 60% of all rectal injuries), followed by the intraperitoneal rectum (30%) and combined intraperitoneal and extraperitoneal injuries (10%).4,5 Because of the scarcity of relevant and high-quality literature, recent paradigm shifts in management recommendations, and the relatively rare nature of these injuries, the ideal approach to the work-up, and treatment of rectal trauma remains unclear.
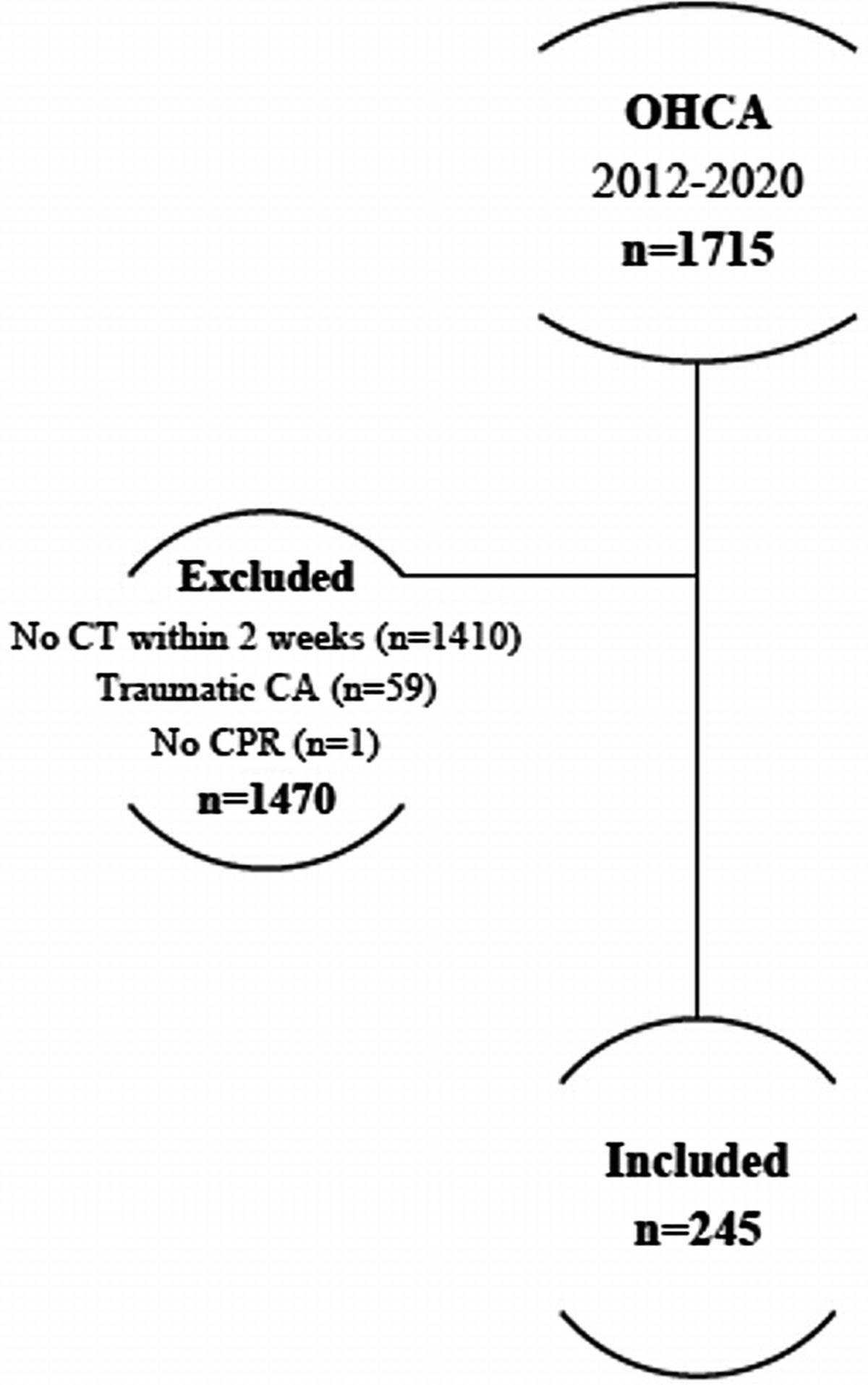
A safe and evidence-based approach to patients with potential traumatic rectal injury is proposed in this article in the form of a diagnostic and management algorithm (Fig. 1) created by the Western Trauma Association (WTA) Algorithms Committee. The management proposed within should be applied to patients with suspected or proven full-thickness rectal injuries (American Association for the Surgery of Trauma [AAST] Grades 2–56). Patients with confirmed partial thickness rectal injuries (AAST Grade 1) do not require intervention.
 Figure 1:
Figure 1: WTA algorithm for the diagnosis and management of traumatic rectal injury. Circled letters correspond to lettered sections in the article text. OR, operating room.
The algorithm process involves initial drafting by the WTA Algorithms committee based on the available literature, extensive revisions by committee members and consideration of expert opinion, and finally, presentation at the annual WTA meeting with commentary and revision based upon expert opinion offered by WTA members and meeting attendees. The letters in the algorithm figure correspond to the lettered sections below, where the evidence and rationale surrounding each portion of the algorithm are discussed in detail. The evaluation and management recommendations are based largely on retrospective cohort studies due to the paucity of randomized controlled trials (RCTs) and other prospective data on the subject. Because of this, the algorithm should be considered as a modifiable framework with which to approach rectal trauma. Adaptations based on clinical judgment, patient factors, hospital resources, and/or injury burden are suggested.
ALGORITHM (A) Screening and Clinical AssessmentTrauma patients with the potential for rectal injury should be approached in the standard fashion for any trauma patient, applying the Advanced Trauma Life Support principles.7 Most (>75%) rectal injuries are secondary to penetrating trauma, of which the vast majority are from gunshot wounds.3,4,8 An early index of suspicion for rectal injury should be raised by the presence of bullet wounds that span the pelvis and, less frequently, by stab wounds to the perineum or lower portion of the buttocks. Rectal injuries after blunt trauma are uncommon and tend to occur as avulsion-type injuries following high-energy mechanisms or as a result of sharp bony fragments associated with pelvic fractures. An additional injury mechanism is trauma due to the insertion of rectal foreign bodies, which typically results in no more than an AAST Grade 1 injury.9 In uncommon instances of full-thickness injury from rectal foreign body insertion, these injuries should be evaluated and treated as any other traumatic mechanism of injury. During the primary and secondary surveys, the physical exam of these patients should focus on identifying these risk factors for rectal injury. Identification of gross hematuria should also increase the clinical concern for rectal injury as approximately one-third of patients with rectal injury have a concomitant bladder injury.10
A digital rectal exam (DRE) has long been considered a standard portion of the initial assessment of any trauma patient. Although some authors have advocated against its routine performance, citing its low sensitivity5,11,12 and the infrequency with which it changes intervention,11,13 it can provide useful information in patients at risk for rectal injury. For example, a DRE that reveals blood and/or a palpable defect has a specificity for rectal injury that approaches 100%.5,12,14 Furthermore, after blunt pelvic fractures, DRE with palpation of bony fragments reveals the presence of an open pelvic fracture shortly after patient arrival and allows the prompt initiation of antibiotics. It should be emphasized that a normal DRE does not exclude rectal injury.5,12,15 A high index of suspicion for rectal injury prior to DRE performance should be maintained regardless of the DRE findings. With these notable caveats, most consider DRE a standard portion of the initial physical examination for patients at risk for rectal injury.
(B) Diagnosis in the Hemodynamically Stable PatientHemodynamically normal patients proceed to the computed tomography (CT) scanner from the trauma bay for an intravenous contrast scan. There is no routine role for rectal contrast administration during CT scan screening for rectal injuries for several reasons. The first is that portions of the extraperitoneal rectum are obscured by the catheter and balloon used for contrast injection and, therefore, cannot be assessed. The second is that extraluminal contrast after rectal contrast CT scan is poorly sensitive for detecting rectal injuries. One recent meta-analysis reported a sensitivity of 12% with a false-negative rate of 88%.16 The third is the additional time needed for administration of rectal contrast, which must be done by a physician in some hospitals. These two features frequently render its administration impractical, especially in busy centers. Last, forced instillation of rectal contrast may contribute to further contamination via an existing rectal injury and increase the risk of local infection or pelvic sepsis. If the CT scan reveals the presence of associated abdominopelvic injuries necessitating surgical intervention (e.g., small bowel, intraperitoneal bladder, etc), diagnosis of the patient's potential rectal injury is pursued under the Hemodynamically Unstable Patient pathway described in the following section.
Computed tomography scans for diagnosis of rectal injury should generally be considered suggestive and not conclusive. A multicenter study of patients with full-thickness rectal injuries demonstrated that among patients who had a CT scan performed, only one-third of these scans were positive for injury with demonstration of rectal wall injury/thickening or perirectal stranding.17 Because of its low diagnostic yield, a CT scan with any suggestion of rectal injury is followed up with endoscopy (i.e., proctosigmoidoscopy) as an adjunctive diagnostic tool to confirm the diagnosis and establish the anatomic location of rectal injury. The combination of CT scan and endoscopy has been shown to have a sensitivity of 97% in the diagnosis of rectal injuries.17
Endoscopy at the anatomic extremes of the rectum will delineate an injury as intra- or extraperitoneal and can be performed with a rigid or flexible scope depending on resource availability. If the injury location is mid-rectum, the anatomic determination of intra- or extraperitoneal location will be challenging, if not impossible, endoscopically. In these cases, diagnostic laparoscopy or laparotomy is used to exclude an intraperitoneal injury component.18–21
(C) Diagnosis in the Hemodynamically Unstable PatientIt cannot be overemphasized that hemorrhage control takes precedence over control of gastrointestinal spillage. Therefore, patients with a suspected rectal injury who are hemodynamically unstable should proceed directly to the operating room for exploratory laparotomy. If the patient is not in extremis and positioning can be accomplished rapidly, lithotomy will facilitate evaluation and potentially management of the rectal injury after bleeding control is obtained. It should be underscored that there are notable disadvantages to positioning a patient in lithotomy, including the time required and obscured groin access. Consequently, for the vast majority of unstable patients, hemorrhage control should proceed via exploratory laparotomy with the patient positioned supine. If access to the perineum and rectum is subsequently needed, the patient can be repositioned afterward as outlined below.
After control of bleeding, the intraperitoneal rectum is assessed for injury via the laparotomy. This is followed by proctoscopy to assess the integrity of the extraperitoneal rectum. If the patient was not placed in lithotomy at the commencement of the case, the patient can be repositioned into lithotomy for proctoscopy. If the clinical suspicion for injury is low, proctoscopy can also be accomplished beneath the drapes with the patient frog-legged. After anatomic delineation of any intraperitoneal and extraperitoneal rectal trauma, injury management ensues.
(D) Management of Intraperitoneal Rectal InjuryIntraperitoneal rectal injuries should be managed similarly to colon injuries. After gaining access to the peritoneal cavity, visual inspection of the intraperitoneal rectal injury determines it to be destructive or nondestructive. In general, destructive injuries are those that are devascularized or with associated mesenteric injury; have large, irregular wall defects; and/or those with extensive injury to the bowel wall, for example, from associated thermal injury after gunshot wound.
Destructive intraperitoneal rectal injuries are typically managed with resection and primary anastomosis.18,22 In contrast, nondestructive injuries are repaired primarily at laparotomy,2 commonly in a transverse orientation and in two layers. In a recent multicenter study, the addition of a proximal diversion to either of these approaches was associated with a significant increase in abdominal complications with no observed benefit and therefore is not routinely recommended.4 However, proximal diversion with a colostomy or protective loop ileostomy may be indicated in select situations based on surgeon assessment of overall injury burden, including consideration of associated injuries and volume of blood loss; patient comorbidities, including diabetes mellitus or steroid use; and patient physiology.
Another scenario where proximal diversion should be considered after repairing an intraperitoneal rectal injury is in the context of identification of a single intraperitoneal rectal injury following a gunshot wound. Because a hollow viscus gunshot wound tends to produce through-and-though injuries, the possibility of a paired extraperitoneal rectal injury is high. Protective diversion is recommended for management of the extraperitoneal injury component as outlined below.
(E) Management of Extraperitoneal Rectal InjuryThe optimal management of extraperitoneal injuries is more controversial and has changed dramatically over the past century. Nonetheless, as with intraperitoneal injuries, the destructive or nondestructive nature of an extraperitoneal injury guides its management. A destructive extraperitoneal injury can be managed with proximal diversion alone without attempts to repair or resect the injury.5,18 This is typically accomplished with a loop sigmoid colostomy, which can be constructed laparoscopically or open based on the patient's associated injuries, clinical status, and the surgeon's judgment.
If the injury is nondestructive, the feasibility of transanal primary repair should be assessed. Depending on the surgeon's familiarity with transanal surgery and the distance from the anorectal junction, the injury may or may not be accessible transanally. If it is, primary repair of the injury without fecal diversion is adequate.1 If a nondestructive injury is inaccessible transanally, proximal diversion alone as described above with a loop sigmoid colostomy is sufficient.23 In some cases, there will be secondary evidence of an extraperitoneal rectal injury on endoscopy with visualization of gross blood or a hematoma but the injury itself is obscured or poorly visualized. In these cases, proximal diversion is generally recommended and further attempts at exposure or dissection of the rectal injury are unnecessary.
For those patients who undergo proximal diversion, the ideal timing of colostomy reversal is controversial. In terms of broad principles, the patient should fully recover from the traumatic injuries and be optimized nutritionally prior to colostomy closure. Most surgeons evaluate the rectal integrity with a contrast enema before reversal. However, the utility of this investigation has not been studied among trauma patients specifically and is controversial among patients undergoing ostomy reversal after elective resections despite historically being considered the gold standard investigation.24,25 If there is any question about rectal integrity on contrast enema, or if the injury was particularly destructive, one can consider flexible sigmoidoscopy to visualize the area of injury and ensuring healing prior to stoma reversal.
Conventionally, it was thought that a several month interval after injury was necessary before ostomy reversal.26 There are now studies supporting colostomy reversal after trauma from periods extending from index admission27,28 to less than 3 months post-injury.29,30 Therefore, the timing of colostomy reversal after rectal trauma should be individualized according to patient factors and overall burden of injury but generally approached within weeks to months after trauma. For patients with complex colorectal injuries, associated perineal/sphincter injuries, or an anticipated hostile abdomen, ostomy reversal may be contraindicated and should not be performed in the early setting.
OTHER AREAS OF CONTROVERSYThere are several remaining controversies in the diagnosis and management of rectal trauma. Table 1 summarizes the existing research deficits identified during algorithm preparation, two of which are explored in more detail in this section.
TABLE 1 - Identified Research Gaps in Rectal Trauma Subject/Knowledge Deficit Algorithm Section (1) Definition of the specific role and diagnostic yield of DRE in initial patient evaluation. A (2) Determination of the relative utility of rigid vs. flexible proctosigmoidoscopy. B (3) Delineation of the role for adjunctive proximal diversion after resection or repair of an intraperitoneal rectal injury. D (4) Definition of the specific subset of patients, if any, with extraperitoneal rectal injuries who may benefit from adjunctive presacral drain insertion. E (5) Further investigation of the specific subset of patients who may be candidates for nonoperative management after penetrating nondestructive extraperitoneal rectal injury. E (6) Determination of the optimal timing of colostomy reversal among patients who undergo proximal diversion for rectal injury management. EPresacral drainage has long been considered a central tenet of extraperitoneal rectal injury management. This concept emerged from examining combat-related rectal injuries during the First and Second World Wars, during which a dramatic reduction in mortality among patients with rectal injury was attributed to the routine use of fecal diversion and presacral drainage.8,31 Further wartime experience with these injuries during the Vietnam War confirmed the benefits of diversion and drainage, and added distal rectal washout which was associated with further reductions in mortality and infectious complications.32–34
These military data were extrapolated and adopted into the care of civilian rectal injuries, with early results that were generally positive. One original civilian study showed a mortality benefit with the routine use of diversion and presacral drainage.35 Another demonstrated that failure to drain the presacral space was associated with a significant increase in infectious complications. However, no impact on mortality or any benefit from distal rectal washout was identified.8 A study published the same year advocated the opposite and demonstrated that distal rectal washout was associated with dramatic decreases in infectious complications following rectal injury, potentially related to a reduction in bacterial translocation from organisms within the gastrointestinal tract.36 Despite these controversies, diversion, direct repair, distal rectal washout, and presacral drainage were considered the standard of care for extraperitoneal rectal injuries for decades.
As data slowly accrued among the civilian subset, the benefit of these interventions became less clear. In particular, the utility of distal rectal washout appeared minimal or nonexistent,8,37,38 and it gradually fell out of favor. Contemporary studies began to question the utility of presacral drainage and failed to demonstrate a clear benefit from the intervention.39–41 An RCT of 48 patients with penetrating extraperitoneal rectal injuries published in 1998 showed no impact on infectious complications from presacral drainage and recommended the technique be abandoned.42 An Eastern Association for the Surgery of Trauma practice management guideline on nondestructive penetrating extraperitoneal injuries recommended against the routine use of distal rectal washout or presacral drainage.23 This was followed by an AAST-sponsored multicenter trial on rectal injuries that revealed presacral drainage with or without distal rectal washout was independently associated with an increase in infectious complications and recommended the abandonment of these techniques.4
Presacral drainage and especially distal rectal washout are now rarely used in clinical practice. A small and highly select group of patients may benefit from the addition of presacral drainage,43 although these patients are not empirically delineated. Such patients may include those likely to be intolerant of sepsis such as the elderly or comorbid, or patients with certain injury morphologies, such as large rectal wall defects implying a greater degree of fecal spillage into the presacral space. For the majority of patients, however, data support the abandonment of presacral drains from extraperitoneal rectal injury management.
Nonoperative Management of Small Penetrating Extraperitoneal Rectal InjuriesThe absolute necessity of diverting or repairing small penetrating extraperitoneal rectal injuries, particularly following stab wounds, is unknown.44 Anecdotally, a nonoperative approach to these injuries appears safe at centers versed in the nonoperative management of abdominopelvic trauma, but very limited data support this approach. In 2006, Gonzalez et al.45 studied 14 consecutive patients admitted with penetrating extraperitoneal rectal injuries managed nonoperatively. Compared to historical controls who underwent operative management, the nonoperatively managed patients had shorter hospital lengths of stay by a mean of 2 days, and none developed complications related to the rectal injury.45 These findings are provocative and will be an area for future investigation in the management of rectal injuries. However, diversion or repair remains the standard of care for penetrating extraperitoneal rectal injuries until more data are amassed.
SUMMARYRectal trauma is uncommon, hindering clinical experience with these injuries and rendering high-quality scientific examination of diagnostic and management options challenging. In general, hemodynamically normal patients at risk for rectal injury based on injury mechanism, trajectory, and associated injuries proceed to the CT scanner for IV contrast scans of the abdomen and pelvis. If concern for rectal injury persists based on a CT scan, proctoscopy is the next step in rectal evaluation. Hemodynamically abnormal patients proceed directly to the operating room for hemorrhage control, followed by assessment of the intraperitoneal rectum via laparotomy and of the extraperitoneal rectum via proctoscopy. Regardless of the patient's hemodynamic status, management is then pursued once the injury has been delineated as intraperitoneal or extraperitoneal. Intraperitoneal rectal injuries are managed as colon injuries and extraperitoneal rectal injuries are generally treated with proximal diversion as a loop sigmoid colostomy alone. Several areas of remaining controversy exist and will require further study, including the optimal time for colostomy reversal; the persistent role, if any, for presacral drainage; and the possibility of nonoperative management for small, nondestructive penetrating extraperitoneal rectal injuries.
AUTHORSHIPAll authors meet authorship criteria for this article as described below. All authors have seen and approved the final article as submitted. The first author (M.S.) had full access to all data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. M.S. and M.J.M. participated in the conception and design. M.S. participated in the acquisition of data. M.S., S.K., M.dM., L.J.M., C.V.R.B., J.L.H., K.I., E.J.L., N.K., K.A.P., C.J.F., N.G.R., J.A.W., R.C., and M.J.M. participated in the analysis and interpretation of data. M.S., M.J.M. participated in the drafting of the article. S.K., M.dM., L.J.M., C.V.R.B., J.L.H., K.I., E.J.L., N.K., K.A.P., C.J.F., N.G.R., J.A.W., and R.C. participated in the critical revision of the article. M.J.M. participated in the supervision.
DISCLOSUREThe authors declare no funding or conflicts of interest.
REFERENCES 1. Gash KJ, Suradkar K, Kiran RP. Rectal trauma injuries: outcomes from the U.S. National Trauma Data Bank. Tech Coloproctol. 2018;22(11):847–855. 2. Weinberg JA, Fabian TC, Magnotti LJ, Minard G, Bee TK, Edwards N, et al. Penetrating rectal trauma: management by anatomic distinction improves outcome. J Trauma. 2006;60(3):508–513. 3. McGrath V, Fabian TC, Croce MA, Minard G, Pritchard FE. Rectal trauma: management based on anatomic distinctions. Am Surg. 1998;64(12):1136–1141. 4. Brown CVR, Teixeira PG, Furay E, Sharpe JP, Musonza T, Holcomb J, et al. Contemporary management of rectal injuries at level I trauma centers: the results of an American Association for the Surgery of Trauma multi-institutional study. J Trauma Acute Care Surg. 2018;84(2):225–233. 5. Schellenberg M, Inaba K, Priestley EM, Durso J, Wong MD, Lam L, et al. The diagnostic yield of commonly used investigations in pelvic gunshot wounds. J Trauma Acute Care Surg. 2016;81(4):692–698. 6. Moore EE, Cogbill TH, Malangoni MA, Jurkovich GJ, Champion HR, Gennarelli TA, et al. Organ injury scaling, II: pancreas, duodenum, small bowel, colon, and rectum. J Trauma. 1990;30(11):1427–1429. 7. American College of Surgeons. Advanced Trauma Life Support. 2023. Available at https://www.facs.org/quality-programs/trauma/education/advanced-trauma-life-support/?page=1. Accessed March 30, 2023. 8. Burch JM, Feliciano DV, Mattox KL. Colostomy and drainage for civilian rectal injuries: is that all? Ann Surg. 1989;209(5):600–610. 9. Schellenberg M, Brown CVR, Trust MD, Sharpe JP, Musonza T, Holcomb J, et al. Rectal injury after foreign body insertion: secondary analysis from the AAST Contemporary Management of Rectal Injuries Study Group. J Surg Res. 2020;247:541–546. 10. Osterberg EC, Veith J, Brown CVR, Sharpe JP, Musonza T, Holcomb JB, et al. Concomitant bladder and rectal injuries: results from the American Association for the Surgery of Trauma Multicenter Rectal Injury Study Group. J Trauma Acute Care Surg. 2020;88(2):286–291. 11. Beeton G, Alter N, Zagales R, Wajeeh H, Elkbuli A. The benefits and clinical application of the digital rectal exam in trauma populations: towards enhancing patient safety and quality outcomes. Am J Emerg Med. 2023;63:132–137. 12. Shlamovitz GZ, Mower WR, Bergman J, Crisp J, DeVore HK, Hardy D, et al. Poor test characteristics for the digital rectal examination in trauma patients. Ann Emerg Med. 2007;50(1):25–33. 13. Esposito TJ, Ingraham A, Luchette FA, Sears BW, Santaniello JM, Davis KA, et al. Reasons to omit digital rectal exam in trauma patients: no fingers, no rectum, no useful additional information. J Trauma. 2005;59(6):1314–1319. 14. Hargraves MB, Magnotti LJ, Fischer PE, Schroeppel TJ, Zarzaur BL, Fabian TC, et al. Injury location dictates utility of digital rectal examination and rigid sigmoidoscopy in the evaluation of penetrating rectal trauma. Am Surg. 2009;75(11):1069–1072. 15. Mangiante EC, Graham AD, Fabian TC. Rectal gunshot wounds. Management of civilian injuries. Am Surg. 1986;52(1):37–40. 16. Nguyen J, Bashan KA, Jiang C, Lin M, Tootla Y, Udobi K, et al. Rectal contrast CT scans of limited utility in diagnosing colonic injuries in penetrating trauma: a meta-analysis. Am Surg. 2022; Epub ahead of print;000313482210867. 17. Trust MD, Veith J, Brown CVR, Sharpe JP, Musonza T, Holcomb J, et al. Traumatic rectal injuries: is the combination of computed tomography and rigid proctoscopy sufficient? J Trauma Acute Care Surg. 2018;85(6):1033–1037. 18. Biffl WL, Moore EE, Feliciano DV, Albrecht RM, Croce MA, Karmy-Jones R, et al. Management of colorectal injuries: a Western Trauma Association critical decisions algorithm. J Trauma Acute Care Surg. 2018;85(5):1016–1020. 19. Navsaria PH, Shaw JM, Zellweger R, Nicol AJ, Kahn D. Diagnostic laparoscopy and diverting sigmoid loop colostomy in the management of civilian extraperitoneal rectal gunshot injuries. Br J Surg. 2004;91(4):460–464. 20. Navsaria PH, Graham R, Nicol A. A new approach to extraperitoneal rectal injuries: laparoscopy and diverting loop sigmoid colostomy. J Trauma. 2001;51(3):532–535. 21. Namias N, Kopelman T, Sosa JL. Laparoscopic colostomy for a gunshot wound to the rectum. J Laparoendosc Surg. 1995;5(4):251–253. 22. Demetriades D, Murray JA, Chan L, Ordoñez C, Bowley D, Nagy KK, et al. Penetrating colon injuries requiring resection: diversion or primary anastomosis? An AAST prospective multicenter study. J Trauma. 2001;50(5):765–775. 23. Bosarge PL, Como JJ, Fox N, Falck-Ytter Y, Haut ER, Dorion HA, et al. Management of penetrating extraperitoneal rectal injuries: an Eastern Association for the Surgery of Trauma practice management guideline. J Trauma Acute Care Surg. 2016;80(3):546–551. 24. Lindner S, Eitelbuss S, Hetjens S, Gawlitza J, Hardt J, Seyfried S, et al. Less is more-the best test for anastomotic leaks in rectal cancer patients prior to ileostomy reversal. Int J Color Dis. 2021;36(11):2387–2398. 25. Farzaneh CA, Jafari MD, Duong WQ, Grigorian A, Carmichael JC, Mills SD, et al. Evaluation of pelvic anastomosis by endoscopic and contrast studies prior to ileostomy closure: are both necessary? A Single Institution Review. Am Surg. 2020;86(10):1296–1301. 26. Parks SE, Hastings PR. Complications of colostomy closure. Am J Surg. 1985;149(5):672–675. 27. Khalid MS, Moeen S, Khan AW, Arshad R, Khan AF. Same admission colostomy closure: a prospective, randomised study in selected patient groups. Surgeon. 2005;3(1):11–14. 28. Renz BM, Feliciano DV, Sherman R. Same admission colostomy closure (SACC). A new approach to rectal wounds: a prospective study. Ann Surg. 1993;218(3):279–292; discussion 292-3. 29. Velmahos GC, Degiannis E, Wells M, Souter I, Saadia R. Early closure of colostomies in trauma patients—a prospective randomized trial. Surgery. 1995;118(5):815–820. 30. Demetriades D, Pezikis A, Melissas J, Parekh D, Pickles G. Factors influencing the morbidity of colostomy closure. Am J Surg. 1988;155(4):594–596. 31. Taylor ER, Thompson JE. The early treatment, and results thereof, of injuries of the colon and rectum. Internat Abstr Surg. 1948;87:209–228. 32. Lavenson GS, Cohen A. Management of rectal injuries. Am J Surg. 1971;122(2):226–230. 33. Ganchrow MI, Lavenson GS Jr., McNamara JJ. Surgical management of traumatic injuries of the colon and rectum. Arch Surg. 1970;100(4):515–520. 34. Lung JA, Turk RP, Miller RE, Eiseman B. Wounds of the rectum. Ann Surg. 1970;172:985–990. 35. Trunkey D, Hays RJ, Shires GT. Management of rectal trauma. J Trauma. 1973;13(5):411–415. 36. Shannon FL, Moore EE, Moore FA, McCroskey BL. Value of distal colon washout in civilian rectal trauma–reducing gut bacterial translocation. J Trauma. 1988;28(7):989–994. 37. Bostick PJ, Johnson DA, Heard JF, Islas JT, Sims EH, Fleming AW, et al. Management of extraperitoneal rectal injuries. J Natl Med Assoc. 1993;85(6):460–463. 38. Tuggle D, Huber PJ Jr. Management of rectal trauma. Am J Surg. 1984 Dec;148(6):806–808. 39. Savoie KB, Beazley TM, Cleveland B, Khaneki S, Markel TA, Hammer PM, et al. The utility of presacral drainage in penetrating rectal injuries in adult and pediatric patients. J Surg Res. 2017;219:279–287. 40. Navsaria PH, Edu S, Nicol AJ. Civilian extraperitoneal rectal gunshot wounds: surgical management made simpler. World J Surg. 2007;31(6):1345–1351. 41. Velmahos GC, Gomez H, Falabella A, Demetriades D. Operative management of civilian rectal gunshot wounds: simpler is better. World J Surg. 2000;24(1):114–118. 42. Gonzalez RP, Falimirski ME, Holevar MR. The role of presacral drainage in the management of penetrating rectal injuries. J Trauma. 1998;45(4):656–661. 43. Uchino H, Kong V, Elsabagh A, Laing G, Bruce J, Manchev V, et al. Contemporary management of rectal trauma—a South African experience. Injury. 2020;51(5):1238–1241. 44. Emigh B, Inaba K, Schellenberg M. Contemporary diagnosis and management of traumatic rectal injuries. Surg Pract Sci. 2021;10024:100024. 45. Gonzalez RP, Phelan H 3rd, Hassan M, Ellis CN, Rodning CB. Is fecal diversion necessary for nondestructive penetrating extraperitoneal rectal injuries? J Trauma. 2006;61(4):815–819.
Comments (0)