
Remember me

Infection prevention and control are fundamental patient safety practices and healthcare quality indicators.1 To mitigate infection risk, healthcare workers (HCWs) must comply with standard infection control measures, such as ensuring hand hygiene before and after all care practices and using personal protective equipment (PPE) in case of contact with blood or bodily fluids.2 Common PPE includes gloves, medical masks, particle-filtering masks with or without valves, N95 masks, goggles, face shields, and gowns.2,3
Since the beginning of the COVID-19 pandemic, HCWs have undertaken important duties to protect and maintain public health and provide safe treatment of patients.6 The importance of PPE use in healthcare institutions has increased because of the need to control the transmission of COVID-19 infection. Healthcare workers have had to use PPE during long working hours to prevent virus transmission,7,8 which has led to PPE-related skin problems on the face.9–11 Moreover, in addition to skin integrity problems, long-term use of PPE also affects HCWs’ daily work performance and comfort.9,12,13
Multiple studies have found high rates of skin injury among HCWs due to PPE use.8,9,12–15 In a multicenter, cross-sectional survey study in China (N = 4,306), Jiang et al9 found that 42.8% of participants experienced skin injury due to PPE use. Similarly, Yıldız et al12 found a skin injury rate of 47.9% among HCWs (N = 48) in the COVID-19 unit in a public hospital in Turkey. Abiakam et al13 found a PPE-related skin injury rate of 88.0% among HCWs (N = 307) from the National Health System in England who worked in clinics where patients with COVID-19 received care.
In addition to skin injury, HCWs also experience other PPE-related problems. In an international survey study (N = 2,711), Tabah et al14 uncovered a number of problems related to the use of PPE in ICUs, including heat (51.0%), thirst (47.0%), pressure areas (44.0%), headache (28.0%), inability to use the bathroom (27.0%), and extreme fatigue (20.0%).14 In the study by Duan et al,8 97.0% of the 104 HCWs surveyed reported discomfort and injuries caused by wearing PPE for long hours. Participants reported having breathing problems (20.0%), fatigue (16.0%), pressure injuries (PIs; 13.0%), anxiety (12.0%), acne (10.0%), insomnia (7.0%), depression (6.0%), and allergic rash (4.0%).8 In the mixed-type qualitative appraisal study by Hoernke et al,15 HCWs stated that their goggles fogging while performing procedures such as intubation and anesthesia is frustrating and stressful.15
Several factors contribute to reduced facial skin integrity as a result of PPE use. The PPE production materials play a role: hard edges, rigid frames, and ear straps create constant pressure and friction.16 In addition, moisture accumulation (eg, sweat, condensation) creates microclimate changes that reduce the integrity of the stratum corneum and increase the skin’s susceptibility to irritation.9,14 Further, because PPE is mass-produced in standard designs, it is difficult to adapt these items to different face shapes and sizes.10,11 These factors all increase the risk of skin injury, particularly in individuals with sensitive skin.17
Various interventions have been proposed to help prevent facial skin injuries due to the use of PPE during the COVID-19 pandemic. In particular, leading professional organizations published practice recommendations to guide all HCWs working under pandemic conditions in the prevention and maintenance of skin integrity.18–21 In addition, international consensus reports and expert opinions10,11,22 in line with these recommendations and PI guidelines16,23 have been helpful resources in meeting the information needs of HCWs. Recommended interventions include limiting the daily use of PPE as much as possible, using thin and sensitive hydrocolloid or silicone foam dressings under the areas where PPE comes into contact with the skin, applying barrier skin care products, and increasing the tolerance of the skin with daily skin cleaning and care.10,12,18 These preventive measures are also among the recommended best practices to increase tissue tolerance in the prevention of medical device-related PIs.16,23
Relevant literature on this topic primarily focuses on identification of skin injuries, prevention and management of PIs due to PPE use, and practice guidelines prepared by professional organizations.16,18 Studies examining the PPE-related personal experiences of HCWs, their recommendations for solutions to PPE-related problems, and their suggestions for improving the quality of PPE are limited. The purpose of the present study was to determine (1) the problems experienced by HCWs who use PPE on their face (eg, mask, goggles, face shield), (2) the interventions they use to prevent these problems, and (3) their recommendations for improving the quality of PPE.
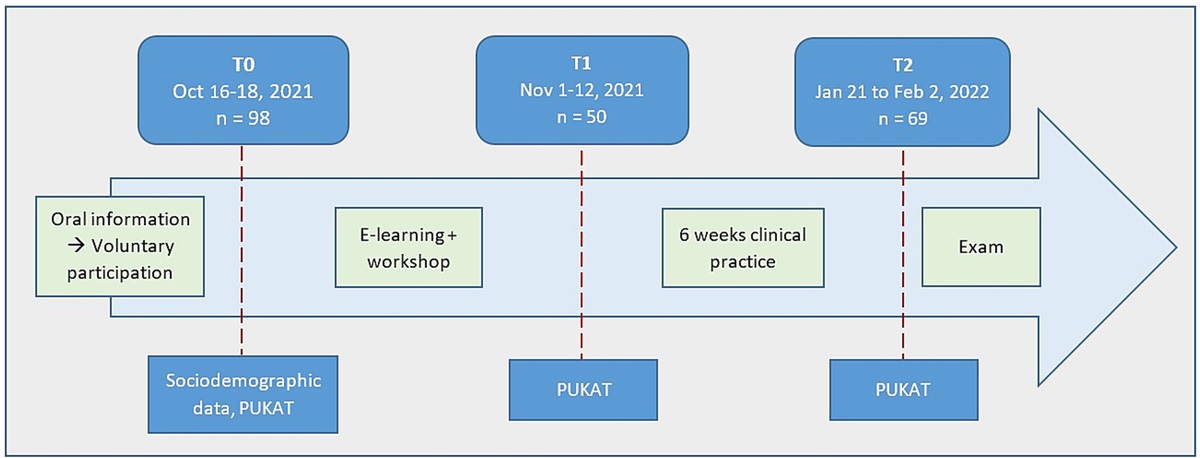
METHODS Study ParticipantsIn this descriptive, qualitative study, the researchers used purposive sampling24 with no exclusion criteria to assemble the research sample. The researchers leveraged their professional communication network and asked colleagues to refer potential participants. Those referrals were then contacted by phone or email. Participants included nurses, physicians, and other HCWs working in different health institutions at various levels in Turkey.
Data Collection ToolBased on the literature,9,14,16 the authors created a semistructured data collection form that consisted of a total of 13 questions. This form includes six demographic questions and seven open-ended items regarding the problems experienced by HCWs because of PPE use, recommendations to prevent and solve these problems, and their views on improving the quality of PPE.
Data Collection MethodData were collected during individual participant interviews that took place between March 16, 2021 and May 28, 2021. Interviews were conducted either face-to-face or via social media communication platforms (Zoom, WhatsApp, and Skype). With the permission of the participants, interviews were recorded by audio recording or note-taking. Two authors conducted all interviews together, with one author asking the questions and the other taking notes and filling out the data collection form. Afterward, two authors transcribed the audio recordings and verified the data. The same data collection form was used in all interviews.
Data AnalysisData were analyzed with descriptive statistics: frequency and percentage were calculated for categorical data, and mean and SD were calculated for continuous numerical data. The researchers evaluated participants’ answers to the open-ended questions by qualitative inductive content analysis.25
In the inductive content analysis process, the researchers first transcribed the audio recordings and written notes for each participant interview. All responses were entered in an Excel file (Microsoft Corp). The researchers then focused on the content of the question and relevant literature information on the subject9,11,12,26 for each answer to identify units of meaning. Condensed meaning units that could be used interchangeably were coded under more inclusive concepts and divided into subcategories. Subcategories were then combined to create main categories (Figure 1).25 In terms of reliability and consistency, two authors who are experts in qualitative research independently carried out this process and agreed on the results. The authors who conducted the inductive content analysis process are specialized in stoma and wound care nursing and infection control, and the categorizations determined were in line with the relevant literature.9,11,12,26
 Figure 1.:
Figure 1.: STAGES OF QUALITATIVE INDUCTIVE CONTENT ANALYSIS
Ethical ConsiderationsThe researchers obtained approval from the university ethics committee before conducting the study. All participants provided verbal informed consent agreeing to participate in the study before being interviewed.
RESULTS Descriptive Characteristics of the ParticipantsA total of 29 HCWs (15 women) participated in this study The majority of participants were nurses (n = 18); of the remaining participants, nine were physicians, one was a dentist, and one was a dialysis technician. Overall, 24.1% of the participants stated that they worked in a COVID-19 unit, 75.9% received training for the use of PPE, and 65.5% reported that their institution had a PPE usage protocol (Table 1).
Table 1. - PARTICIPANT CHARACTERISTICS Variable n (%) Sex Female 15 (51.7) Male 14 (48.3) Occupation Nurse 18 (62.1) Physician 9 (31.0) Othera 2 (6.9) Highest degree received Bachelor’s degree 15 (51.7) Specialty in medicine 9 (31.0) Master’s degree 3 (10.3) Associate 2 (6.9) Work unit OR 7 (24.1) COVID unit 7 (24.1) Outpatient clinic 5 (17.2) General surgery 4 (13.8) Internal medicine clinics 4 (13.8) Intensive care clinic 2 (6.9) Training on use of PPE Yes 22 (75.9) No 7 (24.1) PPE usage protocol in institution of employment Yes 19 (65.5) No 8 (27.6) Do not know 2 (6.9) Variable Mean (SD) Range Age, y 34.14 (10.41) 23–58 Employment duration, y 9.60 (8.06) 1–28 Duration of daily PPE use, h Surgical/medical mask 11.90 (6.17) 1–24 N95 mask 5.49 (8.57) 1–24 Goggles 2.15 (3.82) 1–16 Face shield 1.91 (4.25) 1–16 Frequency of changing PPE in daily use, h Surgical/medical mask 2.72 (2.00) 1–9 N95 mask 2.91 (4.11) 1–14 Goggles 1.09 (1.90) 1–8 Face shield 1.22 (1.88) 1–8Abbreviation: PPE, personal protective equipment.
aOne dentist, one dialysis technician.
In terms of daily PPE use, participants spent a mean of 11.86 ± 6.17 hours wearing a surgical/medical mask, 5.49 ± 8.58 hours wearing an N95 mask, 2.15 ± 3.18 hours wearing goggles, and 1.91 ± 4.25 hours wearing a face shield. Participants reported changing surgical/medical masks a mean of every 2.72 ± 2.00 hours in daily use. They changed N95 masks after a mean of 2.91 ± 4.11 hours, goggles after a mean of 1.09 ± 1.91 hours, and face shields after a mean of 1.22 ± 1.88 hours (Table 1).
PPE-related Problems Experienced by ParticipantsThe researchers grouped participants’ responses regarding the problems they experienced while using PPE into four main categories: skin problems, physical effects, functional effects, and psychological effects. These main categories and subcategories are shown in Table 2.
Table 2. - PROBLEMS WITH PPE USE EXPERIENCED BY PARTICIPANTS Main Category Mask Problems Subcategories (n = 130) n (%) Goggles Problems Subcategories (n = 47) n (%) Face Shield Problems Subcategories (n = 28) n (%) Skin problems Wound formation in contact areas 17 (22.7) Marks around the eyes 3 (37.5) Marks on forehead 3 (60.0) Acne formation 15 (20) Wound formation in contact areas 3 (37.5) Redness on forehead 1 (20.0) Marks in contact areas 13 (17.3) Redness at contact areas 2 (25.0) Wound formation on forehead 1 (20.0) Allergy-itching-rash 13 (17.3) Redness at contact areas 8 (10.7) Chapped lips 3 (4.0) Hair growth 3 (4.0) Dryness and sores in the mouth 2 (2.7) Spot formation 1 (1.3) Total 75 (57.7) 8 (17.0) 5 (17.9) Physical effects Discomfort in breathing 18 (46.2) Pressure and pain in contact areas 5 (71.4) Pressure and pain in contact areas 4 (50.0) Pressure and pain in contact areas 10 (25.6) Headache 2 (28.6) Headache 4 (50.0) Nasal dryness and congestion 5 (12.8) Sweating and moisture around the mouth 5 (12.8) Headache 1 (2.6) Total 39 (30.0) 7 (14.9) 8 (28.6) Functional effects Poor fit on face 4 (50.0) Fogging 15 (48.4) Obstructing the vision 7 (46.7) Fogging on prescription eyeglasses 2 (25.0) Obstructing the vision 10 (32.3) Undermining the sterility 6 (40.0) Smell 1 (12.5) Undermining the sterility 4 (12.9) Difficulty during the procedures 1 (6.7) Difficulty in meeting basic needs (eating and drinking) 1 (12.5) Difficulty in using prescription eyeglasses 2 (6.5) Fogging 1 (6.7) Total 8 (6.2) 31 (66.0) 15 (53.6) Psychological effects Lack of concentration 4 (50.0) Lack of concentration 1 (100) Anxiety 3 (37.5) Fatigue 1 (12.5) Total 8 (6.2) 1 (2.1) 0 (0.0)Abbreviation: PPE, personal protective equipment.
The skin problems category comprised 57.7% of the problems related to the use of masks, 17.0% of the problems related to the use of goggles, and 17.9% of the problems related to the use of a face shield. Among the subcategories for these problems, wound formation in contact areas with mask use (22.7%), marks around the eyes and wound formation in contact areas with the use of goggles (37.5%), and marks on the forehead with face shield use (60.0%) were the problems reported most frequently.
The physical effects category included 30.0% of the problems related to mask use, 14.9% of the problems related to the use of goggles, and 28.6% of the problems related to the use of a face shield. Among the physical effects subcategories, discomfort in breathing with mask use (46.2%), pressure and pain in contact areas with goggles use (71.4%), and pressure and pain in contact areas and headache with face shield use (50.0%) were reported most often.
The functional effects category included 6.2% of the reported problems related to the use of masks, 66.0% of the problems related to the use of goggles, and 53.6% of the problems related to the use of a face shield. The subcategories mentioned most often were poor fitting on face (50.0%) in mask use, fogging (48.4%) in goggles use, and obstructing the vision (46.7%) in face shield use.
The psychological effects category included 6.2% of the problems related to mask use and 2.1% of the problems related to goggle use. Among the psychological effects subcategories, lack of concentration (50.0%) and anxiety (37.5%) with mask use were prominent statements.
Reported Interventions to Prevent PPE-related ProblemsResearchers grouped participants’ responses regarding preventive actions related to PPE use into three main categories: skin protection and care, applications for use, and general applications. These main categories and associated subcategories are listed in Table 3.
Table 3. - INTERVENTIONS TO PREVENT THE PROBLEMS EXPERIENCED WITH PPE USE Intervention Category Mask-related Subcategories (n = 53) n (%) Goggles-related Subcategories (n = 32) n (%) Face Shield-related Subcategories (n = 28) n (%) Skin protection and care Applying moisturizer (cream, petroleum jelly, barrier cream) to contact areas 17 (54.8) Applying a protective cover (cotton, sponge, plaster, hydrocolloid, foam) to contact areas 6 (75.0) Applying a protective barrier (napkin, sponge) to contact areas 2 (66.7) Applying a protective cover (cotton, hydrocolloid, foam) to contact areas 8 (25.8) Changing the sterilization method 1 (12.5) Applying moisturizer (cream) to contact areas 1 (33.3) Washing skin with special soap or gel 5 (16.1) Applying moisturizer (cream) to contact areas 1 (12.5) Performing a skin examination 1 (3.2) Total 31 (58.5) 8 (25.0) 3 (10.7) Applications for use Increasing mask replacement frequency 7 (58.3) Cleaning goggle lenses with soap and disinfectant to prevent fogging 3 (75.0) Using goggles instead of face shield 2 (66.7) Attaching an ear saver strap to the mask straps 3 (25.0) Using face shield instead of goggles 1 (25.0) Frequent removal 1 (33.3) Removing the mask wires 1 (8.3) Using a mask with thick straps 1 (8.3) Total 12 (22.6) 4 (12.5) 3 (10.7) General applications Using a nasal spray and mouthwash 4 (40.0) No intervention 14 (70.0) No intervention 17 (77.3) Applying to dermatology clinic 3 (30.0) Not using goggles 6 (30.0) Not using face shield 5 (22.7) No intervention 3 (30.0) Total 10 (18.9) 20 (62.5) 22 (78.6)Abbreviation: PPE, personal protective equipment.
Interventions in the skin protection and care category encompassed 58.5%, 25.0%, and 10.7% of preventive measures for mask use, goggles use, and face shield use, respectively. Among the subcategories, applying moisturizer (cream, petroleum jelly, barrier cream) to contact areas with mask use (54.8%), applying a protective cover (cotton, sponge, plaster, hydrocolloid, foam) to contact areas with goggles use (75.0%), and applying a protective barrier (napkin, sponge) to contact areas with face shield use (66.7%) were the most frequently used interventions.
In the category of applications for use, interventions were applied at a rate of 22.6% in mask use, 12.5% in goggles use, and 10.7% in face shield use. Among the subcategories for this category, frequency of mask change (58.3%), cleaning goggles’ lenses with soap and disinfectant to prevent fogging (75.0%), and using goggles instead of a face shield (66.7%) were the most frequently used interventions.
In the category of general applications, interventions were applied at a rate of 18.9% in mask use, 62.5% in goggles use, and 78.6% in face shield use. Although most participants did not report any interventions for goggles (70.0%) or face shield (77.3%) use in this category, some listed not using goggles (30.0%) or a face shield (22.7%) as an intervention.
Recommendations for Improving the Quality of PPEParticipants’ responses regarding how to improve the quality of PPE were grouped into three main categories: production materials and quality, product size, and functional properties (Table 4).
Table 4. - PARTICIPANT RECOMMENDATIONS FOR IMPROVING THE QUALITY OF PPE Recommendation Category Mask Recommendation Subcategories (n = 104) n (%) Goggles Recommendation Subcategories (n = 61) n (%) Face Shield Recommendation Subcategories (n = 52) n (%) Production material and quality Use materials (eg, soft and flexible ear straps, silicone protective layer) that do not cause pressure and friction in contact areas 32 (45.1) Production in sterile and disposable packages 26 (56.5) Production in sterile and disposable packages 26 (63.4) Production in sterile and disposable packages 26 (36.6) Use soft materials that do not cause pressure and friction in contact areas 20 (43.5) Use soft materials that do not cause pressure or friction in contact areas 15 (36.6) Soft and hypoallergenic mask contact material 12 (16.9) Should not cause smell 1 (1.4) Total 71 (68.3) 46 (75.4) 41 (78.8) Product size Production in different sizes to suit every face type 15 (93.8) Production in different sizes to suit every face type 4 (100) Production in different sizes to suit every face type 11 (100) Individual size adjustment 1 (6.3) Total 16 (15.4) 4 (6.6) 11 (21.2) Functional properties High level of protection 13 (76.5) Should not cause fogging 11 (100) Easy breathing 4 (23.5) Total 17 (16.3) 11 (18.0) 0 (0.0)Abbreviation: PPE, personal protective equipment.
The category of production materials and quality included 68.3% of recommendations for masks, 75.4% of recommendations for goggles, and 78.8% of recommendations for face shields. Using materials (soft and flexible ear straps, silicone protective layer, etc) that do not cause pressure and friction in contact areas was the most frequently expressed recommendation for masks (45.1%), whereas production in sterile and disposable packages was the most expressed recommendation for goggles (56.5%) and face shields (63.4%).
The product size category included 15.4% of recommendations for masks, 6.6% of recommendations for goggles, and 21.2% of recommendations for face shields. Across all PPE types, the most common recommendation was to produce PPE in different sizes to suit every face type.
Regarding functional properties, 16.3% of recommendations for mask production and 18.0% of the recommendations for goggles production fell within this category. The most common production recommendations were a high level of protection for masks (76.5%) and to not cause fogging for goggles (100.0%).
DISCUSSIONIn this descriptive qualitative study, the authors focused on the personal experiences of HCWs to determine problems they faced with PPE use in daily practice and obtain their recommendations for improving the quality of PPE.
Participants reported that surgical/medical masks are the most used PPE in terms of the average duration of PPE use, followed by N95 masks. In the online survey study conducted by Tabah et al14 with HCWs in ICUs, face shields, N95/FFP2 masks, goggles, FFP3 masks, and surgical/medical masks were the PPE types used most often on the face. It is not surprising that face shields were so commonly used in that study because of the ICU setting: a high number of medical procedures and care interventions that take place in the ICU include risk of contact with contagious secretions.14 In contrast, the present study included participants from all hospital units, leading to the surgical/medical mask being the most frequently used PPE.
International guidelines recommend that HCWs change masks every 4 hours.27 In the present study, participants reported changing masks a mean of every 2.72 ± 2.00 (medical/surgical masks) to 2.91 ± 4.11 (N95 masks) hours. However, they still experienced problems related to PPE use, most frequently reporting skin problems and wounds. Marks on contact areas were also noted to be a common problem for all PPE but are not considered to be a skin integrity problem.
In line with these problems, participants most often reported taking preventive measures regarding skin protection and care. They described applying moisturizer to contact areas when using a mask (54.8%) and applying a protective cover and barrier to contact areas when using goggles (25.8%) or a face shield (66.7%). In addition to skin protection measures, participants also mentioned increasing the frequency of mask replacement (58.3%), using ear saver straps to reduce the pressure exerted by PPE on the skin (25.0%), not using goggles (30.0%), and not using a face shield (22.7%). In this study, medical/surgical and N95 masks were disposable, but goggles and face shields were sterilized and reused.
In the multicenter cross-sectional survey study by Jiang et al,9 42.8% of participants developed facial skin injury due to PPE use: 30.0% developed PIs, 10.8% experienced moisture-associated skin damage, and 2.0% had skin tears. In the same study, 27.4% of the participants had two or more types of injuries, and 76.8% had injuries at two or more anatomic regions.9 Those authors determined that sweating and working with PPE for long hours were among the most important risk factors for skin injuries.9 In the descriptive study by Abiakam et al,13 88.0% of participants experienced skin injuries caused by PPE. These injuries primarily occurred on the chin (29.0%) and nasal bridge (27.0%), where the masks contacted skin the most.13 Further, HCWs in that study noted the importance of feeling safe (61.0%), breathing easily (37.0%), and feeling comfortable (26.0%) while wearing PPE.13 Although the present study differs in methodology and PPE-related injury rate, the findings are consistent with the literature regarding problems experienced by HCWs.
Silicone wound dress
Comments (0)