
Remember me
Colorectal cancer (CRC) is a significant public health concern globally, with it being the third most commonly diagnosed cancer in both men and women and a leading cause of cancer-related deaths worldwide (1). Screening colonoscopies have contributed to a decrease in mortality by 51% and incidence rates of CRC by 32% in the past 50 years by allowing early detection and removal of precancerous adenomas (2,3). Most polyps found during colonoscopies, exceeding 90%, are small or diminutive in size (≤5 mm). These smaller polyps are considered unlikely to harbor advanced neoplasia or invasive cancer (4,5). Consequently, the leave-in-situ and resect-and-discard approaches for managing diminutive colorectal polyps have been established in response to this finding. The resect-and-discard paradigm was formalized in 2011 and proposed by the American Society for Gastrointestinal Endoscopy Preservation and Incorporation of Valuable Endoscopic Innovation (6).
The American Society for Gastrointestinal Endoscopy Preservation and Incorporation of Valuable Endoscopic Innovation document delineates 2 performance thresholds that must be met by endoscopic technologies before their implementation in clinical practice for the assessment of diminutive colorectal polyps. The first threshold is that for a technology to guide the decision to leave in situ rectosigmoid hyperplastic polyps ≤5 mm, the negative predictive value (NPV) for adenomatous histology should be equal to or exceed 90% (PIVI-1). The second threshold is that endoscopic technology used to determine the histology of colorectal polyps 5 mm or smaller, when combined with histopathologic assessment of larger polyps, should provide an agreement of 90% or higher in assigning postpolypectomy surveillance intervals when compared with decisions made based on pathology assessment of all detected polyps to allow for resection and discarding without pathologic assessment (PIVI-2) (7).
The resect-and-discard and leave-in-situ paradigms rely on the ability of endoscopists to accurately predict polyp histology with high confidence using endoscopic classification schemes, such as the Kudo classification, Narrow-Band Imaging International Colorectal Endoscopic classification, and blue-light imaging modality (8-10). Unfortunately, many endoscopists, especially the less experienced ones, are unable to do so using the current standard colonoscopy equipment. A survey sent to 330 gastroenterologists nationwide showed that only 41.9% of gastroenterologists agreed that an endoscopist can reliably classify polyps as adenomatous or hyperplastic on endoscopic appearance alone and only 40.3% of gastroenterologists felt comfortable using a “diagnose-and-leave” approach for a polyp they believed was hyperplastic (11). Therefore, the current standard of care is to remove all polyps and to submit them for histopathological evaluation.
Computer-aided diagnosis (CADx) powered by artificial intelligence has been gaining attention as a potential method to improve optical diagnosis standardization and accuracy (12,13). The aim of this article was to review whether artificial intelligence as a new technology will improve the performance and confidence of endoscopists to eventually implement leave-in-situ and resect-and-discard strategies in the clinical setting.
The implementation of resect-and-discard and leave-in-situ strategies is important mainly for cost-saving reason, which can be substantial because it decreases submitting specimens to pathology. The expense of pathological analysis for diminutive polyps has a detrimental impact on the cost-effectiveness of colonoscopy. Simulation Markov modeling has demonstrated that using a resect-and-discard strategy for diminutive polyps can lead to significant cost savings of $25 per person screened, resulting in annual savings of $33 million for the US population. Adding a leave-in-situ strategy, with an estimated cost savings of more than $1 billion per year, would also avoid unnecessary polypectomies and reduce albeit low potential adverse events while improving efficiency in assigning postprocedure surveillance intervals (14,15). Moreover, it is noteworthy that the current processing of pathology specimens was found to have a high environmental impact (16).
Implementation of resect-and-discard and leave-in-situ strategies has been hindered by a lack of financial incentives for endoscopists, perceived medical-legal risks (because it may be difficult to determine the cause of an interval cancer if one were to arise, and endoscopists may face liability), and local rules for tissue handling (17). The leave-in-situ strategy may cause more concern than the resect-and-discard strategy because patients may question the accuracy of polyp characterization and some endoscopists may worry about increased work and litigation risks. Pathologists may be concerned about disruptive imaging technologies affecting the scope of their work (6).
The initial focus of artificial intelligence (AI) in colonoscopy practice has been on the automated detection of polyps (computer-aided detection), which can help reduce the risk of missed polyps during colonoscopy, which will subsequently improve the adenoma detection rate (ADR), thereby decreasing the incidence of interval cancer (18,19). A systematic review and meta-analysis by Barua et al have shown that the use of AI-based polyp detection systems (computer-aided detection) during colonoscopy has been shown to increase adenoma and polyp detection rates and mean numbers of adenomas and polyps detected per colonoscopy. The ADR with AI was 29.6% compared with 19.3% without AI, indicating a clinically significant increase of 10.3 percentage points (20). This was similarly demonstrated by another systematic review and meta-analysis by Hassan et al, which showed an increase in ADR by 44% and adenoma per colonoscopy by 70% (21). This improvement may have implications for future colorectal cancer prevention.
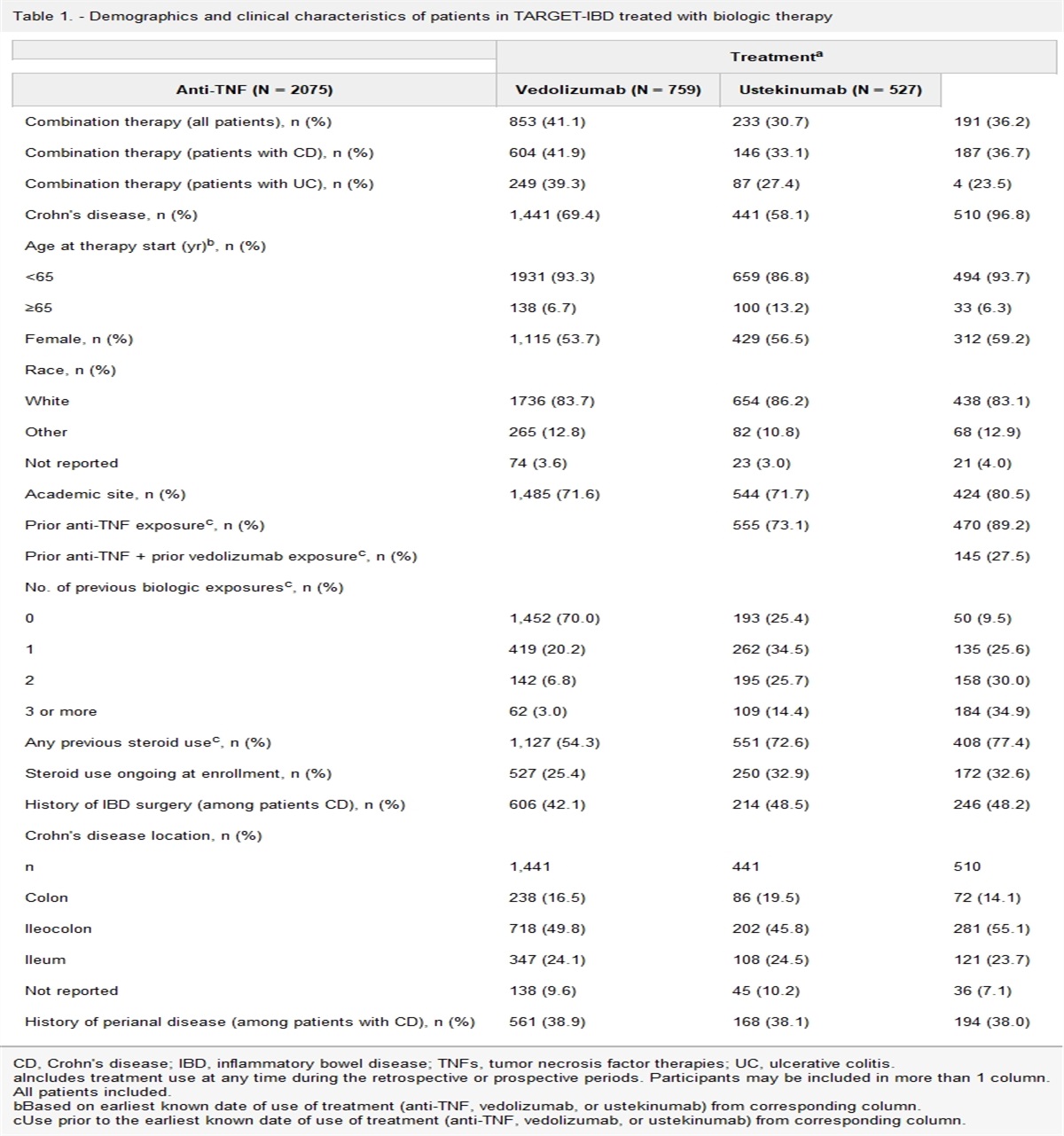
Computer-aided diagnosis (CADx) characterization has the potential to predict histology in vivo by classifying disease patterns in real time after adequate supervised training (18). AI models can accurately differentiate between conventional adenomas and hyperplastic polyps in diminutive colorectal polyps when used on unaltered colon polyp video sequences. The overall accuracy of the model was 94%, with a sensitivity of 98% and a specificity of 83%. The positive predictive value was 90%, and the negative predictive value was 97% (22). The use of CADx has the potential to enhance the confidence of endoscopists. This is especially important for the leave-in-situ strategy because its validity was not clinically confirmed before the introduction of AI. This lack of validation in the pre-AI era led to uncertainty regarding the accuracy of diagnoses and the potential occurrence of false-negative results (23). Several studies have been conducted in real time to evaluate the performance of CADx in optical biopsy for colorectal polyps (Table 1).
Table 1. - Real-time CADx studies–NPV for DRSP (PIVI-1) and postpolypectomy surveillance interval agreement (PIV-2) of CADx compared with endoscopists Study name Year Patients included Total polyps NPV CADx PIVI-1 NPV endoscopist PIVI-1 PIVI-2 CADx ESGE-USMSTF PIVI-2 endoscopist ESGE-USMSTF Barau 2022 518 892 92.8% 91.5% Not available Not available Hassan 2022 162 291 97.6% 97.6% 95.6%–95.9% 96.5%–95.9% Li 2023 274 188 80.6% 83.3% 97.5%–70.8% 97.1%–71.9% Rondotti 2022 389 596 86.7% (CADx alone)AI, artificial intelligence; CADx, computer-aided diagnosis; DRSP, diminutive rectosigmoid polyps; ESGE, European Society of Gastrointestinal Endoscopy; NPV, negative predictive value; PIVI, Preservation and Incorporation of Valuable Endoscopic Innovation; USMSTF, US Multi-Society Task Force.
In a study conducted by Rondonotti et al, a computer-aided diagnosis system called CAD-EYE was used to assist in making optical diagnoses. The study was conducted in 4 open-access endoscopy centers in Italy where they dichotomized the participating endoscopist as experts and nonexperts in optical diagnosis. Experts are endoscopists who have followed a dedicated training program, performed optical diagnosis on regular basis according to the European Society of Gastrointestinal Endoscopy (ESGE) curriculum, and underwent periodic auditing and monitoring (24,25).
The AI-assisted high-confidence optical diagnosis was successful in 92.3% of cases. The NPV of AI-assisted optical diagnosis for diminutive rectosigmoid polyps (PIVI-1) was 91.0% (95% confidence interval [CI], 87.1–93.9), meeting the threshold for the leave-in-situ strategy. However, the NPV for AI alone was suboptimal at 86.7% (95% CI, 82.3%–90.1%). It is possible that the introduction of a second-generation CAD-EYE system in the future could improve this. The PIVI-2 threshold was met with 97.4% (95% CI, 95.7%–98.9%) and 92.6% (95% CI, 90.0%–95.2%) of patients, according to ESGE and US Multi-Society Task Force guidelines, respectively, indicating an agreement rate of ≥90% for postpolypectomy intervals in the resect-and-discard strategy. The accuracy of AI-assisted optical diagnosis was notably lower for nonexperts (82.3%; 95% CI, 76.4%–87.3%) compared with that for experts (91.9%; 95% CI, 88.5%–94.5%). However, over time, the performance of nonexperts gradually approached that of experts (25).
Hassan et al in a prospective, single-arm study conducted in one open-access endoscopy center in Italy showed that the CADx diagnosis was feasible in 291 of 295 cases (98.6%), with a high NPV of 97.6% for ≤5 mm rectosigmoid lesions. The study found that a real-time CADx system exceeded the 90% NPV for adenomatous histology required for the leave-in-situ strategy, potentially reducing polypectomies and related costs by 44.4% (23).
Regarding the resect-and-discard strategy, CADx accuracy was 77.9%, which was due to a lower specificity of 65.9%. Based on the gold standard of histology, the postpolypectomy surveillance interval was accurately determined in 155 of 162 cases (with an adjusted agreement of 95.6%; 95% CI, 90.8%–98.0%) following the ESGE recommendations. Similarly, following the US Multi-Society Task Force guidelines, it was accurately assessed in 149 of 162 cases (with an adjusted agreement of 95.9%; 95% CI, 89.8%–98.4%). This could lead to a reduction in pathology requirement to 83% of the identified lesions in the study with more than 95% agreement with histology-based postpolypectomy surveillance according to both American and European guidelines. The authors demonstrated favorable interactions between humans and the machine because the CADx diagnosis in white light was validated by the endoscopist in blue light with high confidence in most of the instances. This led to an AI-assisted endoscopist high-confidence NPV of 97.6%. In addition, high-confidence diagnoses were heightened compared with previous literature reports (78.2% vs 92.2%), thereby verifying the positive impact of AI-supported optical diagnosis on the confidence of endoscopists. Overall, the study demonstrates the potential of AI-assisted optical diagnosis in reducing costs and increasing efficiency in the management of colorectal polyps (23).
In a multicenter study by Barua in 2022 using Endobrain, the study focused on comparing sensitivity instead of NPV to assess the safety and efficacy of “leave-in-situ” because high sensitivity means a low false-negative rate. Using conventional visual inspection, the sensitivity, specificity, positive predictive value, and NPV of small rectosigmoid polyps diagnosis was 88.4% (95% CI, 84.3%–91.5%), 83.1% (95% CI, 79.2%–86.4%), 78.9% (95% CI, 74.3%–82.9%), and 91.5% (95% CI, 88.5%–93.8%), respectively, in contrast to 90.4% (95% CI, 86.8%–93.1%), 85.9% (95% CI, 82.3%–88.8%), 82.0% (95% CI, 77.6%–85.6%), and 92.8% (95% CI, 90.1%–94.9%), respectively, using CADx. However, the percentage of polyp evaluations with high confidence was 74.2% (95% CI, 70.9%–77.3%) using standard visual inspection as opposed to 92.6% (95% CI, 90.6%–94.3%) using CADx. AI did not significantly increase the sensitivity; however, it enhanced the specificity and practitioner's confidence in optical diagnosis. Approximately 92.6% of polyps were characterized into neoplastic or non-neoplastic with high confidence with CADx compared with only 74.2% with the standard method. The increase in confidence implies that more polyps can be left in situ, which will contribute to cost reduction. CADx met the NPV PIVI criteria more than 90%, which fulfill the criteria of the leave-in-situ strategy. However, the authors concluded that they are not able to draw any firm conclusions regarding the identification and extraction of small rectosigmoid polyps using the colonoscopy system they deployed (26).
In the most recent prospective multicenter study in 4 large tertiary referral centers by Li et al using CAD-EYE for diminutive sigmoid-rectal polyps, CADx exhibited an NPV of 80.6% (95% CI 73.1%–86.7%) while endoscopists achieved an NPV of 83.3% (95% CI 75.9%–89.3%). Both CADx and endoscopists fell short of meeting the PIVI-1 threshold of 90% for the NPV. When CADx and endoscopists reached an agreement, resulting in concordance, the NPV increased to 85.3% (95% CI 78.0%–90.9%). However, this level of performance does not meet the requirements for adopting a leave-in-situ approach. For the resect-and-discard strategy, when adhering to the recommendations of the US Multi-Society Task Force, neither CADx nor the endoscopists were able to reach the PIVI-2 threshold of 90% agreement. There was a 70.8% (95% CI 65.0%–76.1%) agreement between CADx and final histology vs 71.9% (95% CI 66.1%–77.1%) for endoscopists. However, when using the recommendations from the ESGE, both CADx and endoscopists surpassed the PIVI-2 threshold of 90% agreement, 97.5% (95% CI 94.8%–99.0%) with CADx and for endoscopists 97.1% (95% CI 94.3%–98.7%). The study has showed that endoscopists were superior to CADx in the overall diagnostic accuracy and sensitivity for neoplastic polyps; however, CADx had higher specificity. There was an increase in diagnostic accuracy when there was concordance between CADx and endoscopists. CADx has the potential to enhance the performance of endoscopists by serving as a second reader and aiding in the accurate optical diagnosis of polyps (27).
The clinical studies so far on CADx have showed mixed results regarding CADx and PIVI end points. CADx as a standalone technology did not outperform the endoscopists; however, it did not diminish the performance of endoscopists as per the 4 real-world studies discussed earlier. Rondonotti showed that CADx can add to the learning effect of diminutive rectosigmoid polyps, and Barua demonstrated that it can increase the high confidence read, which can have a role in improving nonexpert endoscopists who have between 1 and 5 years of colonoscopy experience or having independently performed between 200 and 1,000 procedures. Despite these results, there is still a concern of potential deskilling if endoscopists excessively depend on technology and neglect to rely on their clinical skills and experience (28).
One potential impact on the accuracy of CADx is the challenges in pathology for diagnosing diminutive polyps less than or equal to 3 mm. Ponugoli et al provided evidence that pathologic evaluation of polyps ≤3 mm in size, detected and removed by colonoscopy, is not the definitive diagnostic measure when the endoscopic interpretation is of a conventional adenoma with high confidence, yet the pathologic interpretation reports normal tissue. In the study, 644 lesions ≤3 mm were identified as high-confidence adenomas by a single expert endoscopist, and 15.4% of those lesions were classified as normal by pathology. In the same study, 2 impartial optical evaluation experts independently reviewed high-quality lesion images and reached a consensus with the endoscopic diagnosis in 93.9% (P = 0.15) and 100% (P = 0.51) of cases, respectively (29).
The authors suggest this discrepancy arises because of a higher true fragmentation rate than what is reported in pathology findings. This is potentially because while some tissue fragments during removal, only a single piece may be retrieved. An additional explanation offered relates to the processing method used. If the sectioning through minute polyps fails, this could result in a misdiagnosis, causing an adenoma to be mistaken for a normal tissue. During the process, a pathology specimen is fixed without orientation and embedded in paraffin. Thin slices (typically 4 μm in width) are then cut from one end of the paraffin block until the slices reach the tissue. This initial cutting or “facing” process may eliminate some or all the polyps, contributing to the diagnostic discrepancy (29).
A similar conclusion was reached by Sahidi et al. The authors included 644 colorectal lesions ≤3 mm with a high-confidence optical diagnosis of adenoma. Of these lesions, 458 (71.1%) had a matching pathological diagnosis while 186 (28.9%) showed discrepancies between endoscopic and pathological diagnoses. The introduction of real-time AI clinical decision support solutions (CDSS) showed promising results. When used, the CDSS agreed with the endoscopic diagnosis for 577 lesions (89.6%). In cases of discordant diagnoses between endoscopy and pathology, the CDSS aligned with the endoscopic diagnosis in 168 lesions (90.3%). Notably, the CDSS also concurred with the endoscopic diagnosis in 90 cases (90.9%) where pathology determined them as normal mucosae. These findings highlight the potential of AI in resolving conflicting diagnoses between endoscopists and pathologists in the future for polyps less than 3 mm in size (30).
Further investigations to assess the generalizability of these results should be conducted to validate and investigate the root causes of these disparities between endoscopy and pathology findings. Some limitations to the study by Ponugoli are that the authors did not subject the polyps not diagnosed as adenomas by pathology to review by another pathologist and the specimens were not recut for confirmation. It is also important to recognize that the endoscopists and reviewers involved in the study demonstrated expertise in predicting polyp histology endoscopically. The generalizability of the results may be uncertain because the proportion of lesions deemed high confidence but found to be normal or hyperplastic on pathology could differ for endoscopists with less experience (29).
In summary, despite the positive results, we cannot draw firm conclusions regarding the efficacy of the system in leave-in-situ or resect-and-discard strategies. Although AI alone may not currently be sufficient to replace human endoscopists in optical diagnosis, it seems to be a valuable tool for assisting endoscopists and potentially improving diagnostic accuracy and confidence of endoscopists. The role of CADx as a second reader, rather than a standalone diagnostic tool, seems more beneficial. It is also evident that CADx performance can be influenced by factors such as the system used, level of expertise of the endoscopist, and agreement between the AI system and endoscopist.
Several other potential applications for AI in the future include the ability to assess the quality of bowel preparation, measure lesion size, describe the morphology of lesions, identify features associated with invasive cancer, guide therapeutic procedures in real time, and automatically generate reports. These applications have the potential to improve the accuracy and efficiency of colonoscopy, leading to better patient outcomes (31). For instance, the ENDOANGEL system can evaluate colon cleansing in real time. It was trained using static images and colonoscopy videos and managed to achieve an accuracy rate between 93.3% and 89.4% for bowel preparation assessment, which surpasses the performance of endoscopists (32).
Kwak et al developed a new technique using the bifurcation-to-bifurcation (BtoB) distance–measuring method and applied it to endoscopic images. It was highly accurate and reliable in measuring the size of colon polyp (concordance correlation coefficients, 0.961; CI 0.926–0.979), outperforming the visual estimation and open biopsy forceps methods (33). Ichimasa developed an AI model to predict lymph node metastasis in patients with T1 CRC, which resulted in reduction of unnecessary surgeries after endoscopic resection of T1 CRC (34).
The integration of AI into clinical practices presents a set of unique challenges. This includes ethical dilemmas, technical feasibility issues, implementation hurdles, and regulatory matters.
Trust in AI analyses by medical professionals and regulatory authorities is a fundamental factor in the widespread adoption of AI platforms. Therefore, research should aim to foster complete transparency in the development and validation of AI models to alleviate any concerns about their public deployment. Unfortunately, the training process for AI is often nontransparent. The development of an effective model calls for large and varied data sets, encapsulating both normal and anomalous colonoscopies. Ideally, these data sets should be gathered from multiple centers and should comprise patients of varied ethnicities, ages, sexes, and health conditions.
It is essential to avoid the “black box” issue, which refers to AI models that lack clarity or explanation of how their algorithms function or produce predictions (35,36). To avoid “black box,” a pertinent academic branch within AI, known as “Explainable AI”, has emerged over the recent years. This branch is centered around the need for transparency in clinical decision support systems and providing clear insights into the decision-making process of AI systems (35,36).
There also exist legal implications. As AI begins to influence clinical decision-making, the question of liability arises in case of a medical error. If an AI model's conclusion was wrong, who should be held accountable?
Real-time decision-making is frequently required in endoscopic procedures. Therefore, AI models should be equipped to make accurate predictions in real time. Achieving an optimal balance between precision and speed is key for the practical application of AI systems. This implementation will require supplementary training of endoscopists and nursing staff for effective usage.
Another hurdle is financial disincentives, for example, physicians who own shares in pathology laboratories or the ones who are reimbursed per polypectomy might oppose the implication of CADx because it can result in less submission of specimen to pathology.
Another obstacle to widespread adoption of AI in clinical practice is the issue of reimbursement. It is imperative to perform comprehensive and high-quality cost-effectiveness analyses of these AI devices in various health care systems with diverse reimbursement policies before integrating them into routine clinical practice. To tackle this obstacle, the development of multifunctional AI systems capable of performing multiple tasks with a single device holds promise (37).
More research might be needed to improve the performance of CADx systems, possibly by merging CADx with other technologies such as AI capable of evaluating mucosal surface, polyp size, and resection completeness or by refining the AI algorithms as discussed earlier.
In the future, medical professionals will need specialized training to navigate ethical issues unique to the use of AI in health care and to better understand the interpretation of AI outputs. They might have to learn how to identify biased and under-represented data sets. At the very least, they will need to critically assess the suggestions provided by AI-based tools, rather than accepting them without question.
CONFLICTS OF INTERESTGuarantor of the article: Maysaa El Zoghbi, MD, MSc.
Specific author contributions: All the authors have equally planned the flow of the review article. All the authors equally collected the data. M.E.Z. and S.G. drafted the manuscript.
Financial support: None to report.
Potential competing interests: M.E.Z. and J.C.A. have no conflict of interest to disclose. S.A.G. is a consultant for Olympus, Medtronic, Iterative Scopes, Microtech, Cook, and Fujiflim. A.R. and C.H. are consultants for Fujifilm, Olympus, and Medtronic; research activity for NEC and Odin. A.S. is a consultant for Iterative Health, Freenome Inc, Motus GI, and UnviversalDX.
REFERENCES 1. Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018;68(6):394–424. 2. Winawer SJ, Zauber AG, Ho MN, et al. Prevention of colorectal cancer by colonoscopic polypectomy. N Engl J Med 1993;329(27):1977–81. 3. Burke C, Kaul V, Pohl H. Polyp resection and removal procedures: Insights from the 2017 digestive disease week. Gastroenterol Hepatol 2017;13(19 Suppl 2):1–24. 4. Hassan C, Pickhardt PJ, Kim DH, et al. Systematic review: Distribution of advanced neoplasia according to polyp size at screening colonoscopy. Aliment Pharmacol Ther 2010;31(2):210–7. 5. Ponugoti PL, Cummings OW, Rex DK. Risk of cancer in small and diminutive colorectal polyps. Dig Liver Dis 2017;49(1):34–7. 6. Abu Dayyeh BK, Thosani N, Konda V, et al. ASGE Technology Committee systematic review and meta-analysis assessing the ASGE PIVI thresholds for adopting real-time endoscopic assessment of the histology of diminutive colorectal polyps. Gastrointest Endosc 2015;81(3):502.e1–502.e16. 7. Rex DK, Kahi C, O'Brien M, et al. The American society for gastrointestinal endoscopy PIVI (preservation and incorporation of valuable endoscopic innovations) on real-time endoscopic assessment of the histology of diminutive colorectal polyps. Gastrointest Endosc 2011;73(3):419–22. 8. Repici A, Ciscato C, Correale L, et al. Narrow-band imaging international colorectal endoscopic classification to predict polyp histology: REDEFINE study (with videos). Gastrointest Endosc 2016;84(3):479–86.e3. 9. Kudo S, Hirota S, Nakajima T, et al. Colorectal tumours and pit pattern. J Clin Pathol 1994;47(10):880–5. 10. Hayashi N, Tanaka S, Hewett DG, et al. Endoscopic prediction of deep submucosal invasive carcinoma: Validation of the narrow-band imaging international colorectal endoscopic (NICE) classification. Gastrointest Endosc 2013;78(4):625–32. 11. Wadhwa V, Alagappan M, Gonzalez A, et al. Physician sentiment toward artificial intelligence (AI) in colonoscopic practice: A survey of US gastroenterologists. Endosc Int Open 2020;08(10):E1379–E1384. 12. Lahiff C, East JE. Endoscopic approach to polyp recognition. Frontline Gastroenterol 2017;8(2):98–103. 13. Mori Y, Kudo SE, Berzin TM, et al. Computer-aided diagnosis for colonoscopy. Endoscopy 2017;49(08):813–9. 14. Hassan C, Pickhardt PJ, Rex DK. A resect and discard strategy would improve cost-effectiveness of colorectal cancer. screening. Clin Gastroenterol Hepatol 2010;8(10):865.e3–9.e3. 15. Rex DK. Reducing costs of colon polyp management. Lancet Oncol 2009;10(12):1135–6. 16. Gordon IO, Sherman JD, Leapman M, et al. Life cycle greenhouse gas emissions of gastrointestinal biopsies in a surgical pathology laboratory. Am J Clin Pathol 2021;156(4):540–9. 17. Rex DK. Can we do resect and discard with artificial intelligence assisted colon polyp “optical biopsy?” Tech Innov Gastrointest Endosc 2020;22(2):52–5. 18. Mori Y, Kudo S-E, Misawa M, et al. Real-time use of artificial intelligence in identification of diminutive polyps during colonoscopy: A prospective study. Ann Intern Med 2018;169(6):357–66. 19. Kaminski MF, Regula J, Kraszewska E, et al. Quality indicators for colonoscopy and the risk of interval cancer. N Engl J Med 2010;362(19):1795–803. 20. Barua I, Vinsard DG, Jodal HC, et al. Artificial intelligence for polyp detection during colonoscopy: A systematic review and meta-analysis. Endoscopy 2021;53(03):277–84. 21. Hassan C, Spadaccini M, Iannone A, et al. Performance of artificial intelligence in colonoscopy for adenoma and polyp detection: A systematic review and meta-analysis. Gastrointest Endosc 2021;93(1):77–85. e6. 22. Byrne MF, Chapados N, Soudan F, et al. Real-time differentiation of adenomatous and hyperplastic diminutive colorectal polyps during analysis of unaltered videos of standard colonoscopy using a deep learning model. Gut 2019;68(1):94–100. 23. Hassan C, Balsamo G, Lorenzetti R, et al. Artificial intelligence allows leaving-in-situ colorectal polyps. Clin Gastroenterol Hepatol 2022;20(11):2505–13.e4. 24. Bisschops R, East JE, Hassan C, et al. Advanced imaging for detection and differentiation of colorectal neoplasia: European society of gastrointestinal endoscopy (ESGE) guideline-update 2019. Endoscopy 2019;51(12):1155–79. 25. Rondonotti E, Hassan C, Tamanini G, et al. Artificial intelligence-assisted optical diagnosis for the resect and-discard strategy in clinical practice: The artificial intelligence BLI characterization (ABC) study. Endoscopy 2023;55(01):14–22. 26. Barua I, Wieszczy P, Kudo S, et al. Real-time artificial intelligence–based optical diagnosis of neoplastic polyps during colonoscopy. NEJM Evid 2022;1(6). 27. Li JW, Wu CCH, Lee JWJ, et al. Real-world validation of a computer-aided diagnosis system for prediction of polyp histology in colonoscopy: A prospective multicenter study. Am J Gastroenterol 2023;118(8):1353–64. 28. Troya J, Fitting D, Brand M, et al. The influence of computer-aided polyp detection systems on reaction time for polyp detection and eye gaze. Endoscopy 2022;54(10):1009–14. 29. Ponugoti P, Rastogi A, Kaltenbach T, et al. Disagreement between high confidence endoscopic adenoma prediction and histopathological diagnosis in colonic lesions ≤3 mm in size. Endoscopy 2019;51(03):221–6. 30. Shahidi N, Rex DK, Kaltenbach T, et al. Use of endoscopic impression, artificial intelligence, and pathologist interpretation to resolve discrepancies between endoscopy and pathology analyses of diminutive colorectal polyps. Gastroenterology 2020;158(3):783–5.e1. 31. Vinsard DG, Mori Y, Misawa M, et al. Quality assurance of computer-aided detection and diagnosis in colonoscopy. Gastrointest Endosc 2019;90(1):55–63. 32. Zhou J, Wu L, Wan X, et al. A novel artificial intelligence system for the assessment of bowel preparation (with video). Gastrointest Endosc 2020;91(2):428–35.e2. 33. Kwak MS, Cha JM, Jeon JW, et al. Artificial intelligence- based measurement outperforms current methods for colorectal polyp size measurement. Dig Endosc 2022;34(6):1188–95. 34. Ichimasa K, Kudo SE, Mori Y, et al. Artificial intelligence may help in predicting the need for additional surgery after endoscopic resection of T1 colorectal cancer. Endoscopy 2018;50(03):230–40. 35. Holzinger A, Langs G, Denk H, et al. Causability and explainability of artificial intelligence in medicine. Wiley Interdiscip Rev Data Min Knowl Discov 2019;9(4):e1312. 36. Watson DS, Krutzinna J, Bruce IN, et al. Clinical applications of machine learning algorithms: Beyond the black box. BMJ 2019;364:l886. 37. Gimeno-Garcia AZ, Hernández-Pérez A, Nicolás-Pérez D, et al. Artificial intelligence applied to colonoscopy: Is it time to take a step forward? Cancers (Basel) 2023;15(8):2193.
Comments (0)