
Remember me

Despite the best standards of care, recurrent pressure injuries (PIs) remain a challenge for many persons with spinal cord injury (SCI), their caregivers, and their medical team.1 It remains a conundrum why some individuals experience a continuous cycle of recurring PI and require extended periods of hospitalization or skilled nursing facilities, whereas others remain PI-free despite similar lifestyle choices.2 The treatment costs particularly impact the Veterans Health Administration (VHA) because it provides a lifetime of care for veterans with SCI through the VHA Spinal Cord Injuries and Disorders System of Care. The authors previously identified a study cohort of 36,626 veterans with SCI seen over a 5-year period.3 The Paralyzed Veterans of America reported that 26,290 veterans with SCI received Veterans Affairs healthcare in 2021.4 Thus, the VHA cares for approximately 12% of the nearly 300,000 persons with SCI currently living in in the US,5 with more than 70% of these veterans receiving annual care.
The development of even one severe PI has a devastating impact on quality of life,6 often leading to prolonged hospitalization or extended care, further complications, and even death. Stillman et al7 found that community-acquired PIs are among the most common causes of rehospitalization. However, within the increased risk population of all individuals with SCI, there appears to be a subgroup of individuals at even higher risk of not just one but recurrent PIs.
The cost burden of PI is significant,8 particularly for the VHA.9 Over 10 years ago, the direct costs of treating a stage 4 PI exceeded $100,000 per PI.10 Additional indirect costs include the loss of income, productivity, progress toward rehabilitation and vocational goals, independence, self-esteem, and sense of self-worth.11 Pressure injury prevention is estimated to be approximately 2.5 times more economic than PI treatment.12 Currently, pressure relief regimens are prescribed based on standardized thresholds for what is considered to be a “safe duration” of sustained applied pressure. For example, although clinicians agree that regular turning schedules are essential, the basis for selecting a specific schedule is less clear. In many clinical settings, a 2-hour turning regimen has long been considered the criterion standard.13 However, this is rarely achieved, even within the hospital setting.14 Other researchers have found that 4-hour turns may be adequate with appropriate support surfaces.15 The situation is similar for preventing PI development in wheelchair users. Pressure relief every 20 minutes is recommended but rarely rigorously maintained. Continued high PI incidence indicates that these standardized regimens are insufficient for the prevention of recurrent PIs for many individuals.
There are many factors related to PI risk, particularly in persons with SCI. Some wounds seem to appear overnight, a condition known as deep-tissue PI (DTPI). In 2007, the National Pressure Injury Advisory Panel updated the PI staging system to include DTPI as a discrete class of PI. It is important to note that the classification is termed “suspected DTPI,” an indication of the challenges of early DTPI detection. This class of PI starts with damage in the deep tissues near the underlying bone. Standard quantitative tissue health assessment techniques, such as interface pressure mapping and visual skin checks, have a limited relationship with DTPI risk16 because damage is not initiated at the surface. Although modeling studies increase our understanding of the stresses and strain that can cause DTPI,17,18 there are currently no reliable clinical tools for detecting risk of DTPI in standard clinical practice. The reported incidence of DTPI appears to be rising,19 which may be due to increased clinician awareness and hospital polices to track PIs present on admission and hospital-acquired PIs. Deep-tissue PI remains a common clinical challenge in part because there are no reliable methods to identify changes in muscle quality that can influence DTPI development.
Although all persons with SCI are at increased risk of PI development, susceptibility to PI recurrence appears to vary among individuals. There is increased subclinical inflammatory activity following injury,20,21 confirmed by functional genomics,22 which is long suspected to contribute to impaired healing. The authors found that some individuals with SCI experience rapidly increasing intramuscular adipose tissue (IMAT) levels in their gluteal muscle, whereas others maintain stable levels over several years. In previous work using biomarkers for early indicators of PI risk, the authors found that muscle composition, specifically IMAT levels, is significantly different in individuals with a PI history versus those without.23,24 Moreover, IMAT accumulation following SCI varies considerably and is not clearly associated with either level of injury or American Spinal Injury Association Impairment Scale grade. However, the level of injury does appear to be directly associated with the accumulation of visceral and subcutaneous fat in a cohort of individuals with complete SCI.25,26 These findings lend support to the hypothesis that varying rates and levels of IMAT following SCI may be governed by genetics.27 Identifying genetic biomarkers predisposing veterans with SCI to recurrent PIs may enable early interventions to minimize medical morbidity, healthcare costs, and reduced quality of life.
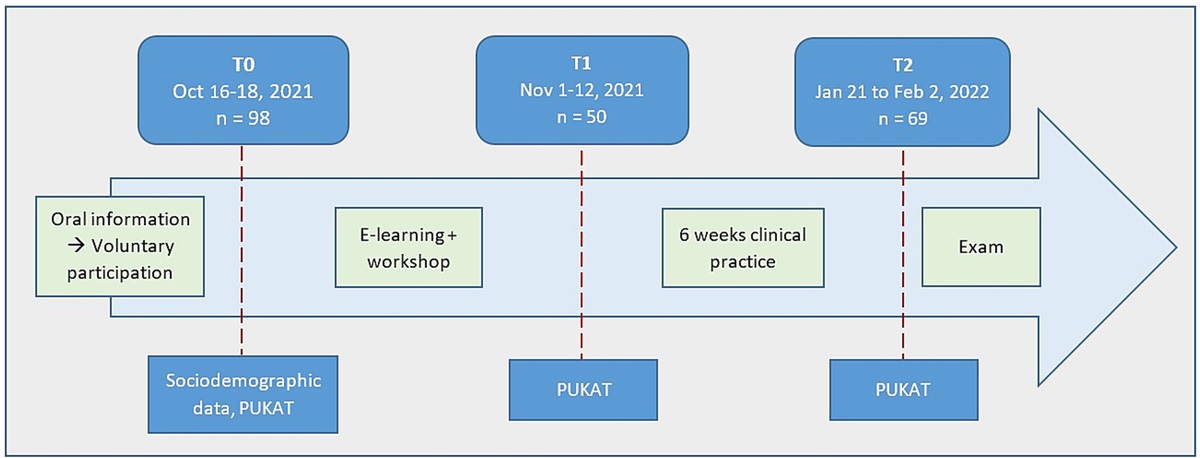
METHODSResearchers sequenced processed whole blood samples to examine the transcriptome profile of veterans with SCI using repeated measures. Study participants were adult veterans with SCI who were recruited from three VHA Spinal Cord Injuries and Disorders Centers. Exclusion criteria included having an open pelvic region PI at time of recruitment or significant active systemic disease at time of enrollment (eg, heart disease, renal failure, uncontrolled diabetes, lupus with neuropathy, sickle cell disease, and symptomatic myasthenia gravis). At intake, researchers obtained a comprehensive profile of clinical and health factors and demographic information relevant to PI history. A medical and social profile relevant to PI risk was collected at enrollment and at each follow-up visit by reviewing patients’ medical charts (Figure 1). Whole blood samples were collected at 6- to 12-month intervals for 2 to 4 years. In addition to DNA profiling with whole genome sequencing (WGS) of the participants, researchers also performed RNA sequencing (RNASEQ) to assess potential genomic markers associated with recurrent PIs.
 Figure 1.:
Figure 1.: COMPREHENSIVE CLINICAL AND MEDICAL PROFILE COLLECTIONAbbreviations: ASIA, American Spinal Injury Association; BMI, body-mass index; SCI, spinal cord injury.
Blood Sample CollectionWhole blood samples were collected for DNA and RNA isolation and subsequent analysis using next-generation sequencing (NGS; Illumina). Samples for DNA analysis were collected in Vacuette K2EDTA (Greiner-BioOne) blood collection tubes and frozen immediately at −80 °C for further analysis. Samples for RNA analysis were collected in PaxGene tubes (Qiagen), left at room temperature for 2 hours, and frozen at −80 °C for further analysis. Samples collected from additional study sites were shipped via Saf-T-Pak (Inmark Life Sciences) on dry ice, immediately intercepted at the warehouse, and frozen at −80 °C until further analysis.
DNA and RNA IsolationLaboratory technicians extracted DNA from whole blood samples using the MagMAX DNA multi-sample kit (Applied Biosystems) following the DNA extraction protocol provided in each kit. Immediately following completion of the DNA isolation, sample concentration was determined using fluorometric quantification (Qubit; Fisher Scientific). Samples were sent to Case Western Reserve Genomics Core for NGS.
RNA was extracted from whole blood samples using the PaxGene Blood RNA Kit (Qiagen) following the RNA extraction protocol provided in each kit. Immediately following completion of the RNA isolation and sample concentration, quality control was carried out using fluorometric quantification (Qubit; Fisher Scientific). The RNA integrity number was determined using the Qubit RNA broad range kit and normalized to 50 ng/μL prior to sequencing using the NovaSeq 6000 (Illumina) system.28
DNA and RNA SequencingBlood samples from the study cohort underwent WGS using NGS (Illumina) by the Genetics Core Facility at Case Western Reserve University. Sample sequences were compared against the human reference genome hg38, and single-nucleotide polymorphisms were identified using the Genomic Analysis Toolkit (Broad Institute) germline mutation pipeline. Variants were filtered based on allele frequencies in the general population (<5% in gnomAD and 1000 Genomes Project), as well as multiple variant effect predictors including Combined Annotation Dependent Depletion, PolyPhen, Sorting Intolerant from Tolerant, and Mutation Assessor. Candidate genes harboring variants of interest were selected based on gene function.
The RNASEQ data were aligned to the human reference genome using STAR aligner. Gene expression and differential expression analyses were performed using Cufflinks with the GENCODE annotation for hg38. Expression data were reported in FPKM (fragments per kilobase million), and differential genes were defined using a false discovery cutoff of 5% (P < .05). Enrichment analysis and pathway analysis were examined using iPathwayGuide (AdvaitaBio).
RESULTSParticipant demographics and clinical characteristics are summarized in the Table.
Table. - STUDY COHORT DEMOGRAPHICS AND PI HISTORY Variable n (%) Sex Male 75 (96.2) Female 3 (3.8) Race Caucasian 62 (80) African American 15 (19) Other 1 (1) Neurological involvement Above T6 56 (72) Below T6 22 (28) AIS Grade Complete (AIS A) 24 (31) Incomplete (AIS B, C, D) 54 (69) History of PI Yes 29 (37) No 49 (63) Variable Median (Range) Duration of injury 9 y (1 mo to 50 y) Age at enrollment 62 y (22 to 82y)Abbreviations: AIS, American Spinal Injury Association Impairment Scale; PI, pressure injury.
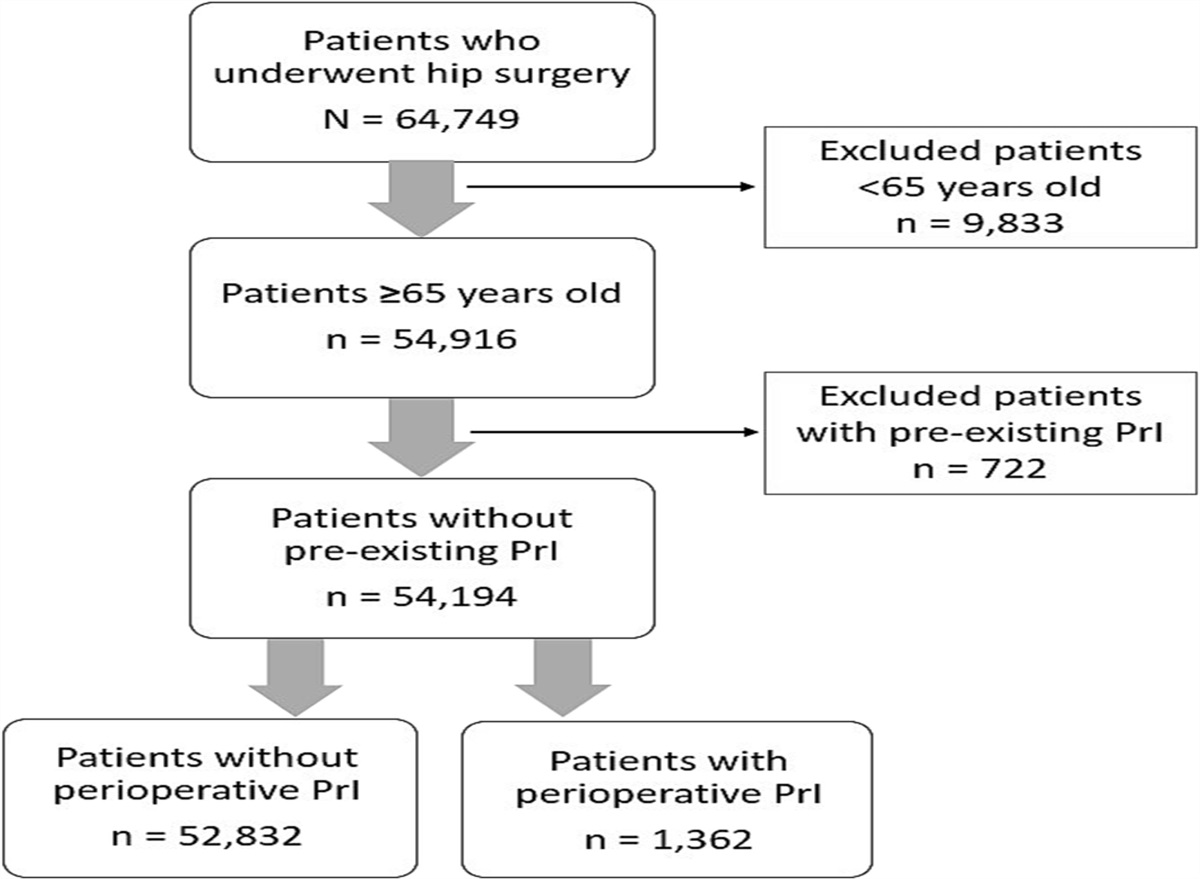
Initial WGS analysis identified 513 genes that showed increased prevalence of single-nucleotide variations in exonic regions with high (>20) combined annotation-dependent depletion scores between persons with high versus low IMAT levels. When cross-referenced with persons who had recurrent PIs, 260 genes met the criteria for inclusion. Gene set enrichment analysis using Hallmark and KEGG (Kyoto Encyclopedia of Genes and Genomes) gene sets of these candidate genes revealed enrichment in genes encoding proteins involved in fatty acid metabolism (P < .01; Figure 2).
 Figure 2.:
Figure 2.: DISTRIBUTION OF ENRICHED GENES DIFFERS WITH DIFFERENT IMAT LEVELS AND RECURRENT PIAbbreviations: IMAT, intramuscular adipose tissue; PI, pressure injury.
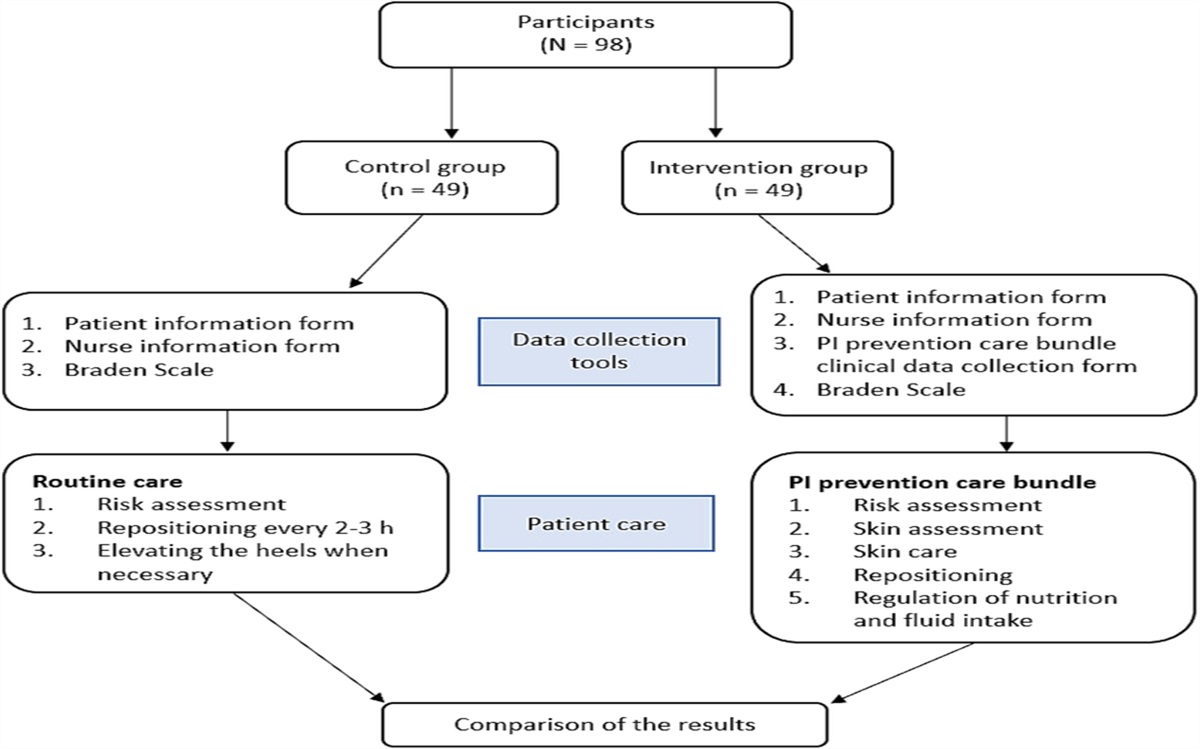
Analysis of the RNASEQ data revealed differences in gene expression between persons with and without recurrent PIs (Figure 3). Researchers identified a robust subset of 25 active genes that are differentially upregulated or downregulated between persons with versus without recurrent PIs. Pathway analysis indicated that persons with recurrent PIs have upregulated activity in genes involved in the metabolic pathways (ENOSF1) and pathways in biological senescence (TMEM158) and downregulated activity in the interleukin 17 signaling pathway directly involved in antimicrobial protection in vivo. In comparison, persons without recurrent PIs have upregulated activity in genes related to bioprocesses such as regulators of vasodilation (TAC3) and downregulated activity in biological pathways related to addiction (FOS, JUN, FOSB).
 Figure 3.:
Figure 3.: HEATMAP SHOWING DIFFERENTIALLY EXPRESSED GENES IN PERSONS WITH AND WITHOUT RECURRENT PRESSURE INJURIESAbbreviation: PrI, pressure injury.
DISCUSSIONGenomic profiles may reveal why some individuals with SCI are predisposed to increased IMAT and resultant recurrent PI risk. This preliminary work has shown the effect of candidate single-nucleotide variants on IMAT accumulation and recurrent PI risk. The authors have previously shown that varying levels of circulatory biomarkers, including FABP4 and FABP3, may be indicative of recurrent PI risk.24,29–31 Further, genetic biomarkers, specifically those related to fatty metabolism, may indicate which persons with SCI are at highest risk of recurrent PIs.32
The gene ENOSF1 is found in the metabolic pathway and is linked specifically to carbohydrate and glucose metabolism.33 In individuals with recurrent PIs, ENOSF1 was upregulated, denoting increased sensitivity to carbohydrates and glucose. Evidence indicates that impaired blood sugar regulation and high levels of circulatory glucose can lead to poor wound healing.34 However, metabolic regulation was not the only biological process observed in the present work: Genes associated with biological senescence, addiction, and vasodilation were also expressed. Although cellular and molecular definitions of aging continue to be debated, aging is a significant risk factor for chronic disease resulting from genomic damage, epigenetic alterations, and impairments to intercell communications.35 Specifically, TMEM158 is a relevant marker of senescence in studies of cancer and age-related muscle function decline (sarcopenia).36 Thus, further examination of the link between increased IMAT and upregulated TMEM158 is needed, particularly as it relates to individuals with recurrent PIs and aging with SCI.
In those without recurrent PIs, an upregulation of TAC3, which serves as a ligand for neurokinin B, may serve as a protective factor. Among the many functions of neurokinin B, vasodilation for BP regulation holds the most relevance for individuals with SCI. Dysregulation of the autonomic nervous system and vascular complications including arterial hypotension, deep vein thrombosis, and coronary artery disease are common sequela following SCI.37 Further, TAC3 upregulation in these individuals suggests improved control of vascular perfusion compared with persons with SCI who experience recurrent PIs. Upregulation of neurotransmitters and receptors that regulate cardiovascular function may provide a target for treatment to improve blood flow and, in turn, wound bed perfusion for those with recurrent PIs. One pathway that appears to interact with the TAC3 gene is the dopamine pathway.38 The dopaminergic pathway also serves as the receptor sites of several drugs used to treat cardiovascular disease, as well as neurologic (ie, addiction, sleep) and physiologic (cellular communication) functions.39,40 Thus, future studies should examine gene-gene and gene-environment interactions and how these influence PI development and the relationships among other secondary health conditions that co-occur in veterans with SCI.
Veterans with SCI experience different postinjury functional independence and quality-of-life changes as a result of their individual medical conditions. In addition to differences in injury and medical sequela characteristics, veterans with SCI differ by age, care support, environment, and other social determinants of health that can influence the diversity of clinical presentation. Clinical phenotypes can be described as identifiable manifestations of disease, such as measurable biological, behavioral, and clinical markers of a condition or disease.41,42 Identifying clinical phenotypes offers opportunities to recognize, predict, and prevent disease progression and estimate healthcare utilization. Phenotyping heterogeneous populations, such as persons with chronic SCI, is complex and challenging to undertake in standard research studies or the clinical point-of-care setting.43 However, in the present study, the authors used computational phenotyping to derive research-grade phenotypes from clinical data using computer-executable algorithms applied to the complete electronic health records of a moderate population of veterans with SCI.42,44 By undertaking complete genotypic profiling, they were able to discover interactions between the genetic background and impact of SCI on the phenotypic occurrence of recurrent PIs.
Implications for PracticeThe negative impact of recurrent PIs on quality of life is profound, and although the pipeline for translation of research to practice is improving, significant barriers to the prevention of recurrent PIs remain. However, by applying 21st-century approaches to this age-old problem, we better understand the potential for using genomic biomarkers to identify increased risk of recurrent PIs. In addition, understanding the role of the environment and social determinants of health on healthcare outcomes leads researchers to an increased appreciation for the likely importance of elucidating the influence of epigenetics on complex disease and phenotypic diversity in recurrent PI. These study findings may impact individualized care planning within 5 years. Precision drug discovery and development are likely to be facilitated,45 and novel pharmaceutical clinical trials could be expected within 10 to 15 years.
CONCLUSIONSUtilizing enhanced personalized risk assessments for persons with SCI may improve health status and quality of life for this patient population while reducing associated costs. The genetic signatures for recurrent PIs identified in this work may also apply to the management of other populations at high risk of PI development. The dopaminergic pathway holds promise as a shared pathway between PI and other secondary health complications of interest, given dopamine’s involvement with movement, memory, attention, sleep regulation, and multiple addiction pathways. Comprehensive electronic health records include clinical records of physical characteristics and laboratory data, as well as potential phenotypic features for homogeneous grouping, and may be leveraged to further address complex interactive health issues such as recurrent PIs and depression in individuals with SCI.
An ongoing multisite repeated-measures study is providing further insights into multi-omic risk of recurrent PIs. External validation of the biomarkers for early PI risk model with a study cohort of 100 persons with SCI will establish the role of genomic and epigenomic factors in the development of recurrent PIs and other comorbid conditions. Within the next 10 years, these validated biomarkers may also provide the basis for rapid point-of-care blood testing to identify individuals at increased risk of recurrent PIs and permit healthcare systems to provide advanced interventions before initial skin breakdown occurs based on their genomic profile.
REFERENCES 1. Ho CH, Bogie K. The prevention and treatment of pressure ulcers. Phys Med Rehabil Clin N Am 2007;18(2):235–53. 2. Guihan M, Richardson MSA. The problem of preventing pressure ulcers in people with spinal cord injury. J Spinal Cord Med 2019;42(6):681–4. 3. Bogie KM, Roggenkamp SK, Zeng N, et al. Development of predictive informatics tool using electronic health records to inform personalized evidence-based pressure injury management for veterans with spinal cord injury. Mil Med 2021;186(Suppl 1):651–8. 5. National Spinal Cord Injury Statistical Center. Traumatic Spinal Cord Injury Facts and Figures at a Glance. Birmingham, AL: University of Alabama at Birmingham; 2022. 6. Gilmer T. Lessons Learned from My Flap Surgery Journey. New Mobility, May 2018. https://newmobility.com/flap-surgery-journey/. Last accessed July 12, 2023. 7. Stillman MD, Barber J, Burns S, et al. Complications of spinal cord injury over the first year after discharge from inpatient rehabilitation. Arch Phys Med Rehabil 2017;98(9):1800–5. 8. Phillips CJ, Humphreys I, Fletcher J, et al. Estimating the costs associated with the management of patients with chronic wounds using linked routine data. Int Wound J 2016;13(6):1193–7. 9. Stroupe KT, Manheim L, Evans CT, et al. Cost of treating pressure ulcers for veterans with spinal cord injury. Top Spinal Cord Inj Rehabil 2011;16(4):62–73. 10. Brem H, Maggi J, Nierman D, et al. High cost of stage IV pressure ulcers. Am J Surg 2010;200(4):473–7. 11. LaMantia JG, Hirschwald JF, Goodman CL, et al. Pressure sore readmission program: a method to reduce chronic readmissions for pressure sore problems. Rehabil Nurs 1987;12:22–5. 12. Lyder CH, Wang Y, Metersky M, et al. Hospital-acquired pressure ulcers: results from the national Medicare Patient Safety Monitoring System study. J Am Geriatr Soc 2012;60(9):1603–8. 13. Norton D, McLaren R, Exton-Smith A. An Investigation of Geriatric Nurse Problems In Hospitals. Edinburgh, UK: Churchill Livingston; 1975. 14. Krishnagopalan S, Johnson EW, Low LL, et al. Body positioning of intensive care patients: clinical practice versus standards. Crit Care Med 2002;30:2588–92. 15. Yap TL, Horn SD, Sharkey PD, et al. Effect of varying repositioning frequency on pressure injury prevention in nursing home residents: TEAM-UP trial results. Adv Skin Wound Care 2022;35(6):315–25. 16. Gefen A, Levine J. The false premise in measuring body-support interface pressures for preventing serious pressure ulcers. J Med Eng Technol 2007;31(5):375–80. 17. Linder-Ganz E, Gefen A. Stress analyses coupled with damage laws to determine biomechanical risk factors for deep tissue injury during sitting. J Biomech Eng 2009;131(1):011003. 18. Stekelenburg A, Gawlitta D, Bader DL, et al. Deep tissue injury: how deep is our understanding? Arch Phys Med Rehabil 2008;89(7):1410–3. 19. Verschueren JH, Post MW, de Groot S, et al. Occurrence and predictors of pressure ulcers during primary in-patient spinal cord injury rehabilitation. Spinal Cord 2011;49(1):106–12. 20. Morse LR, Stolzmann K, Nguyen HP, et al. Association between mobility mode and C-reactive protein levels in men with chronic spinal cord injury. Arch Phys Med Rehabil 2008;89(4):726–31. 21. Radulovic M, Bauman WA, Wecht JM, et al. Biomarkers of inflammation in persons with chronic tetraplegia. J Breath Res 2015;9(3):036001. 22. Herman P, Stein A, Gibbs K, Korsunsky I, Gregersen P, Bloom O. Persons with chronic spinal cord injury have decreased natural killer cell and increased Toll-like receptor/inflammatory gene expression. J Neurotrauma 2018;35(15):1819–29. 23. Lemmer DP, Alvarado N, Henzel K, et al. What lies beneath: why some pressure injuries may be unpreventable for individuals with spinal cord injury. Arch Phys Med Rehabil 2019;100(6):1042–9. 24. Bogie KM, Schwartz K, Li Y, Wang S, Dai W, Sun J. Exploring adipogenic and myogenic circulatory biomarkers of recurrent pressure injury risk for persons with spinal cord injury. J Circ Biomark 2020;9:1–7. 25. Farkas GJ, Gorgey AS, et al. The influence of level of spinal cord injury on adipose tissue & its relationship to inflammatory adipokines & cardiometabolic profiles. J Spinal Cord Med 2018;41(4):407–15. 26. Gorgey AS, Ennasr AN, Farkas GJ, Gater DR Jr. Anthropometric prediction of visceral adiposity in persons with spinal cord injury. Top Spinal Cord Inj Rehabil 2021;27(1):23–35. 27. Schleinitz D, Böttcher Y, Blüher M, et al. The genetics of fat distribution. Diabetologia 2014;57(7):1276–86. 28. Modi A, Vai S, Caramelli D, Lari M. The Illumina sequencing protocol and the NovaSeq 6000 system. Methods Mol Biol 2021;2242:15–42. 29. Schwartz K, Henzel MK, Richmond MA, et al., Biomarkers for recurrent pressure injury risk in persons with spinal cord injury. J Spinal Cord Med 2020;43(5):696–703. 30. Bogie K, Henzel MK, Richmond MA, Alvarado N. Tissue health biomarkers to predict highest risk individuals for pressure injury recurrence. Arch Phys Med Rehabil 2018;99(10):e13. 31. Bogie K, Henzel MK, Richmond M, et al. What lies beneath: tissue biomarkers indicate why pressure mapping alone cannot tell the whole story. Proc AAWC Annual Pressure Ulcer Summit. Ostomy Wound Manage 2018;64(4). 32. Bogie KM, Schwartz K, Henzel MK, et al. Genomic biomarkers for recurrent pressure injury risk in persons with spinal cord injury. Presented at the American Spinal Injuries Association 2022 Annual Scientific Meeting; New Orleans, Louisiana; May 2022. 33. Dashty M. A quick look at biochemistry: carbohydrate metabolism. Clin Biochem 2013;46(15):1339–52. 34. Feng J, Wang J, Wang Y, et al. Oxidative stress and lipid peroxidation: prospective associations between ferroptosis and delayed wound healing in diabetic ulcers. Front Cell Dev Biol 2022;10:898657. 35. Schmeer C, Kretz A, Wengerodt D, Stojiljkovic M, Witte OW. Dissecting aging and senescence—current concepts and open lessons. Cells 2019;8(11):1446. 36. Solovyeva EM, Ibebunjo C, Utzinger S, et al. New insights into molecular changes in skeletal muscle aging and disease: differential alternative splicing and senescence. Mech Ageing Dev 2021;197:111510. 37. Venturelli M, Amann M, Trinity JD, Ives SJ, Richardson RS. Spinal cord injury and vascular function: evidence from diameter-matched vessels. J Appl Physiol (1985) 2021;130(3):562–70. 38. Klein MO, Battagello DS, Cardoso AR, et al. Dopamine: functions, signaling, and association with neurological diseases. Cell Mol Neurobiol 2019;39(1):31–59. 39. Redenšek S, Flisar D, Kojović M, et al. Genetic variability of inflammation and oxidative stress genes does not play a major role in the occurrence of adverse events of dopaminergic treatment in Parkinson's disease. J Neuroinflammation 2019;16(1):50. 40. Zhang Z, Wen H, Li Y, et al. TAC3 Gene products regulate brain and digestive system gene expression in the spotted sea bass (Lateolabrax maculatus). Front Endocrinol (Lausanne) 2019;10:556. 41. Ahmed W, Brinkman P, Fowler S. Chapter 20: Clinical phenotyping. In: Beauchamp J, Davis C, Pleil J, eds. Breathborne Biomarkers and the Human Volatilome. 2nd ed. Elsevier; 2020:321–34. 42. Richesson RL, Sun J, Pathak J, Kho AN, Denny JC. Clinical phenotyping in selected national networks: demonstrating the need for high-throughput, portable, and computational methods. Artif Intell Med 2016;71:57–61. 43. Bastarache L, Denny JC, Roden DM. Phenome-wide association studies. JAMA 2022;327(1):75–6. 44. Pugh MJ, Kennedy E, Prager EM, et al. Phenotyping the spectrum of traumatic brain injury: a review and pathway to standardization. J Neurotrauma 2021;38(23):3222–34. 45. NASEM Forum on Drug Discovery, Development, and Translation. Enabling Precision Medicine: The Role of Genetics in Clinical Drug Development. Washington, DC: NA Press; 2017.
Comments (0)