Gastric cancer tends to metastasize to the lymph nodes, liver, and peritoneum [5, 6]. In contrast, recurrent tumors that cause biliary obstruction are reportedly seen in 1.4% to 2.3% of patients undergoing resection of gastric cancer, and in most of these cases, the recurrence sites are the lymph nodes in the hepatoduodenal ligament. Thus, cases of isolated extrahepatic bile duct metastasis from gastric cancer are rare [7, 8]. A search of the literature from 1980 to the present day using Igaku Chuo Zasshi, a web-based Japanese literature engine, and PubMed (keywords: gastric cancer, bile duct metastasis) revealed only four cases [9,10,11,12]. We summarized all five known cases including the present case (Table 1). Only Poletto et al. reached a diagnosis of extrahepatic bile duct metastasis from gastric cancer before treatment. In their report, immunohistochemical staining showed the markers expressed in the biopsied tissue from the bile duct and the primary site in the stomach were the same. The case described by Poletto et al. and the present case were similar in that the biopsy from the bile duct demonstrated cancer. It is paradoxical because the metastatic site in the bile duct mainly spread to the fibromuscular layer, and not to the mucosal layer, in all five cases. As Poletto et al. suspected, biopsy tissue might be obtained concomitantly from the mucosal surface and the fibromuscular layer. Similar to previous reports, we diagnosed extrahepatic bile duct metastasis from gastric cancer on the basis of the following: absence of cancer cells in the mucosa of the bile duct; the same histological type between gastric cancer and the bile duct tumor; and the same findings of immunohistochemical staining. In particular, immunohistochemical staining is critical as decisive diagnostic evidence.
Table 1 Summary of the five cases of extrahepatic bile duct metastasis from gastric cancerThe present case is, to our knowledge, the first to report gastric cancer simultaneously complicated with extrahepatic bile duct metastasis and PVTT. Ozeki et al. mentioned the three developmental mechanisms of PVTT accompanied by gastric cancer: formation of tumor thrombus due to direct infiltration to the portal vein; infiltration from liver metastasis to the portal vein; and coexistence of gastric cancer and hepatocellular carcinoma complicated with PVTT [13]. Because the present case showed neither liver metastasis nor coexistent hepatocellular carcinoma, the gastric cancer directly infiltrated the portal vein.
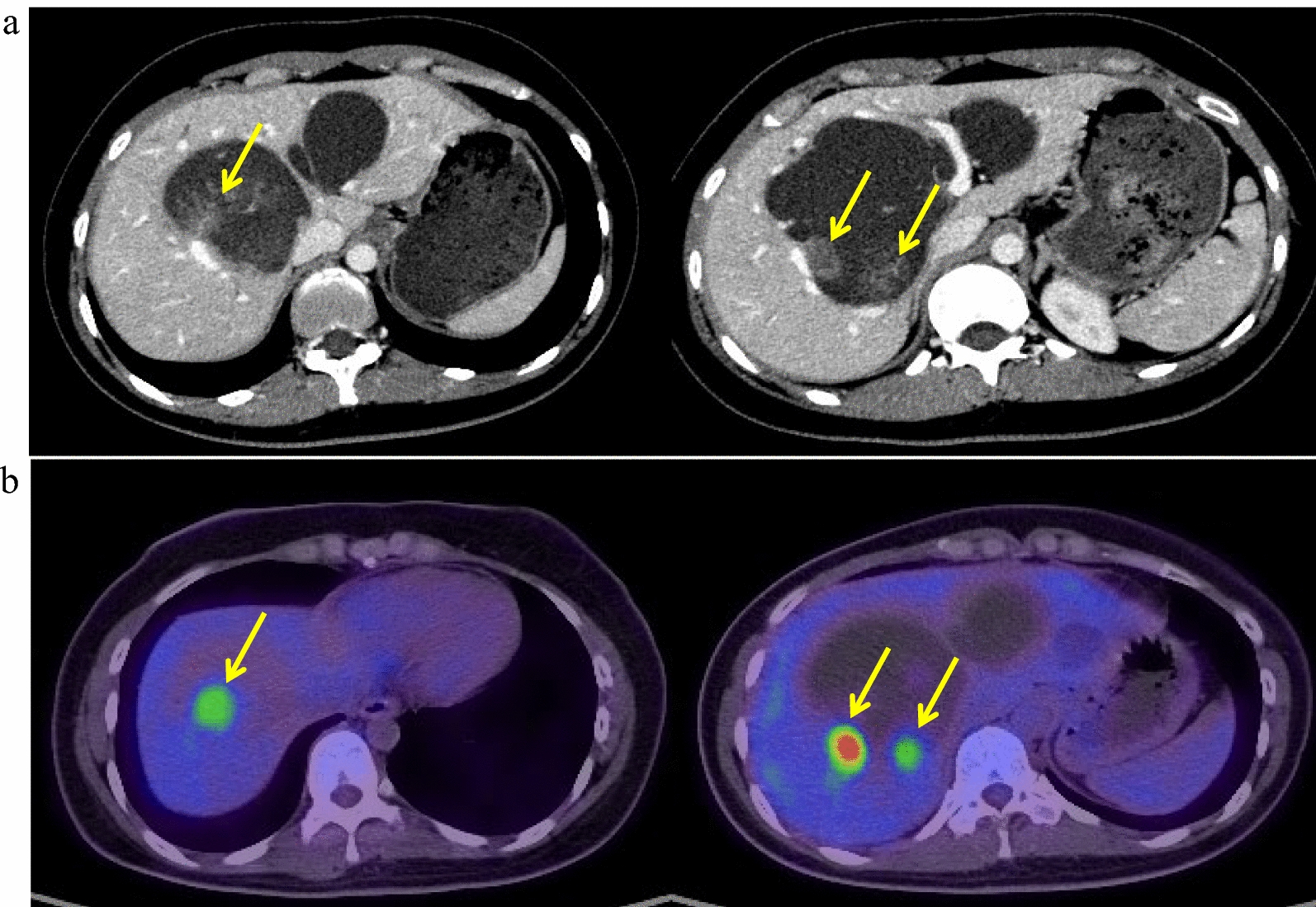
In the present case, it was very difficult to identify the metastatic route because of the presence of many lymph node metastases and PVTT. Although gastric cancer showed advanced lymphatic involvement in the supra-pyloric site and hepatoduodenal ligament neighboring the lower bile duct, which may indicate metastatic route from gastric cancer to the bile duct via a lymphatic route, we considered the metastatic route via a hematogenous route was more likely based on the following findings. Firstly, advanced histological venous involvement was observed in the primary gastric site. Secondly, cancer cells slightly infiltrated the pancreatic tissues between PVTT and the site of bile duct metastasis. Thirdly, PVTT directly indicated hematogenous infiltration. Fourthly, multiple liver metastases followed by lung metastases, both of which were supposed to develop hematogenously, were seen in the early postoperative period.
As a treatment strategy, systemic chemotherapy is generally recommended for gastric cancer with distant metastasis or PVTT. Whereas it is difficult to discuss the treatment strategy for extrahepatic bile duct cancer with PVTT because few cases have been reported previously [14, 15], some papers reported long-term survival after resection of gastric cancer with PVTT following systemic chemotherapy [16, 17]. Waseda et al. reported that chemotherapy should be conducted at first even if gastric cancer with PVTT is considered resectable because PVTT is a poor prognostic factor [18]. Although we preoperatively diagnosed simultaneous gastric cancer and distal bile duct cancer, we could have diagnosed that the bile duct tumor was a metastatic lesion and that PVTT was derived from gastric cancer if immunohistochemical staining for biopsied tissues had been performed before the treatment. If we had reached the correct diagnosis, we would have selected systemic chemotherapy for far-advanced gastric cancer.

Comments (0)