
Remember me

This study collected information on 4449 patients with T2D candidate to oral semaglutide therapy (Fig. S1). As described in Table 1, these patients were 60% males, with a mean age of 63.4 (10.1) years, a relatively short duration of diabetes (< 5 years in 42% of cases), and a mean HbA1c of 7.9 (1.1)%, which was, on average, 1.2% above the recommended target. Most patients had obesity (51%), hypertension (76%), or dyslipidemia (66%), with 19% having three or more cardiovascular risk factors in addition to T2D. Only 14% performed regular physical activity. According to ESC-EASD 2019 definition, the estimated cardiovascular risk was moderated in 6% of the population, high in 61%, and very high in 34%. A total of 15.6% had a prior history of MACE.
Table 1 Characteristics of the populationAccording to ongoing treatment complexity, prior to the recommended change, 9.6% of patients were drug-naïve, 35.6% on oral monotherapy, 35.8% on two oral drugs, 7.7% on three or more oral drugs, and 11.2% on injectable medications, including 1.9% on injectable GLP1-RA and 9.3% on insulin treatment (Table 2). Patients’ characteristics stratified by ongoing treatment complexity are described in Table 1. Further details by patients grouping based on background therapy are available in the supplementary material.
Table 2 Ongoing regimen before oral semaglutideChanges in Medications According to the Proposed RegimenAs described in Table 2, 54.3% of patients added oral semaglutide to the ongoing regimen, leading to an increase in net number of medications (including 1976 subjects adding only oral semaglutide and 438 adding oral semaglutide and other medications at the same time). A switch from other drug classes to oral semaglutide was recommended in 1714 subjects (38.5%), leading to no change in the net number of drug classes. In 321 subjects (7.2%), the addition of oral semaglutide was a substitute for two or more drug classes, leading to a reduction in the number of medications. In the proposed regimen, there was also a minor increase in concomitant use of metformin (from 79.9 to 82.4%) and a significant drop in the use of sulfonylurea (from 14.6 to 2.5%) and insulin (from 9.3% to 6.7%; all p < 0.001), with no change in the concomitant use of SGLT-2i. As expected the concomitant use of DPP4i dropped to almost zero.
Reasons for Choosing Oral SemaglutidePhysicians were asked to report the reason for choosing the initiation of oral semaglutide in each patient. Improvement of metabolic control (80.3%) and reduction of cardiovascular risk (82.9%) were the most common reasons, followed by weight control (63.9%), reduction of microvascular risk (29.3%), and lowering hypoglycemia risk (14.5%).
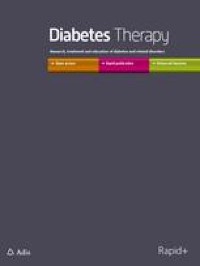
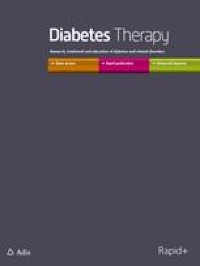
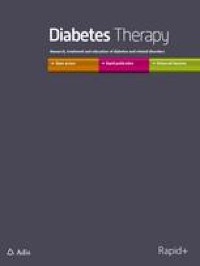
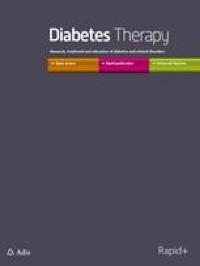
Patient Phenotypes and TrajectoriesWe then evaluated patient phenotypes in relation to the indicated reasons for choosing oral semaglutide. First, as described in Figs. 1 and 2 (and detailed in Table S2), we stratified the population according to the ongoing regimen. While the improvement of metabolic control and reduction of cardiovascular risk were the most reported reasons to choose the drug in all groups, we found some differences. Among patients without concomitant medications (characterized by higher prevalence of obesity and younger age with shorter duration of diabetes), physicians reported a higher impact of weight control (74.8%) and control of microvascular risk (39.8%) compared to patients in other groups (p < 0.0005 for both). Among patients on concomitant therapy with metformin and SGLT-2i, the addition of oral semaglutide was even more driven by the need for improving glycemic control (86.7%). As expected, reduction of hypoglycemia risk was frequently a reported reason among those on metformin plus sulfonylureas (61.9%) or plus insulin (44.2%).
Fig. 1
Patient phenotypes and trajectories by ongoing glucose-lowering regimen. Note: Arrows are reported when the difference between the reported variable in the specific group is significant compared to that in the remaining population. Bold arrows: significant vs overall with study-wide significance p < 0.0005; regular arrows: significant vs overall with nominal p < 0.05
Fig. 2
Reasons for choosing oral semaglutide by ongoing glucose-lowering regimen. Note: Arrows are reported when the difference between the reported variable in the specific group is significant compared to that in the remaining population. Arrows with asterisk: significant vs overall with study-wide significance p < 0.0005; regular arrows: significant vs overall with nominal p < 0.05
When we combined different clinical characteristics in multivariable logistic regression conducted in the entire population (heatmap in Figure S2), we found that younger age, being on SGLT-2i, and higher HbA1c were all independently associated with higher relevance of improving glycemic control as a reason for choosing oral semaglutide. The independent clinical characteristics associated with other reasons to choose oral semaglutide were as follows: younger age and obesity were linked to weight control; lowering hypoglycemia risk was independently associated with prior cardiovascular events and insulin treatment while inversely associated with ongoing use of SGLT-2i (i.e., hypoglycemia was less of a concern when adding oral semaglutide to patients who were already on SGLT-2i); reduction of cardiovascular risk was associated with prior cardiovascular events and younger age and inversely related to ongoing use of injectable therapies (i.e., less of a concern); presence of kidney disease and younger age were associated with reducing microvascular risk as a reason for choosing oral semaglutide.
Estimated Benefits of Adding Oral SemaglutideWe evaluated the expected glycemic improvement in patients who were candidate for oral semaglutide without the concomitant introduction of other diabetes drugs (n = 1869). As shown in Fig. 3A, using the expected HbA1c reduction derived from RCTs, we estimated a reduction of HbA1c from 7.9% to 6.9% (p < 0.0001), with 43% of patients achieving personalized targets, 62% reaching HbA1c < 7%, and 37.6% reaching HbA1c < 6.5%. Similar results were found using estimates from RWE (Fig. 3B).
Fig. 3
Predicted improvements in HbA1c. Prediction of HbA1c reduction and achievement of different glycemic targets were calculated among 1869 patients using oral semaglutide only as add-on therapy. A Estimates done using data from RCTs (PIONEER 2,3,7). B Estimates done using data from the IGNITE real-world evidence (RWE) study. C Comparison of expected benefit (proportion of subjects achieving HbA1c < 7%) from the addition of oral semaglutide versus empagliflozin or sitagliptin, among n = 1259 subjects without SGLT-2 or DPP-4 inhibitors as background regimen
Finally, we compared the proportion of patients who were expected to achieve a HbA1c value < 7% among those with clinical characteristics similar to the respective RCT evaluating oral semaglutide versus sitagliptin or versus empagliflozin. Based on RCT results applied to our population (Fig. 3C), a larger proportion of patients was expected to reach HbA1c < 7% with oral semaglutide than with sitagliptin or empagliflozin (p < 0.0001 for both comparisons).
Comments (0)