
Remember me
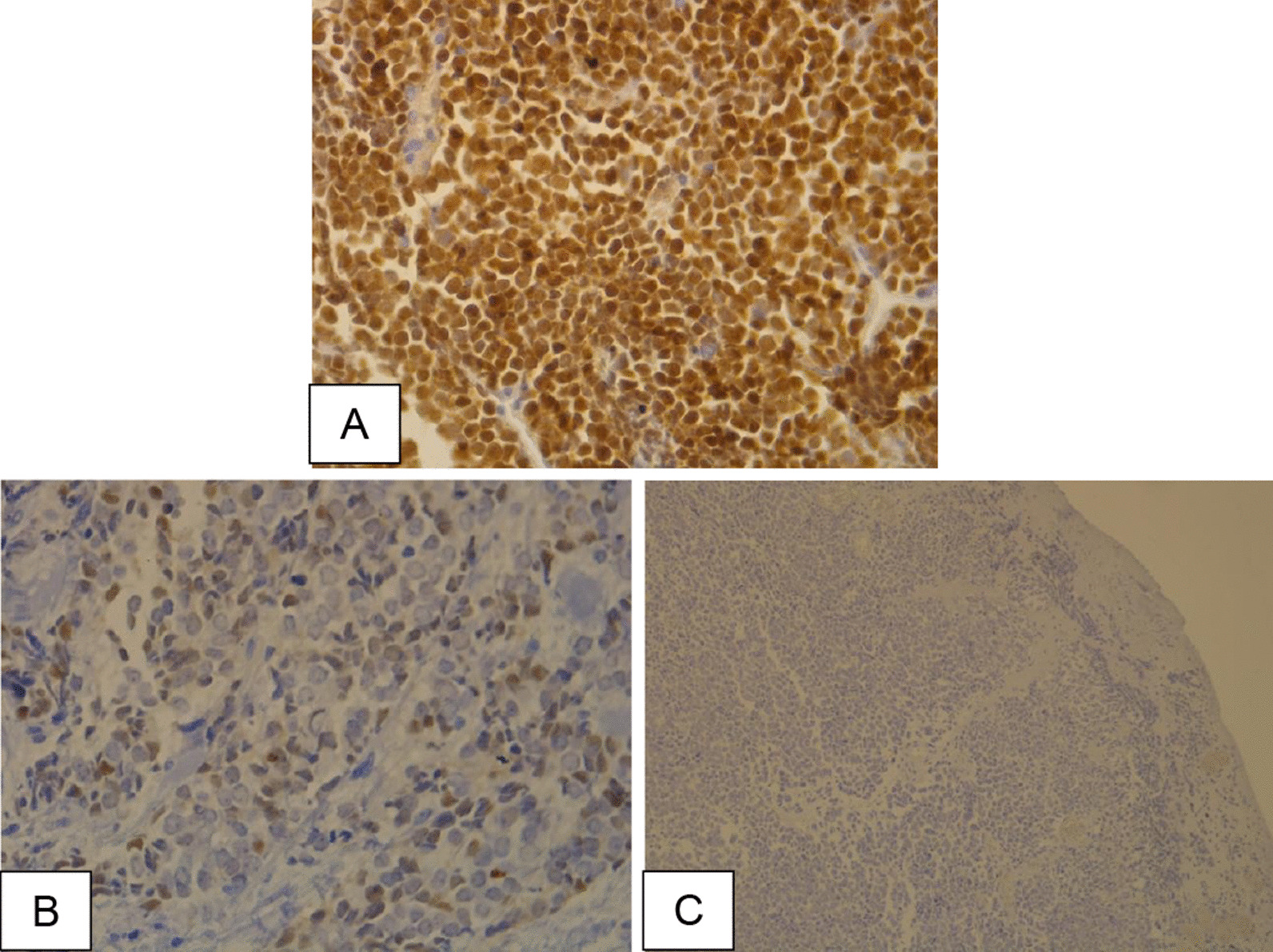
In this cross-sectional study, we utilized sociodemographic and pre-test data that were collected from a convenience sample of 223 women between June and August of 2013 as part of an educational intervention designed to encourage uptake of cervical cancer screening (Fig. 1: Diagram outlining study procedures). Women attending health facilities and at community events in the four parishes of western Jamaica served by Jamaica’s Western Regional Health Authority (WRHA), namely St. James, Westmoreland, Trelawny, and Hanover, were recruited for the study [16]. These parishes provide no-cost Pap tests at hospitals and health centers in the parishes. To be eligible for the study women had to be age 18 years and older and had to have never had a Pap test or had not received a Pap test in the past five years or more. Potential participants were approached by the research team with information about the study. If a woman expressed interest in the study, she was asked “Have you ever had a Pap test?” Women who answered “No” were eligible to participate in the study. Women who answered “Yes” were asked to specify the year in which they last received a Pap test. If the date of the Pap test was five years or greater, they were eligible to participate. Women who received a Pap test in less than five years were excluded from the study.
Fig. 1
Outline of study procedures
Women who met the eligibility criteria were taken through the informed consent process by the research staff and encouraged to ask questions, after which signed informed consent was obtained.
The complete intervention study consisted of: (1) a sociodemographic survey with a pretest that assessed knowledge of (causes, symptoms) and attitudes about cervical cancer and cervical cancer screening; (2) a PowerPoint cervical cancer educational intervention; and (3) a posttest designed to assess changes in knowledge and attitudes about cervical cancer and cervical cancer screening [16]. The study procedures are outlined in Fig. 1. Only the demographic and pre-test data are presented in this paper. Data on the intervention and change in knowledge and attitude from the pretest to the posttest are presented in the manuscript by Coronado Interis et al. [16].
Although these data were collected in 2013, they are still currently relevant since the screening method and screening experience for women in Jamaica have not changed since 2013 [7, 8]. The Pap test is the only screening method that was, and is, available in the public health system. Although the 2020 Ministry of Health and Wellness Screening Guidelines lists HPV testing as a cervical screening method [7], HPV testing has not been implemented in the public health system and screening is still conducted solely by the Pap test, similar to what is stated in the 2011 Ministry of Health Jamaica National Guidelines for Cervical Cancer Prevention and Control [8].
Primary outcome and predictor variablesThe primary outcome of the analyses was previously receiving a Pap test. Predictor variables included sociodemographic characteristics, and knowledge and attitudes about Pap tests.
The following sociodemographic characteristics were analyzed: parish, age, highest education level, employment status, occupation, marital status, number of children, need for childcare, and distance from the nearest clinic. Age was categorized as 18–29, 30–39, 40–49, and 50 years or older. Highest education level was categorized as primary or less, secondary, and college, technical, vocational, or graduate school. Employment status was categorized as unemployed and employed. Occupation was categorized as unskilled worker, and skilled worker/professional/business owner. Marital status was categorized as married, single, cohabitating with partner, and other (divorced, separated, or widowed). Number of children was categorized as 0, 1, and 2 or more. Distance from clinic was categorized as ≤ 30 min and more than 30 min.
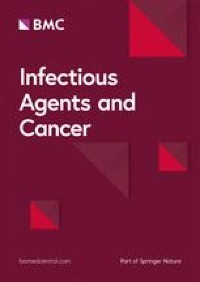
Attitudes included: (1) belief that the Pap test is embarrassing, and (2) belief that the Pap test is painful; responses were categorized as yes, no, or do not know. Additional questions assessed whether the women had heard of cervical cancer, their awareness of screening location and the purpose of the Pap test. Responses to these questions were categorized as yes, no, or do not know. To investigate sources of cervical cancer information, participants were asked whether they had heard of cervical screening from healthcare providers, the media, or other sources such as family, friends, or sexual partners to each of which they answered yes or no.
A knowledge score was constructed by summing correct answers from the 21-item pretest knowledge assessment with possible scores ranging from 0 to 21 (Table 1). The test assessed the following areas: knowledge of how women became infected with the agent that causes cervical cancer, symptoms of cervical cancer, and ways to prevent cervical cancer. After scores were created for all participants, tertiles were generated based on the score distribution and were used to categorize knowledge of cervical cancer as low, medium, and high.
Table 1 Questions used to generate knowledge scoreStatistical analysisTo assess associations between predictor variables and previous Pap test, chi-square tests and Fisher’s exact tests were conducted. A p-value of ≤ 0.05 threshold was used to indicate statistical significance. Crude and adjusted odds ratios and 95% confidence intervals were generated as measures of association for variables significant at the bivariate level and two other variables of interest (heard about screening from healthcare provider and knowledge about cervical cancer) and the outcome of ever having a Pap test. Participants with missing data were included in bivariate analyses but removed from the logistic regression model. All analyses were computed among complete cases and were conducted utilizing Statistical Analysis System (SAS) 9.4 (Cary, North Carolina).
Comments (0)