The time interval between the initial breast cancer and gastrointestinal metastasis varies considerably from synchronous presentation to > 20 years after the diagnosis of the primary lesion [10, 11]. Mutations in E-cadherin, which contributes to cell adhesion, may be related to the susceptibility of ILCs to spread to the gastrointestinal tract [12, 13]. In approximately 1% of cases, gastrointestinal involvement is found to be the first distant metastasis [14]. For an accurate diagnosis, it is necessary to evaluate the histopathological characteristics of primary and metastatic foci. In terms of immunohistochemical surveys, ER and GATA3 positivity and caudal type homeobox 2 (CDX2) negativity may support the diagnosis of gastrointestinal metastases from breast cancer. Additionally, the usefulness of mammaglobin and GCDFP15 molecular markers has been reported in several studies [6, 15]. However, the properties of hormone receptors are not always consistent with those of the initial lesions [16]. In the present study, the expression of PgR in Cases 1 and 3 differed between the foci.
Since the clinical manifestations associated with gastrointestinal metastases are nonspecific, including abdominal pain, diarrhea, nausea, and sometimes asymptomatic, breast cancer is rarely detected based on these symptoms [17, 18]. In this report, vomiting and melena were observed in Case 1, while Case 2 experienced diarrhea and vomiting. In Case 1, bleeding from a Dieulafoy ulcer was indicated, but this was not evident from the metastatic mass in the descending colon. Colonic metastases from breast cancer have been reported to show diffuse intestinal wall thickening and ulcerated or nodular lesions, and endoscopic findings often resemble primary colon cancer or inflammatory bowel disease [19, 20]. Although a biopsy of the hemorrhagic site was not performed in this case, tumor infiltration may have played a role in the colorectal bleeding.
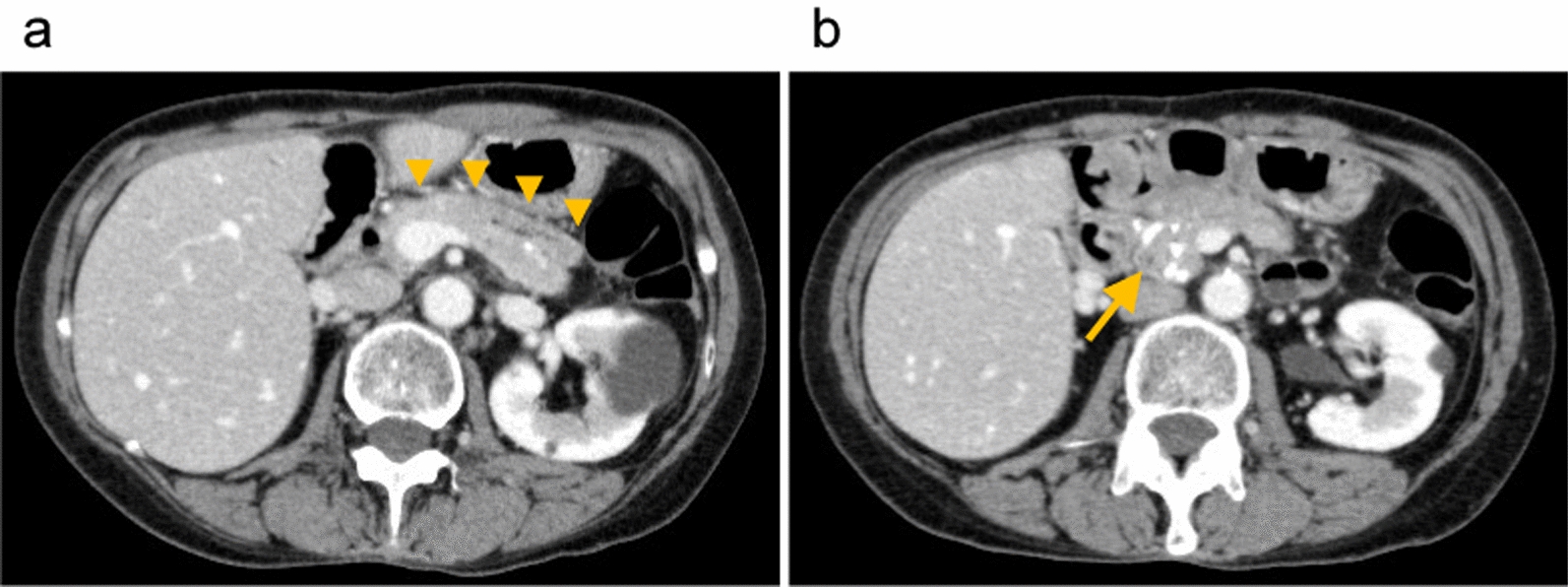
In Case 2, as metastatic masses in the transverse colon were responsible for intestinal obstruction, an ileosigmoid colon bypass was performed. Rapid examination and diagnosis of primary and metastatic lesions enabled early hormonal treatment after the improvement of abdominal manifestations.
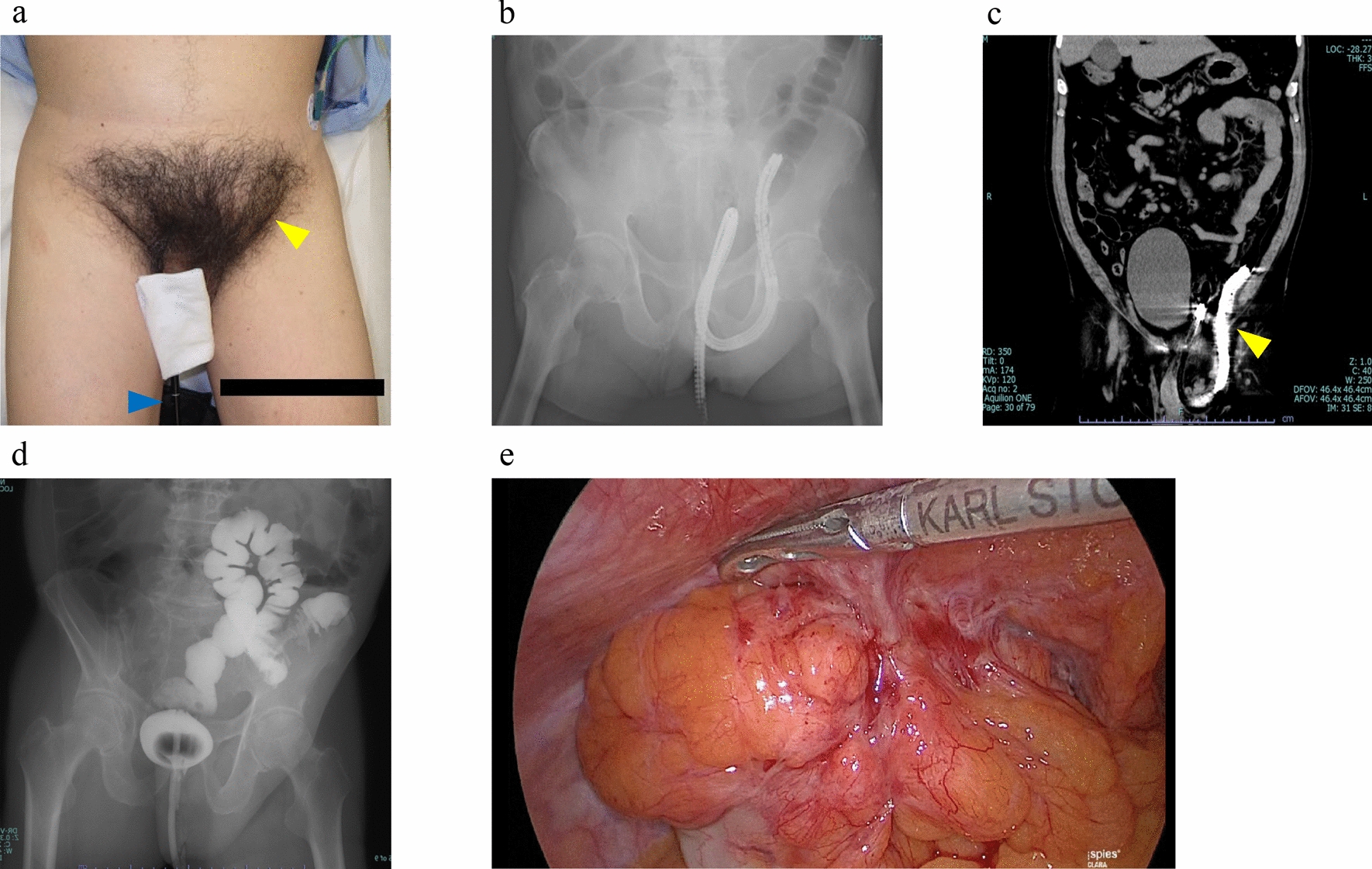
Although Case 3 had no gastrointestinal symptoms, colonic metastasis was found due to elevated CEA levels during the postoperative follow-up of ILC. However, once the metastatic focus was resected, the tumor recurred and penetrated the abdominal wall. Colonic perforation or infiltration of the abdominal wall, which is implicated in metastatic lesions, is extremely rare. This was possibly associated with rapid tumor growth and increased bowel pressure due to intestinal stenosis. Also, high tumor invasiveness due to loss of E-cadherin might be related to this phenomenon. In this case, the fistula gradually shrank with surgical drainage, and temporary tumor regression was observed with chemotherapy. It was an intractable disease, and the metastatic lesion re-enlarged, causing a recurrence of the abdominal wall perforation and an abscess 8 months later. Nevertheless, the surgical treatment for gastrointestinal manifestations followed by systemic therapy for primary breast cancer was effective similar to that in Case 2.
Survival after gastrointestinal metastases is generally poor, and few patients survive for more than 2 years [6]. In this report, Case 1, in which BSC was provided, died 4 months after diagnosis. In contrast, the survival time was 1 year and 2 months after the detection of gastrointestinal metastasis in Case 2 and 3 years and 8 months in Case 3, who underwent systemic treatment subsequent to invasive procedures.

Comments (0)