
Remember me



Laser ablation profiles are the most important element of laser refractive surgery. In 1998, Munnerlyn and colleagues published their method of calculating the ablation profile based on the thin-lens formula.1 Their technique assumed that the eye was made of a single refractive element from which a thin lens was to be removed. This was mathematically convenient and successful and led to the popularization of the Munnerlyn formula. The ablation profile, however, led to excessive flattening of the central cornea, which caused an increase in spherical aberration (by 0.3 μm/D).
Two strategies were used to tackle this problem—the customized Q-value–based treatment and the wavefront-optimized treatment. The former aimed to create a prolate cornea after laser ablation. It was estimated that a Q-value between −0.45 and −0.47, which was higher than the preoperative Q-value, would result in zero spherical aberration.2 The wavefront-optimized strategy noted that the same amount of laser pulse energy resulted in less peripheral ablation than central ablation. The strategy increased peripheral energy to increase the amount of peripheral ablation.3 Mathematically, both strategies were very complex; however, at their core, the authors highlighted in their publications that their equation could be reduced to the thin-lens equation, and they assumed that the eye was composed of a single refractive element and all other aspects such as anterior chamber depth, lens profile, and axial lengths were the same for all eyes. Furthermore, the preoperative aberrations of the patients were not considered.
The next major advances were in wavefront-guided and topography-guided treatments.4,5 These still did not account for multiple refractive elements. Posterior to the cornea, all eyes were considered the same. The wavefront-guided treatment measured the wavefront aberrations and attempted to correct it; however, the applied ablation was not as effective as it was hoped. Its use was recommended for eyes with HOAs above 0.3 to 0.4 root mean square (RMS), where induced HOAs were lower than preoperative HOAs. However, 83% of eyes in the study had <0.3 RMS.4 The topography-guided treatment resulted in much improved outcomes, with 93% to 94% achieving 20/20 and 65% 20/16 or better and 34% 20/15 or better.5–7
The recurring theme in the ablation profiles mentioned above is the removal of a thin lens from the cornea of varying complexity to affect the focus of light. However, removal of a thin lens is not the goal of laser refractive surgery but the technique. Theoretically, the purpose of laser refractive surgery may be rephrased as the ablation of the cornea by such an amount as to change the angle of incidence of a ray of light at the cornea so that the rest of the eye may focus the light appropriately on to the fovea. To achieve this, the path of each individual ray of light after it crosses the anterior surface of the cornea must be known or modeled for each individual eye. This is attempted by ray-trace–based laser in situ keratomileusis (LASIK), which was introduced a decade ago.8,9 In its present form, an optical model of the eye is created based on the measured anterior and posterior corneal tomography, axial length, and anterior chamber depth. Using this optical model, or an “eyevatar,” the wavefront is calculated. Any difference between the measured eye wavefront and the eyevatar-calculated wavefront is adjusted at the anterior surface of the crystalline lens such that the wavefront of the eyevatar model approaches the measured whole-eye wavefront. Thus, the light path/wavefront is modeled from the front corneal surface to the fovea. The model's anterior tomography can then be virtually treated to determine the change in angle of incidence at the cornea, which achieves the best possible postoperative wavefront.
A single diagnostic device called InnovEyes Sitemap (Alcon Laboratories, Inc.) measures the data for the model: corneal tomography (Scheimpflug principle), biometry (partial coherence interferometry), and total eye wavefront (Hartmann-Shack). The proprietary software then creates a model and automatically presents the most appropriate ablation profile for treatment.
The potential advantage of this methodology is that the model accounts for multiple refractive elements which may or may not be aligned, namely the cornea and the crystalline lens surfaces. The model also individualizes the treatment such that 2 eyes may have the same spectacle refraction, but can have potentially different eyevatars and ablation profiles. In addition, the ray-trace treatment has been modulated to account for laser efficiency, corneal biomechanics, and healing after myopic LASIK surgery.
This study presents the largest cohort of eyes to have been treated using ray-tracing–based LASIK in a real-world private practice setting. Functional end points in addition to the effects of InnovEyes on postoperative higher-order aberrations (HOAs) are presented.
METHODSA retrospective chart review of consecutive adult patients undergoing ray-tracing–based LASIK surgery for myopia was undertaken at a single center in Sydney, Australia, between February 2022 and December 2022. This study was conducted in accordance with the National Statement on Ethical Conduct in Human Research (2007) and the CPMP/ICH Note of Guidance on Good Clinical Practice and followed the tenets of the Declaration of Helsinki. Consent to use deidentified data was obtained from the patients, and ethics approval was obtained from an external ethics committee.
Inclusion criteria included myopic adults 18 years and older who underwent bilateral ray-tracing–based LASIK surgery with no coexisting ocular conditions or previous ocular surgery. For refractive stability, patients were instructed not to wear rigid or toric contact lenses for ≥2 weeks or soft contact lens for 1 week before preoperative screening and surgery. Preoperatively patients were required to have had stable refraction for 12 months confirmed through previous prescriptions. All eyes were targeted for emmetropia. Preoperatively at screening visits, patients underwent subjective refraction, cyclopentolate 1%–based cycloplegic refraction, and dilated fundus examination and the ray-tracing–based LASIK device (InnovEyes Sitemap) captured measurements including biometry, wavefront refraction, whole-eye aberrometry, and tomography. The data were exported to the WaveNet server (Alcon Laboratories, Inc.) and excimer laser (EX500, Alcon Laboratories, Inc.). The ablation profile was generated using measurements in which the wavefront sphere and subjective sphere were within 0.5 diopters (D). No nomogram adjustments were made in this cohort. A customized ablation profile based on the ray-tracing technology was automatically generated for each eye.1
Bilateral sequential LASIK flaps were created at 110 microns using a Wavelight FS200 (Alcon Laboratories, Inc.) with a diameter of 9.2 mm. The excimer treatment, as mentioned above, was performed using a Wavelight EX500 (Alcon Laboratories, Inc.) with a treatment zone of 6.5 mm and using the ablation profile generated from the Innoveyes Sitemap data. All surgeries were performed by a single surgeon (C.B.). After the LASIK treatment, patients were reviewed at 1 day, 1 week, 1 month, and 3 months postoperatively. Wavefront measurement and subjective refraction were assessed at 3 months. All wavefront measurements were reported at the 5.5-mm pupil.
The outcomes examined include corrected and uncorrected visual acuities, using the Early Treatment Diabetic Retinopathy Study chart, and manifest refraction spherical equivalent (MRSE) at 3 months. The percentage of eyes with absolute MRSE within ±0.25, ±0.50, ±0.75, and ±1.00 D at month 3 is reported. The percentage of eyes that achieved a uncorrected distance visual acuity (UDVA) equal to or better than the preoperative corrected distance visual acuity (CDVA); percentage of eyes that achieved manifest refraction cylinder within ±0.25, ±0.50, and ±1.00 D at 3 months; as well as preoperative and postoperative mean HOAs including root mean square values of Zernike orders 3 to 6 (RMS 3 to 6) and total HOAs (RMS total HOAs) are also reported. Third-order aberrations include trefoil (Z3−3, Z33) and coma (Z3−1, Z31). Fourth-order aberrations include tetrafoil (Z4−4, Z44), secondary astigmatism (Z4−2, Z42), and spherical aberration (Z40). Fifth-order (Z5−5, Z55, Z5−3, Z53, Z5−1, Z51) and sixth-order (Z6−6, Z66, Z6−4, Z64, Z6−2, Z62, Z60) aberration composite values are reported. A paired t test was applied to the results where appropriate. A Bonferroni correction was applied to the P = .05 results for the 7 paired comparisons of wavefront data resulting in a Bonferroni-corrected P value threshold of 0.0071.
Patients were divided into 4 groups based on postoperative UDVA (20/10, 20/12.5, 20/16 and 20/20) and their pre and postoperative HoAs were compared.
RESULTSFour hundred eyes of 200 consecutive patients with myopia who underwent ray-trace–based LASIK were recruited in this study. All eyes underwent uncomplicated surgery. There were no cases of flap complications, infections, or diffuse lamellar keratitis. Patients were aged 30.87 ± 5.4 years on average; 58% were female with preoperative myopia from −8.25 to −0.25 D and mean CDVA of −0.12 logMAR. Baseline characteristics are summarized in Table 1 while baseline aberrations are summarized in Table 2. The total HOA preoperatively was 0.220 ± 0.073 μm (right eye 0.218 ± 0.072 μm, left eye 0.220 ± 0.076 μm).
Table 1. - Preoperative characteristics Parameter Ray-tracing–based LASIK Patients (eyes) 200 right and 200 left (400) Age (y), mean ± SD (range) 30.8 ± 5.4 (20, 48) Female, n (%) 116 (58) Male, n (%) 84 (42) Right eye Left eye Preop UDVA (logMAR), mean ± SD (range) 0.91 ± 0.38 (0.20, 1.64) 0.92 ± 0.37 (0.20, 1.64) Preop CDVA (logMAR), mean ± SD (range) −0.12 ± 0.06 (−0.20, 0.00) −0.12 ± 0.06 (−0.20, 0.00) Manifest refraction sphere (D), mean ± SD (range) −3.35 ± 1.71 (−8.05, −0.25) −3.5 ± 1.79 (−8.82, −0.25) Manifest refraction sphere category, n/N (%) 0 to ≤−1.0 D 10 (5) 16 (8) >−1.0 to ≤−2.0 D 40 (20) 29 (14.5) >−2.0 to ≤−3.0 D 43 (21.5) 43 (21.5) >−3.0 to ≤−4.0 D 45 (22.5) 47 (23.5) >−4.0 to ≤−5.0 D 27 (13.5) 21 (10.5) >−5.0 to ≤−6.0 D 24 (12) 25 (12.5) >−6.0 to ≤−7.0 D 12 (6) 17 (8.5) >−7.0 to ≤−8.0 D 3 (1.5) 2 (1) >−8.0 to ≤−9.0 D 1 (0.5) 0 (0) Manifest refraction cylinder (D), mean ± SD (range) −0.95 ± 0.82 (−4.4, 0.00) −0.99 ± 0.80 (−4.37, 0.00) Manifest refraction cylinder category, n/N (%) 0 to ≤−0.50 D 64 (32) 58 (29) >−0.50 to ≤−1.00 D 68 (34) 68 (34) >−1.00 to ≤−1.50 D 32 (16) 39 (19.5) >−1.50 to ≤−2.00 D 17 (8.5) 15 (7.5) >−2.00 to ≤−2.50 D 7 (3.5) 8 (4) >−2.50 to ≤−3.00 D 3 (1.5) 5 (2.5) >−3.00 to ≤−3.50 D 5 (2.5) 2 (1) >−3.50 to ≤−4.00 D 1 (0.5) 4 (2) >−4.00 to ≤−4.50 D 3 (1.5) 1 (0.5) MRSE (D), mean ± SD (range) −3.84 ± 1.63 (−8.34, −0.84) −3.98 ± 1.75 (−8.25, −0.5)MRSE = manifest refraction spherical equivalent
*Statistically significant
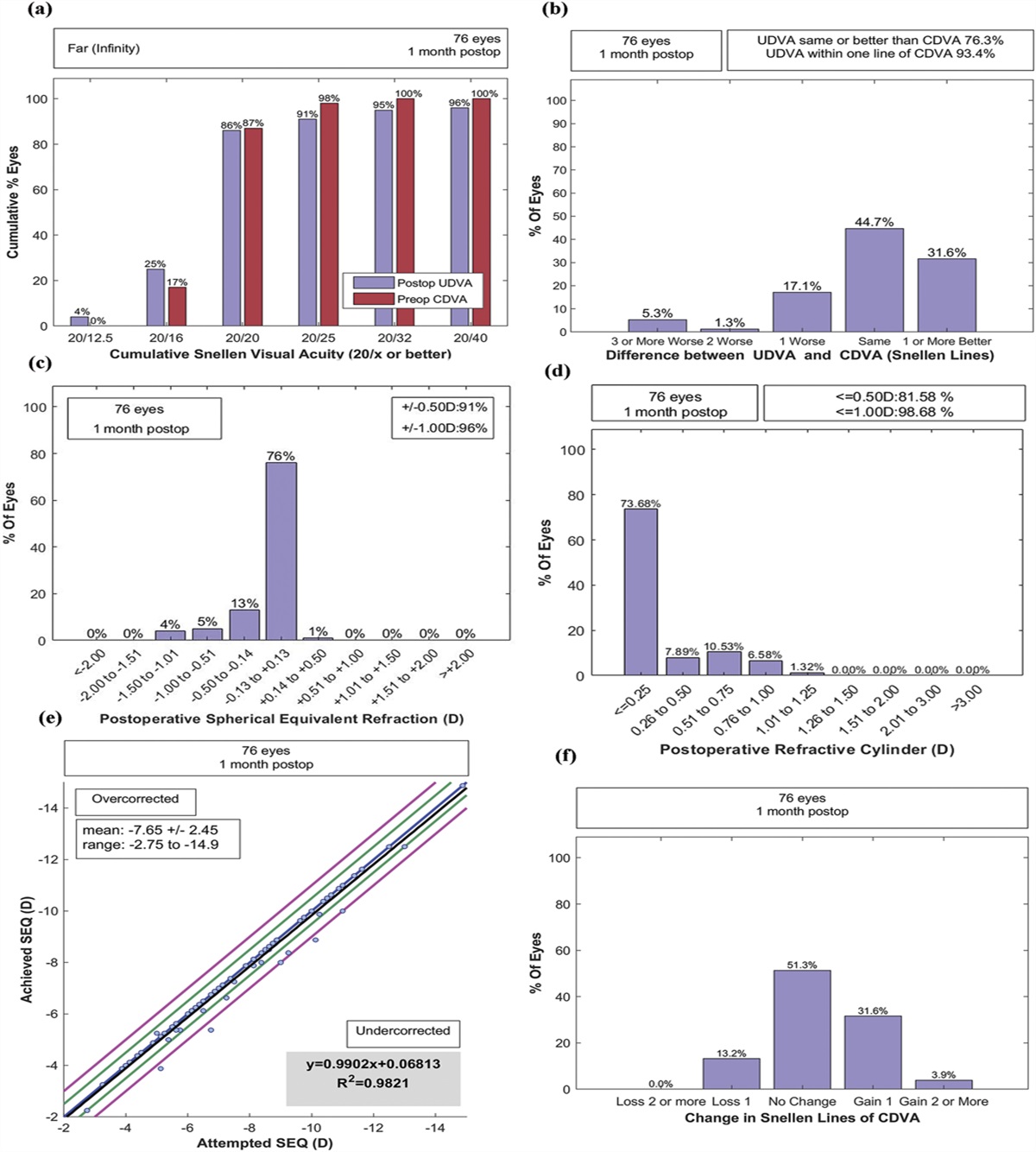
The standardized graphs in Figure 1 demonstrate the visual and refractive outcomes of our cohort at 3 months. The mean postoperative sphere, cylinder, and spherical equivalents at 3 months for 400 eyes were 0.12 ± 0.28 D (right eye 0.10 ± 0.26 D, left eye 0.14 ± 0.30 D), −0.24 ± 0.20 D (right eye −0.23 ± 0.20 D, left eye −0.24 ± 0.20 D), and 0.00 ± 0.28 D (right eye −0.01 ± 0.25 D, 0.02 ± 0.28 D), respectively. The UDVA at 3 months was −0.14 ± 0.06 logMAR (right eye −0.15 ± 0.08 logMAR, left eye −0.14 ± 0.08 logMAR). UDVA of 20/20 or better was achieved in 100% of eyes, and CDVA (right eye −0.17 ± 0.06 logMAR, left eye −0.17 ± 0.06 logMAR) was 20/20 or better in 100% of eyes (Figure 1, A). UDVA of 20/10 was achieved in 8% eyes (right eye 8% and left eye 9%) postoperatively, compared with 0% of CDVA preoperatively. Approximately half of the eyes (50.5% (right eye 54% and left eye 47%)) achieved 20/12.5 or better UDVA, with 89.3% (right eye 90% and left eye 89%) of eyes achieving 20/16 or better.
 Figure 1.:
Figure 1.: Refractive and visual outcomes at month 3. A: Cumulative postoperative UDVA compared with preoperative CDVA. B: Line difference between postoperative UDVA and preoperative CDVA. C: Change in lines between preoperative and postoperative CDVA. D: Attempted vs achieved spherical equivalent refraction. E: Spherical equivalent refraction accuracy. F: SEQ (MRSE) stability at screening, week 1, month 1, and month 3. G: Refractive astigmatism. H: Target-induced astigmatism vs surgically induced astigmatism. I: Refractive astigmatism angle of error. MRSE = manifest refraction spherical equivalent; SEQ = spherical equivalent refraction UDVA; uncorrected distance visual acuity; VA = visual acuity
Comparison of postoperative UDVA with preoperative CDVA showed that 84% eyes (right eye 85% and left eye 83%) had equivalent or better postoperative UDVA, with 45.0% eyes (right eye 47% and left eye 43%) having no change and 39% eyes (right eye 38% and left eye 40%) gaining 1 or more lines of improvement in visual acuity (Figure 1, B). Mean logMAR CDVA at all postoperative visits was better than preoperative mean CDVA. Analysis of lines of change from preoperative CDVA to month 3 CDVA showed that 46.5% eyes (right eye 46% and left eye 46.5%) had no change, 40.3% eyes (right eye 41% and left eye 39.4%) gained 1 line, and 8.0% eyes (right eye 7% and left eye 9.6%) gained 2 lines of visual acuity (Figure 1, C). None of the eyes lost 2 or more lines of CDVA compared with preoperative CDVA.
The absolute MRSE at 3 months was within ±0.25, ±0.50, or ±1.00 D in 56.5% (right eye 59% and left eye 54%), 96.3% (right eye 97% and left eye 96%), and 100% (right eye 100% and left eye 99.5%) of eyes, respectively (Figure 1, E). There was a very strong correlation between attempted and achieved SE refraction (both eyes R2 = 0.98, not shown; right eye R2 = 0.98; left eye R2 = 0.98, Figure 1, D). MRSE had a high level of stability postoperatively, with a mean change of 0.06 D in each eye from week 1 to month 1 and 0.02 D from month 1 to month 3 (Figure 1, F). Astigmatic correction was successful, with the percentages of eyes achieving manifest refraction cylinder within ±0.25 D, ±0.50 D, and ±1.00 D being 82% (right eye 84%; left eye 80%), 96% (right eye 97%; left eye 96%), and 100% (right eye 100%; left eye 100%), respectively. The relationships between target-induced astigmatism and surgically induced astigmatism and the refractive astigmatism angle of error are shown in Figure 1, H and I, respectively. There was an overcorrection of astigmatism with a slope of 1.12 (R2 = 0.91; right eye 1.13, R2 = 0.97; left eye 1.11, R2 = 0.96; Figure 1, H). Two eyes had a decrease in CDVA of 2 lines at week 1/month 1, which resolved to be within 1 line of baseline by month 3. No eyes had an increase in absolute refractive astigmatism >1 D of cylinder.
The preoperative and 3-month postoperative aberration values for Zernike orders 3 to 6, spherical aberration, coma, and total higher-order aberrations at 5.5-mm diameter are reported in Table 2. A clinically significant change in aberration is defined as a change of 0.1 μm.10 All the aberrations showed a statistically significant increase (P < .001; Bonferroni-corrected threshold P < .0071, paired t test) after the ray-trace laser, except the fourth-order aberration, which includes spherical aberration. The preoperative mean total HOAs (right eye 0.218 ± 0.072 μm; left eye 0.220 ± 0.076 μm) when compared with postoperative total HOAs (right eye 0.281 ± 0.116 μm; left eye 0.277 ± 0.112 μm) increased slightly (right eye 0.063 ± 0.133 μm; left eye 0.057 ± 0.125 μm), but was not clinically significant. The preoperative spherical aberration (right eye 0.064 ± 0.088 μm; left eye 0.066 ± 0.086 μm) decreased slightly (right eye 0.017 ± 0.097 μm; left eye 0.015 ± 0.09 μm), which was statistically significant (right eye −0.047 ± 0.095 μm; P < .001; left eye −0.051 ± 0.091 μm; P < .001). Each Zernike order from order 3 to order 6 (except order 4) and coma showed a nonclinically but statistically significant increase of less than 0.1 μm.
Subgroup analysis of aberrations of eyes based on postoperative visual acuity was undertaken (Figure 2). The 4 groups overall resembled each other preoperatively and postoperatively. Although there is a gradual trend towards decreasing HOA rms values from 20/20 to 20/10 vision, it was not statistically significant.
 Figure 2.:
Figure 2.: Total HOA as a function of postoperative unaided vision. Patients are grouped into 6/3, 6/3.8, 6/4.8, and 6/6 uncorrected distance vision, and the mean total higher-order aberrations (RMS) preoperatively (light gray bar) and at 3 months postoperatively (dark gray bar) are charted. Error bars represent standard error of the mean.
DISCUSSIONThis study presents the largest retrospective chart review to date of ray-trace–based LASIK undertaken in clinical practice. Ray-trace–based LASIK was initially presented a decade ago with a view to create an individualized treatment based on an individualized eye model.9 It was developed as a concept to overcome the limitations of traditional treatments which did not account for the light path beyond the anterior corneal surface.1–6 In the ray-trace model, simulation showed that using traditional wavefront-guided profile, spherical aberration doubled compared with the ray-tracing–based LASIK. This individualized treatment was expected to yield better results.
The ray-trace treatment concept was first tested in a clinical trial of high myopes by Schumacher et al. who treated 127 eyes with a mean manifest refraction of −5.92 D ± 1.72. UDVA of 20/20 or better was achieved in 83.8% of eyes, UDVA 20/16 or better in 61.3% of eyes, and 87.4% had an MRSE within ±0.50 D.11 The study compared different modalities of LASIK (wavefront-optimized, topography-guided, and wavefront-guided) published in the literature and demonstrated favorable visual outcomes. One of the authors reported their 1-year follow-up data for a portion of the study, with 100% of eyes achieving UDVA 20/20 and 9.5% achieving 20/12.5 or better.12 Kanellopoulos using the current version of the ray-tracing algorithm in a smaller cohort of eyes (50 eyes of 25 patients) with preoperative myopia ≤−9 D and astigmatism ≤−6 D also achieved similar results.13 At 6 months, 100% of eyes achieved UDVA of 20/20 or better and more than 40% achieved 20/16 vision or better.
In this study, UDVA of 20/20 was achieved in 100%, 20/16 or better in 89% to 90%, 20/12.5 or better in 50.5% (right eye 54%, left eye 47%), and 20/10 in 8% eyes (right eye 8%, left eye 9%). The results of this study compare favorably with wavefront-optimized treatments, which achieved 20/20 or better in 93%, 20/16 or better in 64%, and 20/12.5 or better in 25% of eyes. The topography-guided treatment with the same excimer laser at 3 months achieved 20/20 in 93% of eyes, 20/16 or better in 69%, 20/12.5 or better in 32%, and 20/10 or better in 8%.5 This study screened patients who were ideal candidates, for whom the topographic astigmatism matched the manifest astigmatism. The use of analytic engines to modify topography-guided treatment, which made its use more widespread, have been reported to achieve 20/20 in 100% of eyes, 20/16 or better in 89%, and 20/12.5 or better in 28% of eyes at 3 months.6,7 Not unexpectedly, the ray-trace–based LASIK performed better; however, a head-to-head study would be needed. The gain of 1 or more lines of postoperative UDVA compared with preoperative CDVA (right eye 39%, left eye 40%) was comparable with topography guided treatment (42%).7 In addition, 48.3% of eyes had improved CDVA of 1 or 2 lines of visual acuity compared with preoperative CDVA. This compared well with outcomes of topography guided treatment (46%).7 At 3 months, 96% of eyes were within ±0.5 D of target MRSE with UDVA of −0.14 logMAR compared with a preoperative value of 0.92 logMAR. No eyes lost 2 or more lines in this study population.
The favorable results in this study could be attributed to a single device (Innoveyes Sitemap) which was used to measure the eye. All calculations were performed automatically and integrated, reducing the need for manual treatment planning and potential for measurement error from using a variety of equipment. The current treatment profile also incorporated compensation for excimer and ablation-related efficiency, corneal biomechanics, and wound healing response in its planning. This and the lower preoperative myopia (MRSE −3.39 ± 1.58 D) likely explain the better outcomes of this study compared with previous ray-trace studies.11
The attempted SEQ and achieved SEQ were almost linearly distributed with slopes of 1.0319 in the right eye and 1.0397 in the left eye and a high R2 value of 0.975 (right eye and left eye). However, Figure 1, D and E indicates a potential overcorrection of 0.25 D above −5 D. This needs to be confirmed with a larger cohort of eyes with myopia above −5 D. The astigmatism also demonstrates an overcorrection. Although 96% of eyes are within 0.5 D, the slope in Figure 1, H suggests an 11% (left eye) to 13% (right eye) overcorrection, which would need confirmation with an in-depth analysis of both low and high astigmatism to determine the cause and the offset that would be required to bring all eyes within 0.5 D. This study includes both eyes of patients to reflect everyday clinical practice. The statistical analysis was performed for each eye separately.
In this study, at 5.5-mm pupil diameter, the total HOAs increased from 0.218 ± 0.072 μm (right eye) and 0.220 ± 0.076 μm (left eye) preoperatively to 0.281 ± 0.116 μm (right eye) and 0.277 ± 0.112 μm (left eye) postoperatively. Aberration measurements can be influenced by a variety of factors, and variations of less than 0.1 µm are not considered clinically significant.10 Kanellopoulos also reported a small increase in total HOAs from 0.25 µm to 0.35 µm (at 4 mm diameter).13 In the present study, the smaller increase in HOAs at 5.5-mm diameter could account for the eyes achieving excellent vision. There was a statistically significant increase in all orders of aberrations, except the fourth order. The increase, however, was less than 0.1 µm. The fourth-order aberration, which included spherical aberration, was not significantly different after ray-trace–based LASIK (P = .055). The spherical aberration was noted to decrease from 0.064 ± 0.088 μm to 0.017 ± 0.097 μm in the right eye and from 0.066 ± 0.086 μm to 0.015 ± 0.098 μm in the left eye, as predicted in the theoretical model. This is despite 21% of the treated cohort being >−5 D sphere, a cohort in which a traditional laser ablation profile would be expected to increase the spherical aberration. Traditional ablation profiles are associated with an increase in total HOAs and spherical aberrations by as much as 2 to 17 times.14–19 The ray-trace–based LASIK performed much better compared with these earlier reports. It is important to note that comparison with previous studies is limited by pupil diameter; however, it is clear from the above discussion that wavefront-based treatment need not be limited to patients with greater than 0.3 to 0.4 μm HOAs.4 A further in-depth analysis is needed to examine the effect of laser ablation on individual HOA components.
It is important to note that in this study, a small cohort of eyes (8%) achieved 20/10 vision. Outcomes of 20/10 require excellent preoperative measurements, uncomplicated surgery, and a laser ablation profile that induces minimal HOAs. Postoperative total HOAs were analyzed in groups based on postoperative UDVA. Although there was no significant difference between HOAs within different postoperative UDVA of 20/10, 20/12.5, 20/16, and 20/20 groups, there was a gradually declining trend from 0.27 µm to 0.3 µm. In summary, although there does not seem to be a clinically significant increase in HOAs, these findings need to be examined in greater detail with further analysis of individual components of the wavefront and variability of wavefront measurement.
The current Innoveyes model contains assumptions including axial symmetry of refractive elements, refractive indices of the cornea, and the contribution of the posterior lens surface based on the Navaro eye model.20 It can still be affected by dry eyes and measurement device-related errors. Further analysis of astigmatic measurement and treatment would help improve the outcomes of this technology. A more detailed analysis is needed to examine the relationship between preoperative refraction and postoperative aberration. It would be of interest to determine the factors that lead to 2-line gain in vision or in 20/10 vision. This study reports 3 months’ data, which were stable; a longer term follow-up would aid in determining stability of refraction and the presence of long-term remodeling.
Ray-tracing–based LASIK in clinical practice was found to be safe and effective for myopic correction both with and without astigmatism. Approximately half of the eyes achieved UDVA of 20/12.5 or better and 8% achieved 20/10. The procedure resulted in a small statistically significant increase in HoA, which was not clinically significant, and a statistically significant reduction in spherical aberration. The use of a ray-tracing–based customized ablation profile based on a single measurement device holds promise in achieving better outcomes.WHAT WAS KNOWN Ray-trace–based LASIK is known to achieve stable and excellent 20/20 UDVA in 100% of high myopes. The outcomes are known to be stable.
WHAT THIS PAPER ADDS This large cohort shows successful outcomes in everyday clinic practice with half the eyes attaining a vision of 20/12.5. There was no clinically significant increase in HOAs. The spherical aberration decreased postoperatively. REFERENCES 1. Munnerlyn CR, Koons SJ, Marshall J. Photorefractive keratectomy: a technique for laser refractive surgery. J Cataract Refract Surg. 1988;14:46–52 2. Manns F, Ho A, Parel JM, Culbertson W. Ablation profiles for wavefront-guided correction of myopia and primary spherical aberration. J Cataract Refract Surg. 2002;28:766–774 3. Mrochen M, Donitzky C, Wullner C, Loffler J. Wavefront-optimized ablation profiles: theoretical background. J Cataract Refract Surg. 2004;30:775–785 4. Stonecipher KG, Kezirian GM. Wavefront-optimized versus wavefront-guided LASIK for myopic astigmatism with the ALLEGRETTO WAVE: three-month results of a prospective FDA trial. J Refract Surg. 2008;24:S424–S430 5. Stulting RD, Fant BS; T-CAT Study Group TCS, Bond W, Chotiner B, Durrie D, Gordon M, Milauskas A, Moore C, Slade S, Randleman JB, Stonecipher K. Results of topography-guided laser in situ keratomileusis custom ablation treatment with a refractive excimer laser. J Cataract Refract Surg. 2016;42:11–18 6. Lobanoff M, Stonecipher K, Tooma T, Wexler S, Potvin R. Clinical outcomes after topography-guided LASIK: comparing results based on a new topography analysis algorithm with those based on manifest refraction. J Cataract Refract Surg. 2020;46:814–819 7. Stulting RD, Lobanoff M, Mann PM II, Wexler S, Stonecipher K, Potvin R. Clinical and refractive outcomes after topography-guided refractive surgery planned using Phorcides surgery planning software. J Cataract Refract Surg. 2022;48:1010–1015 8. Mrochen MC, Cummings A, Maus M, Seiler T. Optical ray tracing-guided LASIK for moderate to high myopic astigmatism. Invest Ophthalmol Vis Sci 2011;52:5755 9. Mrochen M, Bueeler M, Donitzky C, Seiler T. Optical ray tracing for the calculation of optimized corneal ablation profiles in refractive treatment planning. J Refract Surg 2008;24:S446–S451 10. Xu Z, Hua Y, Qiu W, Li G, Wu Q. Precision and agreement of higher order aberrations measured with ray tracing and Hartmann-Shack aberrometers. BMC Ophthalmol 2018;18:18 11. Schumacher S, Seiler T, Cummings A, Maus M, Mrochen M. Optical ray tracing-guided laser in situ keratomileusis for moderate to high myopic astigmatism. J Cataract Refract Surg 2012;38:28–34 12. Cummings A, Kelly G. Optical ray tracing-guided myopic laser in situ keratomileusis: 1-year clinical outcomes. Clin Ophthalmol 2013;7:1181–1191 13. Kanellopoulos AJ. Initial outcomes with customized myopic LASIK, guided by automated ray tracing optimization: a novel technique. Clin Ophthalmol 2020;14:3955–3963 14. Marcos S Aberrations and visual performance following standard laser vision correction. J Refract Surg 2001;17:S596–S601 15. Seiler T, Kaemmerer M, Mierdel P, Krinke HE. Ocular optical aberrations after photorefractive keratectomy for myopia and myopic astigmatism. Arch Ophthalmol 2000;118:17–21 16. Taskov G, Taskov T. Higher order aberrations (HOA) changes after femto-LASIK in topography and wavefront guided treatments. Folia Med (Plovdiv) 2020;62:331–337 17. Marcos S, Barbero S, Llorente L, Merayo-Lloves J. Optical response to LASIK surgery for myopia from total and corneal aberration measurements. Invest Ophthalmol Vis Sci 2001;42:3349–3356 18. Mrochen M, Kaemmerer M, Mierdel P, Seiler T. Increased higher-order optical aberrations after laser refractive surgery: a problem of subclinical decentration. J Cataract Refract Surg 2001;27:362–369 19. Padmanabhan P, Basuthkar SS, Joseph R. Ocular aberrations after wavefront optimized LASIK for myopia. Indian J Ophthalmol 2010;58:307-312 20. Navarro R, Santamaría J, Bescós J. Accommodation-dependent model of the human eye with aspherics. J Opt Soc Am A 1985;2:1273–1281
Comments (0)