
Remember me

Thanks to the use of ultrasound equipment and the engagement of interprofessional teams,1 peripherally inserted central catheter (PICC)-related complications, such as thrombosis,2 infections, and occlusion, have been effectively controlled. However, Kang et al3 found that 4.6% of patients with cancer who have a PICC develop a skin allergy, compared with 3.4% experiencing occlusion and 1.9% developing symptomatic PICC-related thrombosis. Skin injury related to the PICC can occur by various means; for example, affixing the catheter at the puncture site with a dressing may induce tension, an alcohol disinfectant can irritate local skin, or the catheter could cause a medical device-related pressure injury (PI). Wang et al4 reported the incidence of PICC-related skin injury in patients with lung cancer to be as high as 31.5%. Incidences of PICC-related skin injury in the literature range from 24.8% to 31.5%.4–6 Skin injury, in turn, intensifies PICC-related infection, increasing the economic burden of patients and even possibly leading to an unplanned removal.
In 2021, the Infusion Nursing Association updated their guidelines to promote skin management at the catheter site and reduce skin injury.7 After removing the dressing, providers should then examine the area and confirm skin injury if they note erythema lasting longer than 30 minutes or compromised skin integrity due to dermatitis or mechanical skin injuries (eg, blisters or PI).7,8
Although many studies have investigated the risk factors of PICC-related skin injury, few have assessed the timing and characteristics of injury.5,6,10 Research indicates that as the duration of catheter retention increases, the incidence of PICC-related complications also increases, from 34.78% with 3 to 6 months’ duration to 55.56% at 9 to 12 months’ duration.9 Because the developmental trajectory and characteristics of skin injury during PICC placement remain unclear, medical personnel are limited in their ability to decide when to take appropriate interventions.
Study ObjectiveIn this study, the authors aimed to (1) determine the risk factors of skin injury in patients with a chest tumor and PICC and (2) map out the developmental trajectory and characteristics of skin injury during PICC retention.
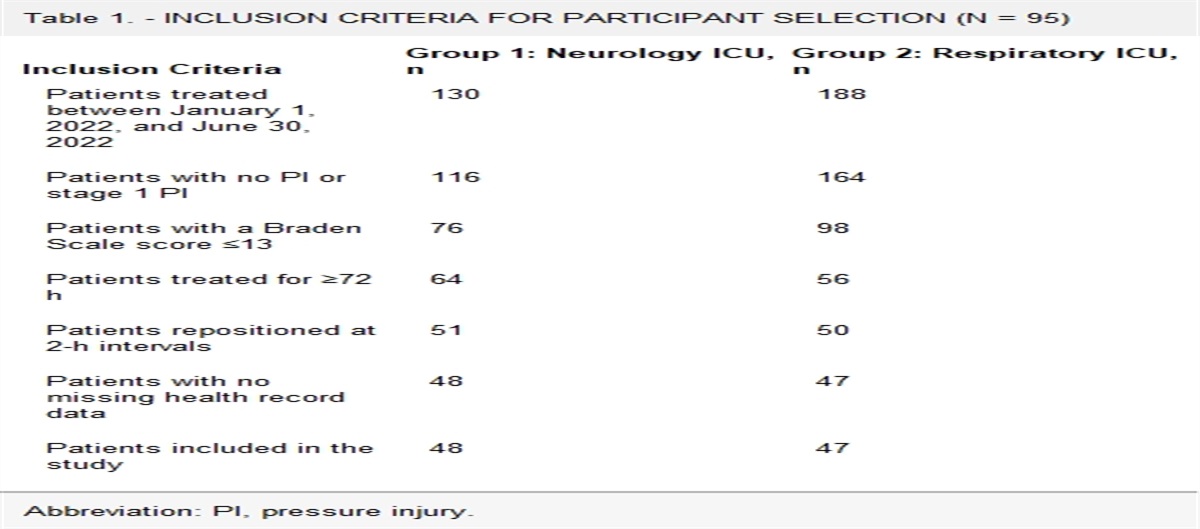
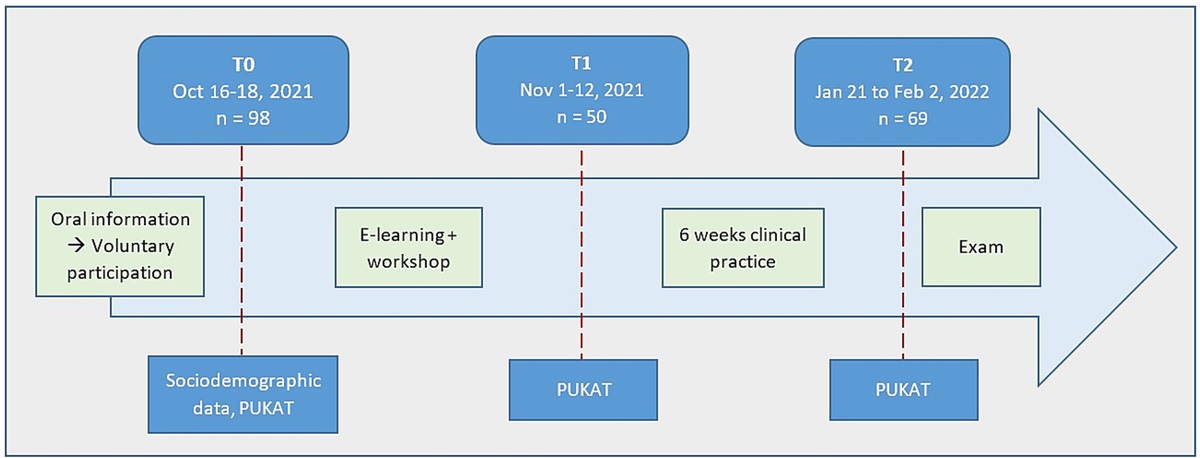
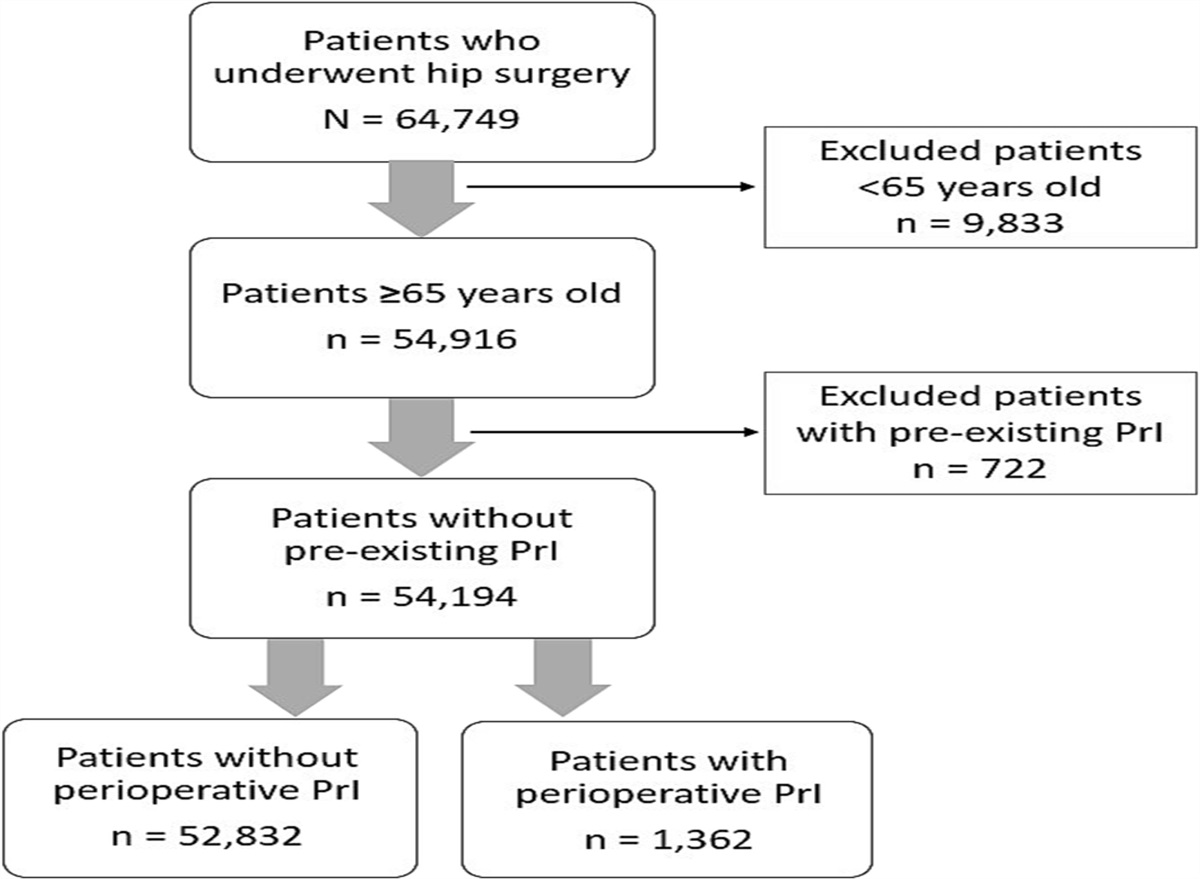
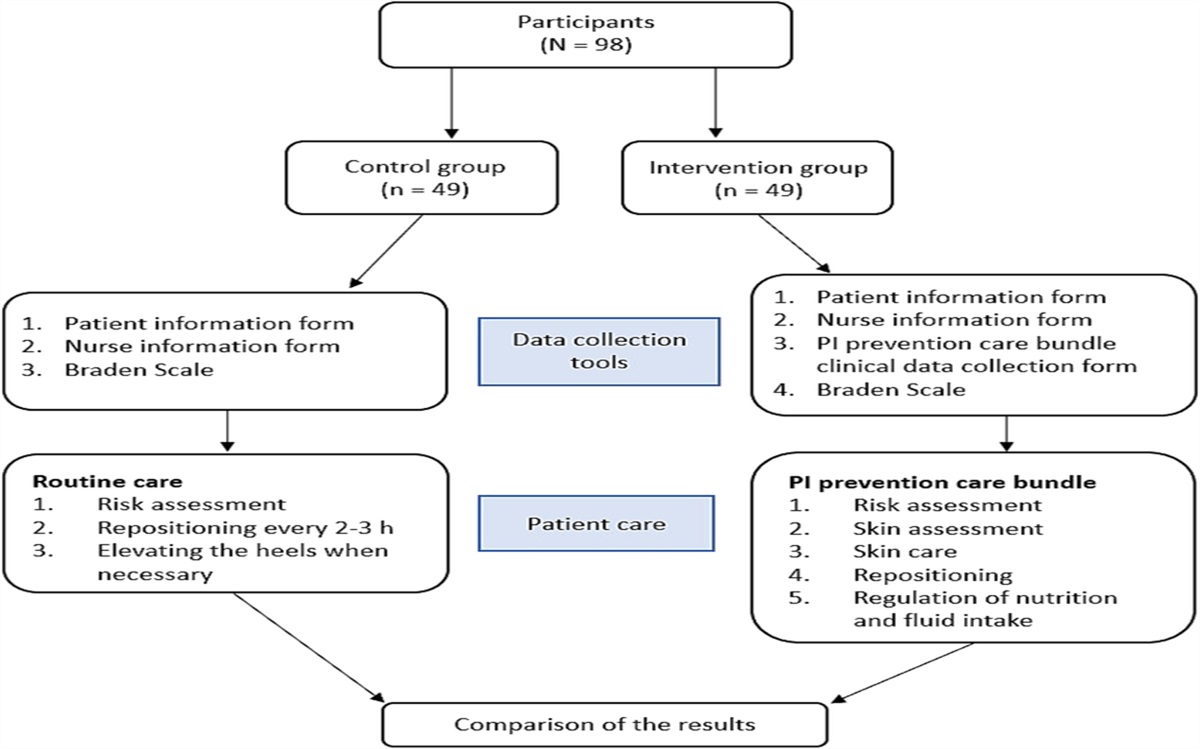
METHODSThis retrospective cohort study included 252 patients with a chest tumor who received PICC placement, maintenance, and removal in a tertiary hospital in Shanghai, China, between March 2018 and December 2021. Patients were included in the study if they were 18 years or older, the purpose of their PICC placement was to receive chemotherapy, they signed the informed consent form before PICC placement, and they received regular catheter maintenance and follow-ups. Patients were excluded if their removal information was missing or they had otherwise incomplete medical records. The protocol of this study was approved by the Hospital Ethics Committee (IS22069).
Physicians prescribed PICC placement on the basis of the patient’s chemotherapy cycles and medications. Then, trained nurses with PICC knowledge evaluated the patients’ surgical history, chemotherapy or radiation history, and recent coagulation indicators to determine if they were a suitable candidate for PICC placement.
PICC Placement and MaintenanceSenior infusion nurses who are well-trained and have relevant certifications perform all PICC placements in the outpatient treatment room. During PICC placements, every step follows the principle of sterility, and an ultrasound device is used to facilitate the success rate for one puncture. Only single-lumen power PICCs (Bard Access Systems) are available in the hospital. Typically, the basilic vein of the right arm is preferred if there are no medical contraindications. The ultrasound-guided puncture is combined with the Seldinger technique under local anesthesia to ensure a smooth placement. After PICC placement, a chest X-ray is conducted by a radiologist to identify the position of the catheter tip and determine whether the catheterization is successful. After successful catheter placement, patients receive a manual describing how to perform PICC maintenance. After the catheter is removed, the maintenance manual is recycled by the PICC department.
It is primarily outpatient PICC nurses who are in charge of PICC maintenance, which occurs once per week. The nurses use disposable PICC maintenance kits that include disinfectants (2% chlorhexidine gluconate and 75% alcohol) and transparent dressing (Tegaderm HP; 3M). All nurses have received PICC maintenance training and use correct maintenance techniques to avoid skin injury: The dressing is removed slowly at 0° or 180° from the horizontal angle; the disinfection area is larger in size than the dressing application; the disinfectant is dry; and the dressing is applied in a tension-free manner, with the interior of the dressing usually affixed first, and then the surrounding areas of the dressing affixed in sequence.
Data CollectionBased on a review of the literature and interviews with experts, the authors created a data collection form that included the following: patient’s personal information (eg, sex; age; coagulation indicators; history of diabetes, hypertension, smoking, alcohol use, disease, and chemotherapy drugs), catheterization information (eg, insertion date, catheterization vein, catheterization limb, removal time), and adverse outcomes (eg, skin injury). One author collected these data from the hospital’s electronic database and a second author verified the accuracy of the data. Patient names were removed to ensure patient privacy.
When conducting weekly catheter maintenance, PICC outpatient nurses recorded the date and checked for complications. Patients were determined to have skin injury if they had erythema, blistering, rash, or PI at the PICC site.
Statistical AnalysisThe researchers divided patients into two groups according to the presence of PICC-related skin injury and conducted univariate and multivariate logistic regression analyses. Data analysis was performed using SPSS 26.0 (IBM Corp). The data were counted by frequency and percentage (%), and a χ2 test or Fisher exact test was performed for categorical variables. Normally distributed data were expressed as mean and SD, and an independent-sample t test was performed; non-normally distributed data were represented by median and interquartile range (IQR), and a Mann-Whitney U test was used for comparison. P < .05 indicated statistical significance.
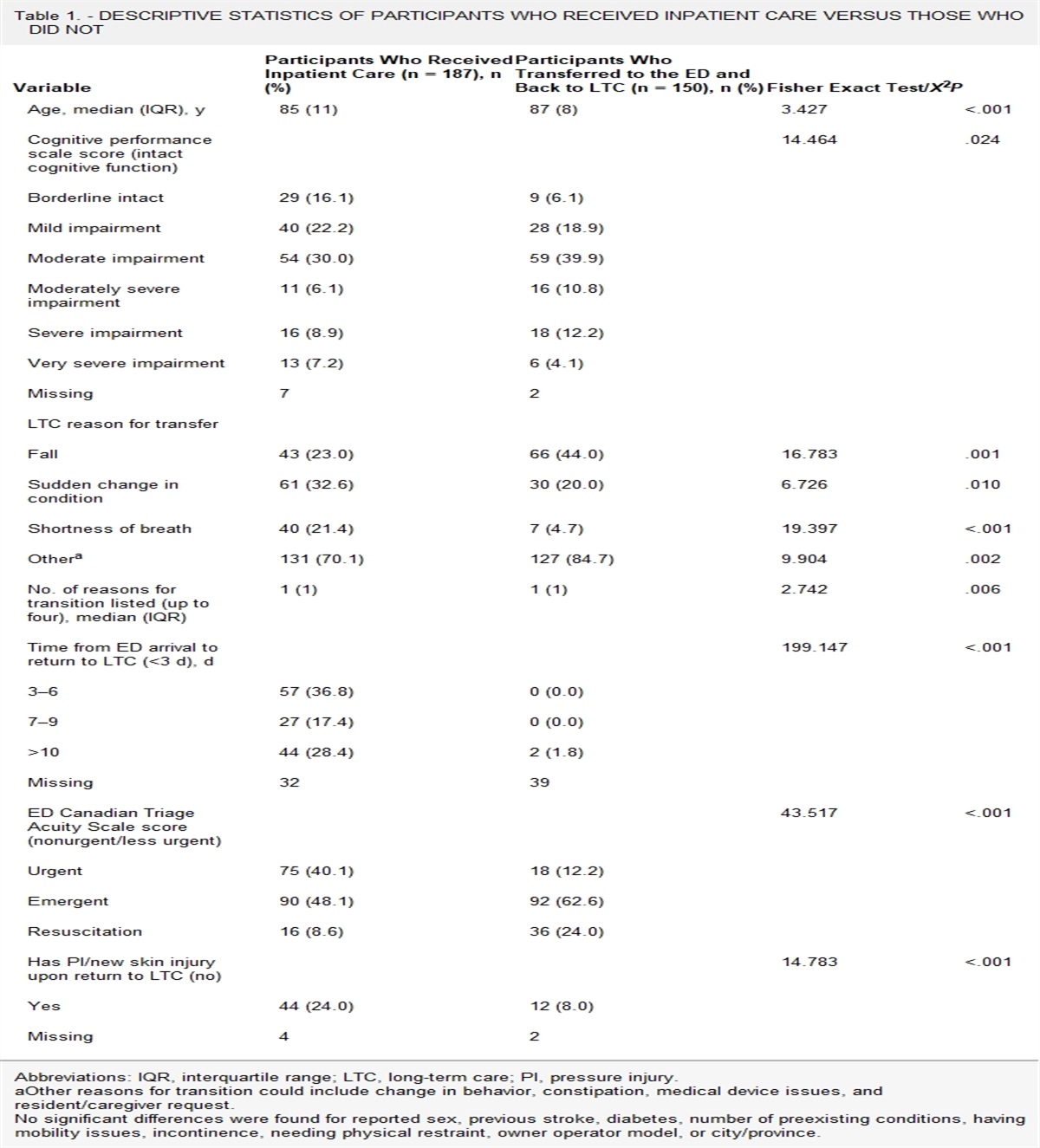
RESULTSThis study included 252 patients (188 men) with a total catheter retention duration of 29,390 days. Patients ranged in age from 32 to 85 years (mean, 63.51 [SD, 7.93] years), and the majority of them (n = 182) had lung cancer. Patient characteristics are shown in Table 1.
Table 1. - BASELINE PATIENT CHARACTERISTICS (N = 252) Variable Skin Injury, n (%) χ 2/Z/t P No Yes Disease type 7.561 .006 Lung cancer 98 (53.8) 84 (46.2) Esophageal cancer 51 (72.9) 19 (27.1) Received PICC maintenance at >1 hospital 0.248 .618 No 64 (61.0) 41 (39.0) Yes 85 (57.8) 62 (42.2) Radiotherapy 4.033 .045 No 10 (63.9) 57 (36.1) Yes 48 (51.1) 46 (48.9) Recombinant human endostatin injection 5.240 .022 No 135 (61.9) 83 (38.1) Yes 14 (41.2) 20 (58.8) Department 0.585 .444 Nonradiotherapy 81 (57.0) 61 (43.0) Radiotherapy 68 (61.8) 42 (38.2) Sex 0.404 .525 Female 40 (62.5) 24 (37.5) Male 109 (58.0) 79 (42.0) Catheterization limb 0.112 .738 Right 135 (59.5) 92 (40.5) Left 14 (56.0) 11 (44.0) Catheterization vein 2.271 .132 Basilic vein 111 (56.6) 85 (43.4) Brachial vein 38 (67.9) 18 (32.1) Catheter tip location 1.654 .198 T7-8 124 (61.1) 79 (38.9) Other 25 (51.0) 24 (49.0) Smoking 6.374 .012 No 123 (63.4) 71 (36.6) Yes 26 (44.8) 32 (55.2) Age, mean ± SD 64.31 ± 7.726 62.96 ± 8.063 −1.330 .185 Body mass index, kg/m2 2.179 .140 18.5-23.9 100 (56.2) 78 (43.8) Other 49 (66.2) 25 (33.8) Hypertension 1.756 .185 No 123 (61.2) 78 (38.8) Yes 26 (51.0) 25 (49.0) Diabetes 0.269 .604 No 132 (59.7) 89 (40.3) Yes 17 (54.8) 14 (45.2) Eosinophil count 2.102 .147 Normal 136 (60.7) 88 (39.3) Abnormal 13 (46.4) 15 (53.6) White blood cell count 3.664 .056 Normal 134 (61.5) 84 (38.5) Abnormal 15 (44.1) 19 (55.9) Surgical history within 1 y 1.499 .221 No 107 (56.9) 81 (43.1) Yes 42 (65.6) 22 (34.4) Allergy history 16.576 .000 No 148 (62.2) 90 (37.8) Yes 1 (7.1) 13 (92.9) Retention time, median (IQR), d 94 (49.5, 134.5) 114 (64, 169) −2.632 .008Abbreviations: IQR, interquartile range; PICC, peripherally inserted central catheter.
The incidence rate of skin injury was 40.8% (103/252), of which 36.9% (38/103) were mechanical skin injury (blisters or PIs), and 63.1% (65/103) were dermatitis. Of the patients who developed dermatitis, 86.5% (56/65) had mild or moderate dermatitis, and 13.5% (11/65) had severe dermatitis.
The mean duration of PICC retention was 116.63 ± 83.72 days, and the median duration was 99 days (IQR, 57.25–147.75 days). Skin injury occurred between 2 and 361 days after PICC placement. The average was 70.23 ± 64.90 days, and the median was 56.0 days (IQR, 20.75–99.25 days).
To understand the peak period of skin injury, the researchers divided the 103 patients who developed a skin injury into seven groups according to when the skin injury occurred (the first month, the second month, the third month, the fourth month, the fifth month, the sixth month, and the seventh month or later). By comparing how many patients developed a skin injury at each time point following PICC placement, the authors were able to track the trajectory of skin injury occurrence. Overall, skin injury occurrence was primarily concentrated within the first 3 months after PICC placement and gradually declined thereafter with increasing catheter duration (Figure 1).
 Figure 1.:
Figure 1.: TIME DISTRIBUTION OF SKIN INJURY OCCURRENCE AFTER CATHETER PLACEMENT
The authors also evaluated occurrence timing by the type of skin injury (Figure 2). Pressure injury development showed no clear trajectory trend and could occur at any time. The occurrence of PICC-related dermatitis was highest in the first 3 months after PICC placement and followed a downward trajectory thereafter, decreasing in occurrence with increasing catheter duration. Similarly, the trajectory of blister development also presented a falling trend as catheter duration increased; however, blistering was most likely to occur within 2 months of PICC placement.
 Figure 2.:
Figure 2.: TIME DISTRIBUTION OF DIFFERENT TYPES OF SKIN INJURIES AFTER CATHETER PLACEMENT
Factors Affecting PICC-Related Skin InjuryUnivariate analyses show that disease type, radiotherapy history, recombinant human endostatin use, smoking history, allergy history, and the duration of catheter retention all varied significantly between patients who developed skin injury and those who did not (Table 1). The authors then set these variables as independent variables for logistic regression analysis (Table 2). Of the variables evaluated in the logistic regression analysis, retention duration, recombinant human endostatin use, smoking history, and allergy history were all risk factors of PICC-related skin injury in patients with chest tumors (Table 3).
Table 2. - VARIABLE ASSIGNMENTS FOR LOGISTIC REGRESSION ANALYSIS Variable Assignment Disease Lung cancer = 0, others = 1 Smoking history No = 0, yes = 1 Allergy history No = 0, yes = 1 Radiotherapy No = 0, yes = 1 Use of recombinant human endostatin injection No = 0, yes = 1Abbreviation: PICC, peripherally inserted central catheter.
Of the 103 patients who developed skin injury, the catheter was prematurely removed in 25 (24.2%). Compared with patients who developed mechanical skin injuries (eg, blister or PI), patients with dermatitis were more likely to have the PICC removed prematurely, with an incidence of 35.4% (Table 4).
Table 4. - COMPLICATION TYPES, FREQUENCIES, AND PICC REMOVAL RATES Complication Type Total Frequency n/N (%) [per 1,000 Catheter Days] PICC Removed Due to Skin Injury, n/N (%) Skin injury 103/252 (40.8) [3.50] 25/103 (24.2) Mechanical skin injury 38/103 (36.9) 2/38 (5.3) Blister 20/103 (19.4) 0 Pressure injury 18/103 (17.5) 2/18 (11.1) Dermatitis 65/103 (63.1) 23/65 (35.4) Unplanned removal of PICC 44/252 (17.4) [1.50] 12/23 (52.2)Abbreviation: PICC, peripherally inserted central catheter.
The demand for PICCs in healthcare remains high because they offer advantages such as low rates of thrombosis or occlusion, convenience, and relatively low cost. Therefore, it is important to identify current catheter problems to improve patient safety and reduce unnecessary medical costs.
A PICC is always fixed by a transparent dressing; as a result, the skin around the PICC puncture site is exposed to a relatively closed and moist environment. During weekly maintenance, the dressing change and use of alcohol or other disinfectants can increase skin irritation. Further, PI is likely to occur when external pressure acts on the catheter for more than 30 minutes. Patients with PICC placement experience skin injury at an incidence of 19.7% to 31.5%.4,6 However, in the present study, the skin injury rate was 40.8%, with dermatitis accounting for 63.1% of cases (65/103) and mechanical skin damage accounting for the remaining 36.9% (38/103). This rate, which is higher than previous studies,5,9 may be due to several reasons. The average age of patients in this study was 63 years, and patients older than 50 years are at high risk for PICC-related skin injury.9 The force between the epidermis and dermis decreases with age, and skin is more easily torn by external forces. In addition, the majority of patients in the present study have lung cancer, and their treatment pattern could lead to a risk of skin injury.
In this study, patients who developed a skin injury were more likely to have an unplanned catheter removal, and the incidence of dermatitis from premature catheter removal was 35.4%. Preventing skin injury associated with PICC will also help prevent premature catheter removal. However, in clinics, skin injury is often seen as a minor problem, and PICC-related skin injury has been overlooked.12 Common treatments include topical application of ointment or keeping the dressing application away from the injury,11 but prevention strategies based on early risk assessment or evidence-based approaches are lacking.13
Previous studies have primarily focused on identifying the risk factors of skin injury with PICC placement and have rarely described at what point after catheterization patients are at highest risk. Mao et al14 found that PICC-related skin injury first occurred in patients after a mean of 33.00 ± 6.29 days. Tian et al5 only reported that the duration of catheter retention served as a protective factor for patients in terms of skin injury development.5
However, in the present study, the authors recorded and evaluated the timing of skin injury development following PICC placement both in general and by type of injury. The researchers counted the number of patients with skin injury on a monthly basis and determined that the occurrence trajectory showed a downward trend, with skin injury occurring most often within 3 months of catheter placement. Regarding the timing of skin injury occurrence by injury type, there was no obvious concentration trend for PIs, which could occur at any time. The occurrence of blisters decreased with increasing duration of catheter retention and was mainly concentrated at 2 months after catheter placement; the occurrence of dermatitis was mainly concentrated at 3 months after catheter placement and similarly decreased with increasing duration of catheter retention. Based on these results, the authors suggest that medical personnel should take preventive measures early after PICC placement to prevent skin injury.
In this study, allergy history, smoking history, recombinant human endostatin injection, and catheter retention duration were all risk factors for PICC-related skin injury in patients with chest tumors. Smoking causes blood vessels to atrophy, reduces blood flow, and leads to skin aging.15 Recombinant human endostatin injection is primarily used to treat non–small cell lung cancer, and allergic reaction is one of its adverse effects.16 As a result, patients with lung cancer who received recombinant human endostatin injection were more likely to develop skin injuries. The finding that patients with a history of allergies were more likely to develop PICC-related skin injury is consistent with the literature.4 These patients are sensitive to external stressors and more likely to develop allergic reactions to medical adhesives, sweat, or disinfectants and are more likely to have dermatitis. Moreover, patients with cancer are more prone to have internal dysfunction after receiving multiple cycles of chemotherapy, resulting in weakness and sweating,17 which increases skin irritation.18,19 Contrary to the study by Tian et al,5 the results of the present study indicate that catheter retention duration is a risk factor for skin injury. This difference in findings may be related to the diversity of study participants. During catheter maintenance, the removal of the transparent dressing will stretch the local skin, removing epidermal cells and weakening the skin barrier, and, ultimately, leading to local skin injury.8,20 Nurses should pay attention to the patient’s skin management during catheter retention to prevent skin injury.
In this study, the incidence of mechanical skin damage was 15.1%. When providing PICC maintenance, nurses should remove the transparent dressing slowly and horizontally and apply the dressing with the normal anatomic position of the limb to decrease skin tension and avoid mechanical skin injury.14 The incidence of PICC-related dermatitis was 25.8%. To help prevent dermatitis, nurses should select dressings with high permeability and low sensitivity according to the patient’s skin status, allergy history, and medication history. If local PICC-related dermatitis or PI develops, nurses should apply an antiallergic ointment, StatLock (Becton Dickinson), or gauze.
Although the authors found no correlation between patients receiving PICC maintenance services from multiple hospitals and skin injury development, differences in disinfectant types, dressing applications, and nurse maintenance techniques among different hospitals could lead to PICC-related skin injuries. With the establishment of PICC maintenance institutions in various regions, patients are able to choose a hospital according to their own needs. Therefore, hospitals should standardize PICC maintenance processes to supplement clinical practice and conduct relevant nurse training to ensure that patients receive the same nursing quality across institutions.
In addition, because patients may be the first to discover complications, nurses should educate patients about the causes and adverse consequences of skin injuries to leverage their risk awareness and treatment adherence. When the nurse performs catheter maintenance on patients, the patient should be educated individually according to their skin condition or skin injury type. To increase patient access to information, it would also be useful for hospitals to establish an online consultation platform for nurses to answer questions and educate patients online when issues arise.
LimitationsBecause this is a retrospective study, the researchers did not have access to factors such as the patient’s skin properties (eg, dry, moist), adhesive-related skin injury history, or self-management ability. However, all of these factors may impact skin injury prevention. Therefore, prospective, multicenter, large-sample cohort studies should be conducted to identify the targeted factors for PICC-related skin injury so that nurses can take timely measures.
CONCLUSIONSThe incidence of PICC-related skin injuries in patients with chest tumors is high, mainly concentrated in the first 3 months after PICC placement, and the occurrence trajectory shows a downward trend. Smoking history, allergy history, the use of recombinant human endostatin, and the duration of catheter retention are risk factors for PICC-related skin injury. By understanding the risk factors and characteristics of PICC-related skin injury, nurses can implement precise interventions to reduce the incidence of skin injury.
REFERENCES 1. Li J, Fan YY, Xin MZ, et al. A randomised, controlled trial comparing the long-term effects of peripherally inserted central catheter placement in chemotherapy patients using B-mode ultrasound with modified Seldinger technique versus blind puncture. Eur J Oncol Nurs 2014;(1):94–103. 2. Chen P, Wan G, Zhu B. Incidence and risk factors of symptomatic thrombosis related to peripherally inserted central catheter in patients with lung cancer. J Adv Nurs 2021;77(3):1284–92. 3. Kang J, Chen W, Sun W, et al. Peripherally inserted central catheter-related complications in cancer patients: a prospective study of over 50,000 catheter days. J Vasc Access 2017;18(2):153–7. 4. Wang Z, Wan G, Pan L, Wang Y. Multivariate analysis of medical adhesive-related skin injury in peripherally inserted central catheter implanted patients with lung cancer. Chin J Clin Nutr 2018;26(3):191–4. 5. Tian L, Yin X, Zhu Y, Zhang X, Zhang C. Analysis of factors causing skin damage in the application of peripherally inserted central catheter in cancer patients. J Oncol 2021:6628473. 6. Zhao H, He Y, Huang H, et al. Prevalence of medical adhesive-related skin injury at peripherally inserted central catheter insertion site in oncology patients. J Vasc Access 2018;19(1):23–7. 7. Gorski LA, Hadaway L, Hagle ME, et al. Infusion therapy standards of practice, 8th Edition. J Infus Nurs 2021;44(1):S1–224. 8. McNichol L, Lund C, Rosen T, Gray M. Medical adhesives and patient safety: state of the science: consensus statements for the assessment, prevention, and treatment of adhesive-related skin injuries. J Wound Ostomy Continence Nurs 2013;40(4):365–80. 9. Wang K, Zhou Y, Huang N, Lu Z, Zhang X. Peripherally inserted central catheter versus totally implanted venous port for delivering medium- to long-term chemotherapy: a cost-effectiveness analysis based on propensity score matching. J Vasc Access 2021:1129729821991360. 10. Zhao H, He Y, Wei Q, Ying Y. Medical adhesive-related skin injury prevalence at the peripherally inserted central catheter insertion site: a cross-sectional, multiple-center study. J Wound Ostomy Continence Nurs 2018;45(1):22–5. 11. Kleidon TM, Ullman AJ, Gibson V, et al. A pilot randomized controlled trial of novel dressing and securement techniques in 101 pediatric patients. J Vasc Interv Radiol 2017;28(11):1548–56. 12. Fumarola S, Allaway R, Callaghan R, et al. Overlooked and underestimated: medical adhesive-related skin injuries. J Wound Care 2020;29:S1–S24. 13. Ullman AJ, Kleidon TM, Turner K, et al. Skin complications associated with pediatric central venous access devices: prevalence, incidence, and risk. J Pediatr Oncol Nurs 2019;36(5):343–51. 14. Mao L, Wen S, Feng S. Application of biomechanical characteristics of the skin in PICC line maintenance in elderly cancer patients. J Nurs Sci 2020;35(17):49–51. 15. Wong QYA, Chew FT. Defining skin aging and its risk factors: a systematic review and meta-analysis. Sci Rep 2021;11(1):22075. 16. Zhang R, Wang ZY, Li YH, et al. Usefulness of dynamic contrast-enhanced magnetic resonance imaging for predicting treatment response to vinorelbine-cisplatin with or without recombinant human endostatin in bone metastasis of non-small cell lung cancer. Am J Cancer Res 2016;6(12):2890–900. 17. Zulkowski K. Understanding moisture-associated skin damage, medical adhesive-related skin injuries, and skin tears. Adv Skin Wound Care 2017;30(8):372–81. 18. Pires-Júnior JF, Chianca TCM, Borges EL, Azevedo C, Simino GPR. Medical adhesive-related skin injury in cancer patients: a prospective cohort study. Rev Lat Am Enfermagem 2021;29:3500. 19. Zhu W, Jia L, Chen G, et al. Relationships between the changes of skin temperature and radiation skin injury. Int J Hyperthermia 2019;36(1):1160–7. 20. Jenks M, Craig J, Green W, Hewitt N, Arber M, Sims A. Tegaderm CHG IV securement dressing for central venous and arterial catheter insertion sites: a NICE medical technology guidance. Appl Health Econ Health Policy 2016;14(2):135–49.
Comments (0)