
Remember me




Intraventricular hemorrhage (IVH) is a type of bleeding that occurs within the ventricular system of the brain, which comprises four interconnected cavities filled with cerebrospinal fluid. IVH can be caused by various conditions, including traumatic brain injury, vascular malformations, and hypertension. In adults, IVH is most commonly associated with hypertensive intracerebral hemorrhage (ICH), a type of bleeding that results from high blood pressure.1 Hypertensive ICH-related IVH occurs when bleeding from the initial site of the hemorrhage extends into the ventricular system.2 Primary IVH, which occurs without any obvious cause, is another type of IVH that occurs in adults.3,4 Primary IVH is often associated with rupture of small blood vessels in the brain and can result in significant morbidity and mortality.3,5 Both hypertensive ICH-related and primary IVH require prompt diagnosis and treatment to prevent further neurological damage.
Several studies have investigated the use of urokinase in the treatment of IVH in adults. A study conducted by Naff et al6 with 12 patients found that urokinase use was associated with a positive impact on the rate of intraventricular clot resolution. In addition, a meta-analysis conducted by van Solinge et al including 19 studies encompassing 1020 patients7 found that urokinase use was associated with a significant reduction in mortality rates and a lower incidence of external ventricular drainage (EVD) obstruction in patients with IVH. These studies suggest that urokinase may be a feasible treatment option for IVH in adults; however, further research is required to determine the optimal dose and timing of urokinase administration. Furthermore, there is still a paucity of evidence to suggest that the use of urokinase could ameliorate functional outcomes or reduce the dependency on permanent CSF diversion.
To evaluate the efficacy of urokinase in the treatment of IVH, we assessed the association between intraventricular urokinase use and IVH volume. We examined the association between changes in IVH volume and clinical outcomes including functional outcomes and shunt dependency rate. To test these hypotheses, we analyzed the data to investigate whether urokinase administration was associated with a reduction in IVH volume, and whether this reduction in IVH volume was associated with improved clinical outcomes.
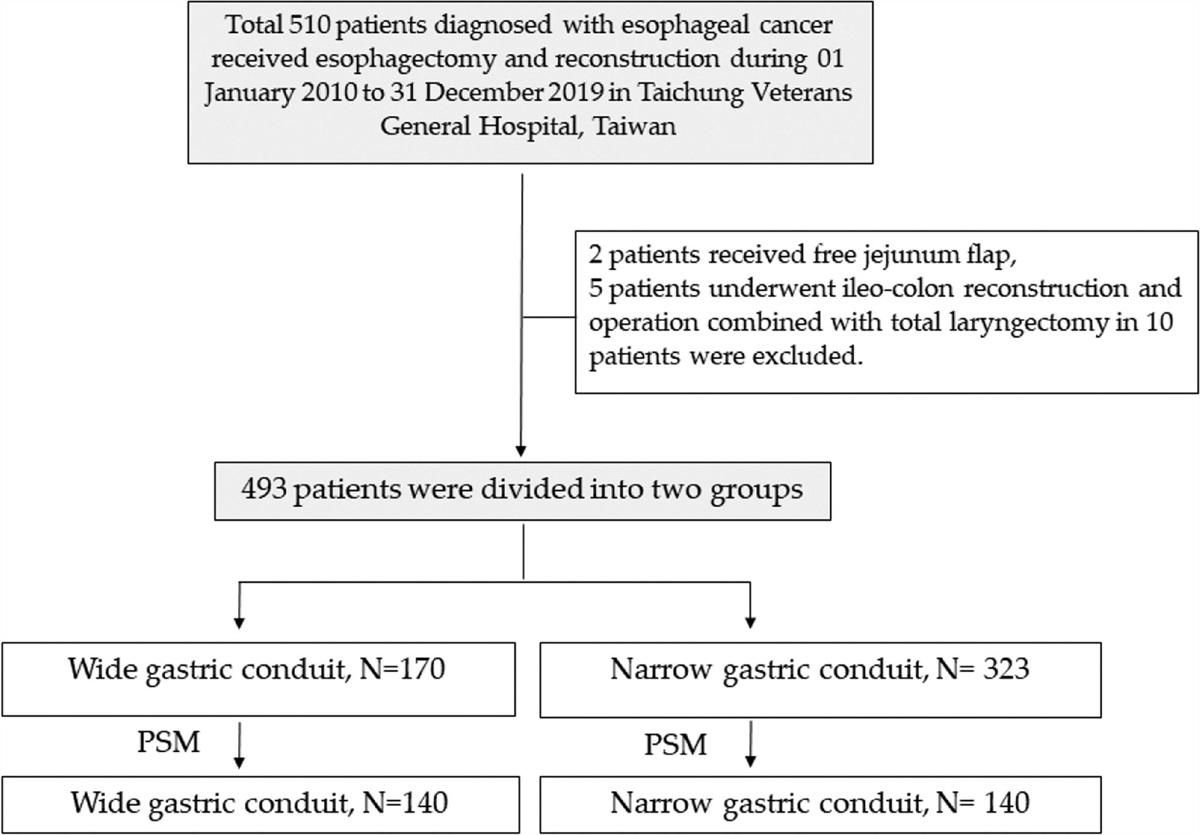
2. METHODSThis retrospective study was approved by the Institutional Review Board of the Taichung Veterans General Hospital. Our research adhered to the ethical standards set forth by the Institutional Review Board (No. CE22334A) and conformed to the guidelines for human research ethics. The study was conducted from 2015 to 2021, including 179 patients with spontaneous ICH accompanied by ventricular extension or primary IVH that hemorrhage only presenting in the ventricular system. Patients who met any of the following criteria were excluded from the study: vascular lesion-related cases, the presence of associated traumatic subarachnoid or subdural hemorrhage, hemorrhage related to brain tumors, or hemorrhagic transformation from ischemic stroke. Patients who did not undergo EVD surgery were excluded. A total of 94 patients were finally enrolled in this study. The recruitment process was shown in Fig. 1. Written informed consent was obtained from all the participants.
 Fig. 1:
Fig. 1: Flow diagram of inclusion and exclusion process.
In this study, non-contrast computed tomography scans were obtained on admission and on day 7 after the surgical intervention (at least 24 h after the final intrathecal administration of urokinase). IVH severity was quantified using the modified Graeb scoring system (mGRAEB).8 The scoring system was used to measure the amount of blood that accumulated in each brain ventricle. The maximum score that could be obtained was 32, which was based on the accumulation of blood in specific areas, including the fourth ventricle (maximum score of 4), third ventricle (maximum score of 4), right and left lateral ventricles (maximum score of 4 for each), right and left occipital horns (maximum score of 2 for each), and the right and left temporal horns (maximum score of 2 for each). In cases where a blood clot extended beyond the normal boundary of these areas, an additional score of +1 was assigned to each compartment.
The main goal was to identify the association between IVH volume reduction and urokinase administration. The primary outcome was the change in the mGRAEB score between the EVD only and EVD combined with fibrinolysis groups. The secondary functional outcome was the modified Rankin Scale (mRS) score at discharge. Additionally, the rate of permanent cerebrospinal fluid (CSF) diversion was documented in both groups 3 months after discharge.
2.1. Statistical analysisIn the statistical analysis, categorical variables were analyzed using the Chi-square test. The Mann–Whitney U test was used to describe continuous variables. Data were reported as counts (percentages) or medians (IQRs). Patients were grouped into “EVD combined with fibrinolysis” and “EVD only’’ groups. Shunt-related factors were compared between the two groups. Statistical significance was set at p < 0.05.
3. RESULTSBetween 2015 and 2021, 179 patients with IVH were admitted to our hospital. Based on the exclusion criteria, we excluded patients with vascular lesion-related cases (intracranial aneurysm, arteriovenous malformation, or sinus thrombosis that complicated with hemorrhage), trauma, and preexisting intracerebral tumors or infections (n = 65). Twenty patients were excluded because of the lack of EVD insertion. A total of 94 patients were therefore enrolled in this study. The recruitment process was shown in Fig. 1.
Among the 94 patients, 66 (70.2%) received intraventricular urokinase (fibrinolytic group) and 28 (29.8%) received external CSF drainage only (EVD only group). No observable differences in characteristics of the study population, including sex, age, GCS score upon arrival, and percentage of patients with comorbid hypertension and diabetes, were found between the two groups (Table 1). In addition, no statistically significant differences in ICH characteristics, including hematoma location and volume, were observed between the two groups.
Table 1 - Characteristics of the study population Total EVD + urokinase EVD only p Patient number 94 66 28 Sex 0.192 Female 25 (26.6%) 15 (22.7%) 10 (35.7%) Male 69 (73.4%) 51 (77.3%) 18 (64.3%) Age 65.0 (55.8-75.3) 63.5 (54.8-72.8) 69.0 (57.0-78.8) 0.387 Hypertension 83 (88.3%) 59 (89.4%) 24 (85.7%) 0.727 Type II DM 20 (21.3%) 15 (22.7%) 5 (17.9%) 0.598 GCS at arrival 13.0 (8.0-15.0) 12 (7.8-15.0) 13.5 (10.0-15.0) 0.226 ICH location 0.565 Basal ganglion 64 (68.1%) 46 (69.7%) 18 (64.3%) Cerebellar/pons 10 (10.6%) 7 (10.6%) 3 (10.7%) Lobar 3 (3.2%) 1 (1.5%) 2 (7.1%) Primary IVH 17 (18.1%) 12 (18.2%) 5 (17.9%) ICH volume 9.1 (4.4-16.6) 10.245 (5.8-19.2) 5.7 (3.8-10.7) 0.077The results of the IVH severity analysis based on mGRAEB score changes between the first and seventh day showed no discrepancies between the two groups (Table 2). The seventh-day median (IQR) mGRAEB score of the fibrinolytics group was (4.0 [2.0-6.0]) while the EVD-only group was (5.5 [3.0–7.0]) with (p = 0.102). The reduction in mGRAEB score within 7 days also showed no difference between the two groups (−5.0 [−8.0 to −2.0] vs −2.5 [−9.0 to −1.0]; p = 0.124). The reduction rate in mGRAEB score was also not significantly different between the two groups (−50.0 [−64.4 to −32.5] % vs −44.2 [−59.3 to −7.9] %; p = 0.489).
Table 2 - IVH severity analysis EVD + urokinase EVD only p mGRAEB score at arrival 11 (7.8 to 16.0) 9 (4.3 to 12.8) 0.114 mGRAEB score at 7th day 5.5 (3.0 to 7.0) 4 (2.0 to 6.0) 0.102 mGRAEB score of 3rd and 4th ventricle at arrival 7 (4.0 to 9.0) 4.5 (0.5 to 9.0) 0.119 mGRAEB score of 3rd and 4th ventricle at 7th day 2 (0.0 to 2.0) 0 (0.0 to 2.0) 0.091 Reduction of mGRAEB score −5 (−8.0 to −2.0) −2.5 (−9.0 to −1.0) 0.124 Reduction of mGRAEB score of 3rd and 4th ventricle −4 (−7.0 to −2.0) −2.5 (−5.0 to 0.0) 0.110 Reduction rate of mGRAEB score (%) −50.0 (−64.4 to −32.5) −44.2 (−59.3 to −7.9) 0.489 Reduction rate of mGRAEB score of 3rd and 4th ventricle (%) −75.0 (−100.0 to −50.0) −71.4 (−100.0 to −50.0) 0.677Further investigation of the mGRAEB score for the third and fourth ventricle also revealed negative findings between the two groups. A reduction in mGRAEB scores for the third and fourth ventricle within a 7-day period showed no difference between the two groups (−4.0 [−7.0 to −2.0] vs −2.5 [−5.0 to −0.0]; p = 0.11). In addition, the reduction rate in mGRAEB scores for the third and fourth ventricle revealed no statistical difference (−75.0 [−100.0 to −50.0] % vs −71.0 [−100.0 to −50.0] %; p = 0.677).
3.2. Secondary analysis findingsIn terms of functional outcomes, the mRS upon discharge (5.0 [4.0-5.0] vs. 4.5 [4.0-5.0], p = 0.674) did not show significant differences between these two groups. In contrast, 22 patients (33.3%) in the fibrinolytic group required permanent shunt placement, whereas 11 (39.3%) in the EVD-only group underwent permanent shunt surgery (p = 0.58) (Table 3).
Table 3 - Functional outcome and shunt dependency analysis Total EVD + urokinase EVD only p MRS 5.0 (4.0-5.0) 5.0 (4.0-5.0) 4.5 (4.0-5.0) 0.674 Shunt placement 0.580 No 61 (64.9%) 44 (66.7%) 17 (60.7%) Yes 33 (35.1%) 22 (33.3%) 11 (39.3%)According to the literature, up to 45% of patients with ICH may experience IVH and subsequent hydrocephalus, which independently contribute to unfavorable outcomes.9–13 Multiple factors may lead to neurological deterioration and mortality, including the development of hydrocephalus, excess intracranial volume, and increased intracranial pressure.14 The timely identification and clearance of IVH may prevent secondary deteriorations associated with IVH, such as increased intracranial pressure, brain swelling, and reduced blood flow. Therefore, the early management of IVH is critical to minimize the risk of mortality and long-term complications.
Among patients with IVH enrolled in our study, we found that the use of intraventricular urokinase was associated with a reduction in IVH severity and a lower 30-day mortality rate. However, our findings are consistent with the existing literature,7,15,16 insofar as no difference was observed in functional outcomes or shunt dependency. In addition, studies investigating the efficacy of fibrinolytic agents, such as recombinant tissue plasminogen activator, in patients with IVH have also reported similar findings.17,18
According to the CLEAR III trial, the removal of >80% of the initial IVH volume resulted in less disability; however, the mean IVH removal rate in the study was only 65% in the fibrinolytic group.19 This result implies that the confounding influence of the residual IVH could have concealed positive effects on the study outcomes. On the other hand, the less than expected results in fibrinolysis also suggest the complex pathway that alteplase takes from the ventricular system to the brain parenchyma. Further studies exploring the communication system of CSF between the perivascular space and surrounding vessels could shed light on how to achieve a more effective fibrinolytic response.
In this retrospective study, we found that the residual IVH volumes of the third and fourth ventricles did not show heterogeneity between the EVD only and EVD combined with fibrinolytics groups. This finding might be explained by the lack of a significant difference in shunt dependency between the two groups. According to a 2015 study conducted by Hughes et al,20 both the third and fourth IVH volumes were relevant to external CSF drainage requirements. Similar findings were reported by Stein et al21 and Young et al,22 respectively. Given the demonstrated relevance of third and fourth IVH volumes with external CSF drainage requirements in previous studies,23,24 our finding of no heterogeneity in residual IVH volume between the EVD only and EVD combined with fibrinolytic groups raises the possibility that persistent IVH may be associated with permanent CSF diversion.
One of the strengths of this study is its focus on multiple significant clinical and functional outcomes, which is integral in comprehensively assessing the implications of the research. In addition, the inclusion of several critical clinical measures enhances the depth of the analysis. However, there are limitations to be acknowledged; the study has a relatively small sample size, which may limit the generalizability of the findings. Additionally, its retrospective design could potentially introduce biases that may affect the interpretation of the results.
In conclusion, this retrospective study found no significant association between intraventricular urokinase administration and reductions in IVH severity. In addition, no association was observed between changes in urokinase levels and improved functional outcomes or shunt dependency. Although the existing literature has described decreased mortality after urokinase administration, we should be more cognizant of how we select patients who may derive optimal benefit from intraventricular urokinase administration.
ACKNOWLEDGMENTSWe would like to thank Editage (www.editage.com) for English language editing.
REFERENCES 1. Hinson HE, Hanley DF, Ziai WC. Management of intraventricular hemorrhage. Curr Neurol Neurosci Rep 2010;10:73–82. 2. Hallevi H, Dar NS, Barreto AD, Morales MM, Martin-Schild S, Abraham AT, et al. The IVH score: a novel tool for estimating intraventricular hemorrhage volume: clinical and research implications. Crit Care Med 2009;37:969–74, e1. 3. Flint AC, Roebken A, Singh V. Primary intraventricular hemorrhage: yield of diagnostic angiography and clinical outcome. Neurocrit Care 2008;8:330–6. 4. Pai A, Hegde A, Nair R, Menon G. Adult primary intraventricular hemorrhage: clinical characteristics and outcomes. J Neurosci Rural Pract 2020;11:623–8. 5. Barnaure I, Liberato AC, Gonzalez RG, Romero JM. Isolated intraventricular haemorrhage in adults. Br J Radiol 2017;90:20160779. 6. Naff NJ, Hanley DF, Keyl PM, Tuhrim S, Kraut M, Bederson J, et al. Intraventricular thrombolysis speeds blood clot resolution: results of a pilot, prospective, randomized, double-blind, controlled trial. Neurosurgery 2004;54:577–83. 7. van Solinge TS, Muskens IS, Kavouridis VK, Gormley WB, Mekary RA, Broekman MLD, et al. Fibrinolytics and intraventricular hemorrhage: a systematic review and meta-analysis. Neurocrit Care 2020;32:262–71. 8. Morgan TC, Dawson J, Spengler D, Lees KR, Aldrich C, Mishra NK, et al.; CLEAR and VISTA Investigators. The Modified Graeb Score: an enhanced tool for intraventricular hemorrhage measurement and prediction of functional outcome. Stroke 2013;44:635–41. 9. Diringer MN, Edwards DF, Zazulia AR. Hydrocephalus: a previously unrecognized predictor of poor outcome from supratentorial intracerebral hemorrhage. Stroke 1998;29:1352–7. 10. Phan TG, Koh M, Vierkant RA, Wijdicks EF. Hydrocephalus is a determinant of early mortality in putaminal hemorrhage. Stroke 2000;31:2157–62. 11. Ziai WC, Nyquist PA, Hanley DF. Ventriculostomy and lytic therapy for intracerebral hemorrhage. Front Neurol Neurosci 2015;37:130–47. 12. Witsch J, Bruce E, Meyers E, Velazquez A, Schmidt JM, Suwatcharangkoon S, et al. Intraventricular hemorrhage expansion in patients with spontaneous intracerebral hemorrhage. Neurology 2015;84:989–94. 13. Witsch J, Falcone GJ, Leasure AC, Matouk C, Endres M, Sansing L, et al. Intracerebral hemorrhage with intraventricular extension associated with loss of consciousness at symptom onset. Neurocrit Care 2021;35:418–27. 14. You S, Zheng D, Delcourt C, Sato S, Cao Y, Zhang S, et al. Determinants of early versus delayed neurological deterioration in intracerebral hemorrhage. Stroke 2019;50:1409–14. 15. Torres A, Plans G, Martino J, Godino O, Garcia I, Gracia B, et al. Fibrinolytic therapy in spontaneous intraventricular haemorrhage: efficacy and safety of the treatment. Br J Neurosurg 2008;22:269–74. 16. Coplin WM, Vinas FC, Agris JM, Buciuc R, Michael DB, Diaz FG, et al. A cohort study of the safety and feasibility of intraventricular urokinase for nonaneurysmal spontaneous intraventricular hemorrhage. Stroke 1998;29:1573–9. 17. Huttner HB, Tognoni E, Bardutzky J, Hartmann M, Köhrmann M, Kanter I-C, et al. Influence of intraventricular fibrinolytic therapy with rt-PA on the long-term outcome of treated patients with spontaneous basal ganglia hemorrhage: a case-control study. Eur J Neurol 2008;15:342–9. 18. Witsch J, Roh DJ, Avadhani R, Merkler AE, Kamel H, Awad I, et al. Association between intraventricular alteplase use and parenchymal hematoma volume in patients with spontaneous intracerebral hemorrhage and intraventricular hemorrhage. JAMA Netw Open 2021;4:e2135773. 19. Hanley DF, Lane K, McBee N, Ziai W, Tuhrim S, Lees KR, et al.; CLEAR III Investigators. Thrombolytic removal of intraventricular haemorrhage in treatment of severe stroke: results of the randomised, multicentre, multiregion, placebo-controlled CLEAR III trial. Lancet 2017;389:603–11. 20. Hughes JD, Puffer R, Rabinstein AA. Risk factors for hydrocephalus requiring external ventricular drainage in patients with intraventricular hemorrhage. J Neurosurg 2015;123:1439–46. 21. Stein M, Luecke M, Preuss M, Boeker DK, Joedicke A, Oertel MF. Spontaneous intracerebral hemorrhage with ventricular extension and the grading of obstructive hydrocephalus: the prediction of outcome of a special life-threatening entity. Neurosurgery 2010;67:1243–51. 22. Young WB, Lee KP, Pessin MS, Kwan ES, Rand WM, Caplan LR. Prognostic significance of ventricular blood in supratentorial hemorrhage: a volumetric study. Neurology 1990;40:616–9. 23. Murthy SB, Awad I, Harnof S, Aldrich F, Harrigan M, Jallo J, et al.; CLEAR III Trial Investigators. Permanent CSF shunting after intraventricular hemorrhage in the CLEAR III trial. Neurology 2017;89:355–62. 24. Kuo LT, Lu HY, Tsai JC, Tu YK. Prediction of shunt dependency after intracerebral hemorrhage and intraventricular hemorrhage. Neurocrit Care 2018;29:233–40.
Comments (0)