To the best of our knowledge, this study is the first multinational, prospective, and long-term follow-up investigation that sheds light on the phenotypic differences of patients with COVID-19 vaccination-related prolonged/worsened headaches. Our findings reveal that these headaches can be categorized into two distinct clusters based on their headache phenotypes. Cluster 1 comprises patients with migraine-like headache features, characterized by throbbing, more severe headaches primarily localized in the frontal region. These patients have a positive history of primary headaches and experience accompanying symptoms such as nausea, photo/phono/osmophobia, and worsened symptoms with physical activity. In contrast, patients in Cluster 2 present with pressing or stabbing headaches of longer duration (more than 1 month). An additional noteworthy finding of our study is the persistence of headache characteristics observed in patients within these Clusters during the long-term (6-month) prospective follow-up period. Although there was a trend of improvement in headache symptoms over time, the overall phenotypic profile of these patients remained relatively stable. This indicates that the specific headache phenotypes identified in the Clusters maintained their characteristics and did not undergo significant changes throughout the follow-up period.
Characteristics of COVID-19 vaccination related headaches, and headache features in patients with a primary headache disorder history
Headache was reported as the fifth most common adverse event following COVID-19 vaccination during the acute phase [14]. Most observations report that headache typically starts within a time window of 72 h after the vaccination process [3, 6, 15]. In a recent study that evaluated new or worsening headaches within 16 days after COVID-19 vaccination, it was found that 289 patients experienced headaches that were temporally correlated with the vaccination. The study reported that regardless of the classification of headache (primary vs. secondary) or the type of vaccine, a migraine-like clinical phenotype was observed in these patients [16]. In a study by Ekizoğlu et al., the authors evaluated vaccine-related headache characteristics in 1819 healthcare personnel who predominantly received the inactivated vaccine (CoronaVac; Sinovac Life Sciences). The study found that headache was more predominant in the female population, with a higher prevalence compared to males (36.1% vs. 19.3%). Additionally, a subset of participants (12.1–16.9%) reported accompanying symptoms resembling migraine, such as nausea, photophobia, and phonophobia. These findings suggest that vaccine-related headaches can exhibit migraine-like features in some individuals [6]. In a separate online survey study involving 1372 fully vaccinated individuals, headache associated with COVID-19 vaccination was commonly described as a pressing sensation that involved the entire cranium. The majority of participants reported moderate-intensity headaches regardless of the vaccine type received. Additionally, the duration of these vaccine-related headaches was generally short, with a median of 2 days from onset to resolution [17]. In another observational study that utilized online questionnaires, 2464 individuals who received the AZD1222 (AstraZeneca) vaccine were assessed. The study found that headache typically began approximately 14.5 ± 21.6 h after vaccination and lasted for an average duration of 16.3 ± 30.4 h. The reported characteristics of the headache included bilateral location in 75.8% of participants, a pressing sensation in 50.4%, and a dull sensation in 37.7%. Regarding headache intensity, 38.7% of participants described it as severe, 35.2% as moderate, and 15.5% as very severe. Interestingly, this study also revealed that migraine-like symptoms, including aggravation of pain during physical activity and sensitivity to light and sound (photo/phonophobia), were reported by the participants who experienced headache after the vaccination. This suggests that the headache experienced in this context may share some similarities with migraine headaches, further highlighting the overlap in symptoms between COVID-19 vaccine-related headaches and migraine [18].
Although headache was mostly reported to be transient after vaccination, it sometimes can be resistant and long-lasting in some patients [14]. Especially in patients with a primary headache disorder, headache might be longer in duration and more severe/intense [1, 15]. According to the study conducted by Silvestro et al., using an online questionnaire, it was reported that among 841 migraine patients, 66.47% of patients after the 1st dose and 60.15% of patients after the 2nd dose of COVID-19 vaccination experienced a headache attack starting after 1 h to 7 days. These vaccine-related headaches were described as more severe (50.62%), long-lasting (52.80%), and longer in duration (49.69%) compared to their usual migraine attacks [19]. Sekiguchi et al. reported that the rates of COVID-vaccine-related headaches were reported as 30.9% after the 1st dose and 66.2% after the 2nd dose in patients with a primary headache history. In comparison, the rates were 13.6% after the 1st dose and 32% after the 2nd dose in individuals without a headache history. These findings suggest that patients with a pre-existing primary headache disorder may be more prone to experience vaccine-related headaches compared to those without a headache history [1]. The findings of our study are consistent with these previous studies mentioned. In patients with a pre-existing headache disorder who developed COVID-vaccination-related headaches, we observed a shorter onset of headache, with most headaches being described as throbbing in quality. Additionally, symptoms such as photophobia, phonophobia, and osmophobia were more prominent in these patients. These observations align with the notion that patients with a pre-existing headache disorder may experience distinct characteristics in their COVID-vaccination-related headaches.
In our study, gender was found to have no effect on the clustering of headache phenotypes (gender distribution was similar in both clusters; p = 0.550). Nonetheless, we believe that a prospective study with a larger sample of patients, specifically focusing on gender differences in terms of long COVID symptoms, including headache, would be beneficial for a more comprehensive understanding and management of headaches associated with COVID-19 vaccination.
Similarly, age had no significant effect on the formation of distinct headache clusters related to COVID-19 vaccination (p = 0.162, Supplementary table 4). Further prospective studies are required to draw more definitive conclusions on this matter.
As an additional noteworthy finding, the comparison of Mig-SCog scale scores between patient visits suggests that cognitive involvement in our group of patients with post-vaccination headache was not severe and exhibited a gradual improvement over time.
Cluster analysis of headaches in patients with a prolonged/worsened COVID-19 vaccination-related headaches
There are only a few studies available that have examined the long-term course of prolonged/worsened COVID-19 vaccination-related headaches. In our study, we found that these headaches can be categorized into two distinct phenotypic clusters, and these phenotypes tend to maintain their characteristics over a 6-month follow-up period. The first cluster consisted of headaches that resembled migraine-like features, including throbbing pain, greater severity, and accompanying symptoms such as nausea, photophobia, and phonophobia. These headaches were exacerbated by physical activity and were more common in patients with a history of primary headaches. The second cluster included headaches with a tension-type phenotype, characterized by pressing or stabbing pain and longer duration (over 1 month). After 6 months of follow-up, 52.32% of patients in cluster 1 and 42.04% in cluster 2 still experienced ongoing (prolonged) headaches. Notably, patients in cluster 1 maintained their headache characteristics without significant changes over the 6-month period. Furthermore, we observed a decrease in headache severity across all patients throughout the 6 months of follow-up.
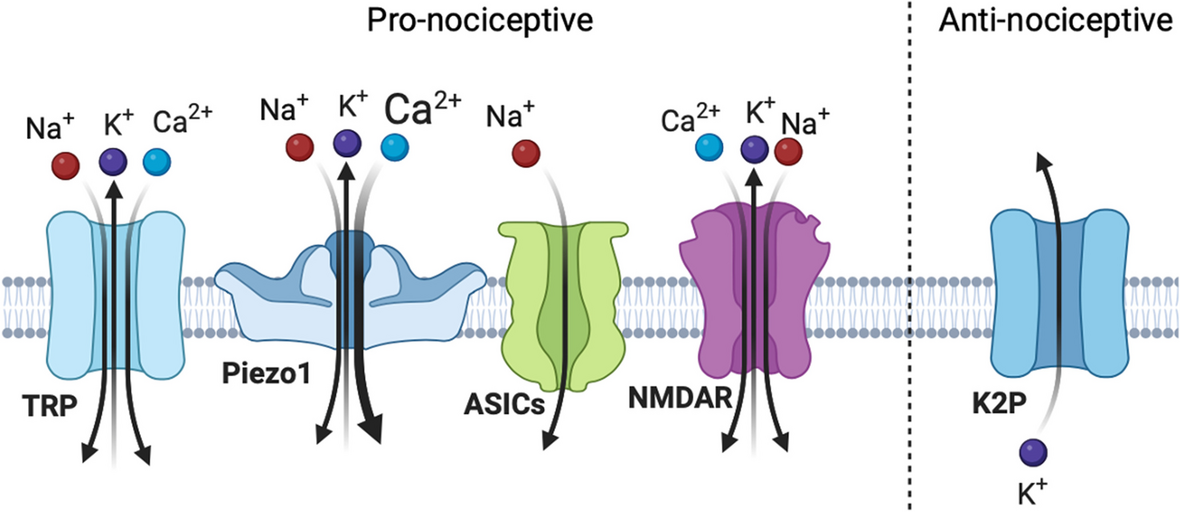
The exact pathophysiology underlying headaches related to COVID-19 vaccination is not yet fully understood, and several hypotheses are being explored. One hypothesis is related to the hyperexcitability of the trigeminovascular system (TVS) and the sensitization of trigeminal nerve fibers. It is believed that in patients with a pre-existing primary headache disorder, these mechanisms may lead to an increase in pain sensitivity and frequency [16, 19]. However, further research is needed to elucidate the precise mechanisms involved in COVID-19 vaccination-related headaches. Indeed, it is plausible that COVID-19 vaccination may stimulate the immune system [20], resulting in an immune response that could potentially trigger TVS. Activation of immune system cells can lead to the production of proinflammatory cytokines, including prostaglandins and bradykinins. These substances have the potential to induce the release of calcitonin gene-related peptide (CGRP) from neurons in the TVS, which is known to play a role in migraine headaches. This immune-mediated response may contribute to the development of migraine-like headaches following vaccination. However, further research is needed to establish a definitive link between immune system activation, TVS involvement, and vaccine-induced headaches [6, 16]. Also, inactivated COVID-19 vaccines, which often contain aluminum salt-based adjuvants, can modulate and induce an immune response. These adjuvants have the potential to stimulate the immune system and trigger the release of proinflammatory cytokines such as interleukin (IL)-1β and IL-18. These cytokines may play a role in triggering headache symptoms [6, 21, 22].
In this study, we provided evidence that patients with a pre-existing headache, particularly migraine, are more likely to exhibit the migraine-like headache phenotype in cluster 1, while the opposite group demonstrates characteristics resembling tension-type headaches. These findings support the notion of increased TVS hyperexcitability and heightened pain sensitivity in cluster 1. Our results suggest that individuals with a pre-existing migraine condition are more prone to experiencing persistent, resistant, and severe headaches following COVID-19 vaccination, which may require ongoing medical treatment. These patients may not experience headache remission after vaccination. As a result, it is crucial for headache specialists and clinicians to provide specialized care for these individuals in terms of headache management.
Prolonged/worsened COVID-19 vaccination-related headaches as a result of other secondary etiologies
In our study, we encountered a relatively small number of cases (4.6%) with other secondary prolonged or worsened COVID-19 vaccination-related headaches, which limited our ability to draw definitive conclusions. However, it was observed that the majority of other secondary headaches were attributed to cerebral venous thrombosis, accounting for approximately 62.5% of the cases. This suggests that this specific cause may have a significant role in the development of serious secondary headaches following COVID-19 vaccination [3, 7].
Moreover, it is noteworthy that almost all patients (87.5%) with other secondary headache etiologies did not have a pre-existing primary headache condition. This emphasizes the importance of conducting a thorough examination in individuals experiencing new-onset headaches related to COVID-19 vaccination.
Further research with larger consecutive sample sizes is warranted to investigate and gain a better understanding of the association between COVID-19 vaccination and other secondary headache etiologies.
Vaccination-related headaches are not currently classified as a separate entity in the ICHD-3 classification system, despite their widespread recognition [12, 17]. Clinicians and researchers currently utilize the code "Headache attributed to the use of or exposure to a substance" (8.1) to categorize vaccination-related headaches. However, we believe that there is a need for a classification specifically for "COVID-19 vaccination-related headaches" in future versions of the ICHD classification system. This inclusion would be beneficial in recognizing the distinct phenotypes of these prolonged or worsened headaches and increasing awareness among clinicians responsible for differentiating and diagnosing these headaches in patients.
Although COVID-19 vaccination can lead to a variety of side-effects, it should be emphasized that “the long COVID phenomenon” itself is a much more serious healthcare problem globally in the long-term course after COVID-19 pandemic. People who recovered from acute COVID-19 might face a wide spectrum of persistent symptoms in the following weeks/months such as insomnia, fatigue, cognitive disturbance (brain fog), myalgia, hair loss, muscle weakness, psychiatric symptoms, and a persistent headache which creates a serious source of disability [23]. In our patients with a COVID-19 history, we also observed that fatigue (68.8%), cognitive impairment (45%) and hair loss (29.1%) was the three major long-COVID-19 symptoms. Hereby, vaccination against COVID-19 serves as a significant weapon against long-COVID-19 phenomenon, in order to prevent these clinical manifestations [24].
Strengths and limitations
Our study possesses several notable strengths. Firstly, it is the first multinational and prospective study to investigate the long-term course of COVID-19 vaccination-related prolonged or worsened headaches. This provides valuable insights into the course of these headaches over time. Additionally, our study demonstrates that COVID-19 vaccination-related headaches exhibit distinct profiles and long-term courses. This highlights the existence of different phenotypes within these patient groups. The identification of these distinct phenotypes has the potential to influence treatment approaches for patients with COVID-19 vaccination-related headaches, allowing for more tailored and effective management strategies.
We acknowledge certain limitations in our study. Firstly, the inclusion of patients from diverse settings such as emergencies and outpatient policlinics introduces heterogeneity to our study group, which may affect the generalizability of our findings. Secondly, the non-consecutive nature of the patients included in the study may introduce selection bias, potentially leading to biased results. Conversely, patients with severe conditions might not be able to accurately express their headache symptoms in an outpatient setting, potentially affecting the completeness of the data. Lastly, Lastly, we were unable to analyze differences between various vaccine types due to the fact that over 75% of our study group had received at least one dose of an mRNA vaccine. Conducting further studies that specifically evaluate patients based on their COVID-19 vaccine types could yield more robust results for addressing this issue.








Comments (0)