
Remember me



What is already known
Practicing hand hygiene is an excellent way to decrease the rate of central line-associated bloodstream infections (CLABSI) in patients with central venous access devices (CVAD). Although subclavian vein catheterization presents a relatively low risk of bloodstream infection associated with nontunnelled CVADs, the risk of pneumothorax is higher with subclavian venous catheters than with jugular or femoral venous catheters. Using an officially approved chlorhexidine-impregnated dressing significantly reduces the rate of CLABSI; however, benefits are only obtained with short-term nontunnelled CVADs.What this paper adds
The use of an evidence-based education program ensured the competence of healthcare professionals in performing CVAD insertions and caring for patients with CVAD, which contributed to the success of this project. Multiple strategies should be implemented to effectively decrease the rate of CLABSI. Leadership and team resource management, education and monitoring, and innovative activities are the key factors in the successful decrease in CLABSI. IntroductionA central venous access device (CVAD) is an intravascular catheter that terminates at or close to the right atrium or in great vessels, such as the superior vena cava, inferior vena cava, internal jugular veins, subclavian veins, and femoral veins. CVADs are used for providing nutrition, drawing blood, and performing infusion and hemodynamic monitoring.1 However, central venous catheterization poses a significant risk of infection by creating conditions not only for microorganisms to enter the bloodstream from the skin at the insertion site but also for microbes to colonize the extraluminal surface at the insertion site.2 The rate of central line-associated bloodstream infection (CLABSI) varies widely in different situations, ranging from 1.25 to 40 bloodstream infections (BSIs)/1000 CVAD-days.3
Effects of bundle care for central venous access deviceThe components of CVAD bundle care include performing hand hygiene, selecting the insertion site, and cleaning the skin prior to insertion.4 In addition, maximum sterile barrier precautions must be taken, and aseptic techniques must be used throughout the entire insertion procedure. Bundle care can decrease the rate of CLABSI by 38% (estimated rate from 2.722 to 1.694).5 The major risk factors for CLABSI include prolonged intensive care unit (ICU) stay and longer catheterization.6 CLABSI affects rates of morbidity, mortality, multidrug resistance (up to nearly 60%) 7 and healthcare costs.8 Based on the data from National Health Insurance Research Database and the Taiwan Nosocomial Infections Surveillance (2007–2015), cases of ICU-acquired bloodstream infection had prolonged hospitalizations by up to 18 days and increased the risk of mortality to 11%.9 The rate of CVAD utilization is 58% and the average density of CLABSI is 4.1 BSIs/1000 CVAD-days in medical centers in Taiwan.10
Evidence from JBI's database about central venous access device insertionsClinical guidelines recommend that skin disinfectants be allowed to dry before CVAD insertion.11 Completion of physical assessment of a patient and taking the patient's history of previous CVAD placement are recommended, after which the insertion of a CVAD should be conducted by competent health professionals.12 Recommended common sites for catheter insertion include the subclavian, internal jugular, and femoral veins, the first of which is preferred because it has been shown to minimize the risk of infection associated with the placement of a nontunnelled CVAD.6 Maximum sterile barrier precautions must be taken and an aseptic technique must be used throughout the entire insertion procedure.11,12
Evidence from JBI database about central venous access device dressings and securement dressingsA systematic review and meta-analysis conducted on adults indicated that the CVAD insertion site should be covered with a sterile dressing or securement dressing.13,14 Commonly used CVAD securement dressings include a sterile, transparent, semi-permeable polyurethane dressing, and a chlorhexidine-impregnated dressing.13 Officially approved chlorhexidine-impregnated dressings have proven helpful for wound care when applied at the catheter insertion site,14,15 and effective at reducing CLABSI in adults when applied to the catheter site for short-term, nontunnelled CVAD.16 Transparent dressings should be replaced every seven days for short-term CVAD. A sterile gauze dressing is recommended for bleeding or oozing around the site. These should be replaced if they are damp, loosened, or visibly soiled. The frequency with which the dressings are changed does not significantly affect the rate of CLABSI11; however, the catheter insertion site should be inspected regularly, either by changing the dressing or by palpation of the intact dressing. If the site is infected, the dressing should be removed.16
The urgent need for change in our central venous access device careThis project was conducted in an urban medical ICU at a tertiary referral center. This ICU qualifies for chemotherapy. Thus, patients in our ICU were the most vulnerable and immunocompromised.
From January to June 2021, the rate of CVAD use was 63.28% (1791 inpatient CVAD-days/2830 inpatient-days) in our ICU. Among the 1791 inpatient CVAD utilization days, there were 15 BSIs, with an incidence of 8.38 BSIs per 1000 inpatient CVAD utilization days. This is higher than that of other medical centers in Taiwan (i.e., 4.1 BSIs per 1000 inpatient CVAD utilization days). Thus, there is an urgent need to improve these conditions.
JBI's evidence recommends standard care for CVAD insertion, dressings, and securements. Our project implemented the JBI recommendations and our institute's policy on CVAD care. Through the JBI audit and feedback method, we aimed to improve staff competence in CVAD care.
ObjectivesThis project aimed to reduce the incidence of CLABSI and improve the outcomes for ICU patients. We plan to use the evidence implementation project to conduct an audit of CVAD care among physicians and nurses to ensure the competence of healthcare professionals in CVAD care based on the JBI evidence summary.
The objectives of the project were:
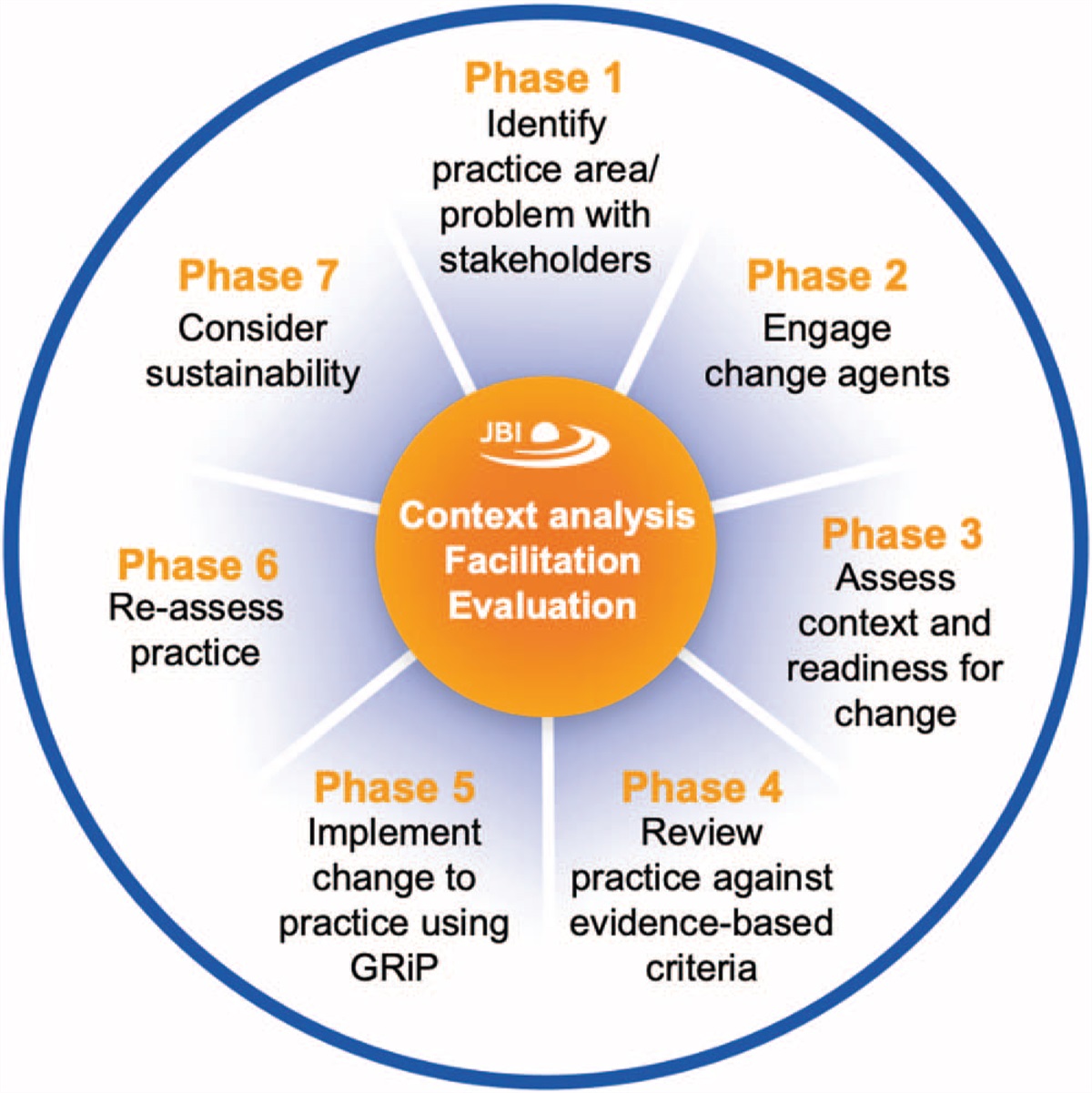
1. To assess the competence of healthcare professionals in CVAD care. 2. To implement strategies for the improvement of competence and to establish sufficient appropriate resources. 3. To evaluate the success of the implementation of the best practices. MethodsThe project methods were based on audit and feedback following the JBI evidence implementation framework's seven phases and the JBI Model for Evidence-based Healthcare (EBHC) to decrease the rate of CLABSI in medical ICU. The JBI Practical Application of Clinical Evidence System (PACES) and Getting Research into Practice (GRiP) were used to assist with data collection, data analysis, and implementation planning.
SampleThis best evidence implementation project was conducted from July 1, 2021 to August 31, 2021, and completed on January 31, 2022. Thirty-two registered nurses and five resident physicians examined their knowledge of central venous catheter (CVC) care and insertion. The CVC insertion skills of the five resident physicians were audited using a checklist, and 20 registered nurses’ CVC care skills were also audited using a checklist. The CLABSI rate was audited monthly for baseline and follow-up audits.
Preplanning Phase 1: Identification of practice area for changeThis project was undertaken in the medical ICU of a tertiary medical center in southern Taiwan. There were 16 beds in the ICU, with 38 nurses with an average working experience of five years. Approximately 45 patients/month are admitted with medical conditions such as respiratory failure or septic shock. The majority of these patients were aged ≥65 years and fragile. The incidence of CLABSI in our ICU was 8.38 BSIs per 1000 inpatient CVAD utilization days before project implantation. We hoped to decrease the CLABSI rate and improve patient outcomes.
Phase 2: Engaging change agentsWe established a project team comprising one senior nurse, one head nurse, one infection control nurse, three nurse practitioners, one attending physician, and one nursing faculty member. The team leader was a nursing faculty member whose primary tasks were building the team and identifying the stakeholders, approaching the hospital administrator for funding, and coordinating and advising on the implementation of all aspects of the project. The team members were responsible for data collection and strategy implementation. In this project, nurses and physicians working in the ICU were selected as the participants. Thirty-two nurses and five physicians participated in the baseline and follow-up audits.
Phase 3: Assessment of context and readiness to changeWe completed a survey as part of a routine audit of the CLABSI between January and June 2021. The usage rate of CVADs was 63.28% in our ICU. The incidence of CLABSI was 8.38 BSIs/1000 CVAD-days, which was higher than that in other ICUs of our hospital (6.00) and in other national medical centers (4.1) in 2020.
Baseline assessment and implementation planning Phase 4: Review of practice against evidence-based audit criteriaThe implementation of improvement strategies was based on the JBI database of CVAD insertion, dressings, and securement dressings. According to the audit criteria developed by JBI PACES, the 11 key criteria were divided into two categories (insertion and dressing, and catheter securement) (Table 1).
Table 1 - Audit criteria, sample, and method of evaluating the compliance and competence for CVC care Audit criterion Participant (P) (times of execution) Methods used to measure the compliance with best practice Insertion 1. A physical assessment of the patient is performed prior to catheter insertion. • P: PhysicianThe JBI PACES program was used by team members to conduct baseline audits. The team members interviewed nurses and residents to identify potential barriers to performance. The five barriers included knowledge of CVC insertion and dressing insufficient for both physicians and nurses; no standardization of CVC insertion performance by the resident physician; lack of team resource management for early CVC removal; lack of cart with CVC insertion and care equipment; and handwashing faucets were too old to be accessible, and there was no timer for sufficient hand washing time.
Based on evidence-based audit criteria, three validated instruments for monitoring performance were used to evaluate the competence of physicians in CVC insertion and nurses in CVC care. Different team members (one physician and one infection control nurse) engaged with their responsibilities, and discussions were held using the PACE framework.
The project team designed three instruments to monitor changes in the knowledge and skills of physicians and nurses. The CVAD care knowledge package and CVAD care devices were developed according to JBI criteria and hospital standards. Three CVAD care knowledge packages were developed. First, 15-item guidelines for providing CVAD care, consisting of 10 items from JBI and five items from the hospital's policy, were used to assess the knowledge of CVAD care (K1–K15 in Fig. 1). A “Pass” mark was given if over 80% of all participants were aware of each item, and a “Fail” mark was given otherwise. The second monitoring instrument was a checklist consisting of 11 steps in the CVAD insertion procedure, to be followed by physicians. It was constructed using a combination of JBI criteria and hospital standards for CVAD insertion (I1–I11). Finally, a 7-step checklist was designed for nurses who provided CVAD care, based on the criteria established by JBI for applying dressings and securing catheters in place (D1–D7). The responses to the second and third checklists were designated as binary variables (“Yes” or “No”). A “Pass” mark was given to each group only if 100% of relevant participants answered correctly. To validate the instruments, five experts (two critical care physicians, one infectious disease physician, one infection control nurse, and one medical ICU head nurse) validated the checklists by evaluating the instruments for clarity of wording, the relevance of each item to the construct being examined, and appropriateness for physicians, nurses, and patients. The average scores for the checklist assessing knowledge of CVAD care, CVAD insertion procedures, and CVAD dressings and securing were 3.76, 3.78, and 3.84, respectively. The content validity index (CVI) for each instrument item was 1, indicating good agreement with the content.
 Figure 1:
Figure 1: Compliance with best practice for knowledge of CVAD care among physicians and nurses at baseline and follow-up according to JBI guidelines and hospital policies. CVAD, central venous access devices.
Impact evaluation and sustainability Phase 6: Re-assessment of practice using a follow-up auditA follow-up audit was performed from December 1, 2021 to January 31, 2022. The project was conducted in accordance with the guidelines set out by JBI PACES.
Phase 7: Consideration of the sustainability of practice changesThe project team consisted of doctors, nurse practitioners, a head nurse, and nurses. We established consensus among the staff regarding early CVC removal. We conducted the CVC care workshop at annual doctor and nurse training programs. Innovative ideas, such as the CVAD dressing cart, are routinely applied in daily care in our unit. CLABSI monitoring was routinely performed at the hospital for infection control. We expect plans to sustain these practical changes.
AnalysisData on changes in compliance were measured using descriptive statistics embedded in JBI PACES in the form of percentage changes from baseline. The data for the audit criteria from the hospital policy were analyzed using Microsoft Excel.
EthicsThis study adhered to the principles of the Declaration of Helsinki. This study was approved by the Human Research and Ethics Committee of National Cheng Kung University Hospital (IRB no.: A-ER-110-351). All the participants provided written informed consent.
Results Baseline assessment and implementation planning 1. The 15-item checklist was used to evaluate the performance of the 37 health care providers, both physicians and nurses, in Phase 4 (43 RN and 5 physicians). The baseline audit revealed that the rate of correct knowledge on the following items was lower than 80%, including: K4, K6, K8, K9, K10, K13, K14, and K15. After the strategies were developed and implemented, the rate of correct CVAD care knowledge assessed with the follow-up audit increased for all items except K1 and K6. However, K8, K10, K13, and K15 remained below 80% (Fig. 1). 2. Evaluation of physicians’ CVAD insertion skills and nurses’ CVAD care skills. To assess the knowledge or physicians and nurses to provide adequate CVAD care, the JBI guidelines propose 11 items. The first six items are related to CVAD insertion and are aimed at physicians, whereas the other five are designed to evaluate nurses’ knowledge of CVAD care skills. Furthermore, the physicians simply asked the nurses about the medical history of the patients, rather than doing so themselves. Regarding the skills required by the physicians, the baseline audit revealed that the rate of compliance with the proposed procedural steps was only 50% for items I2 and item I5. However, the follow-up audit showed that the strategies were successfully implemented, with the compliance rate for all items improving, and four items achieving 100% compliance. There was less improvement for I2 (57.4%), but item I5 improved to 85.71% (Fig. 2). Figure 2:
Figure 2: Compliance with best practice for CVAD insertion skills by physicians at baseline and follow-up according to JBI guidelines. CVAD, central venous access devices.
In terms of the skills that are essential for taking care of CVAD, both physicians and nurses were evaluated. Based on the standards set out in the hospital policy (Fig. 3), the baseline audit revealed a poor compliance rate by physicians for items I8 and I10. Nurses failed to comply with the disinfection process of CVC care (compliance rate for item D6 was 89.39%), and physicians failed to comply with the aseptic process during the CVC insertion procedure (compliance rate for I11 was only 70%). After the strategies were implemented, the compliance rate for almost all the items reached 100%. Item D6 improved to 95.56%, and item I11 was 85.71% (Fig. 3).
 Figure 3:
Figure 3: Compliance with best practice for CVAD care by physicians and nurses at baseline and follow-up according to hospital policies. CVAD, central venous access devices.
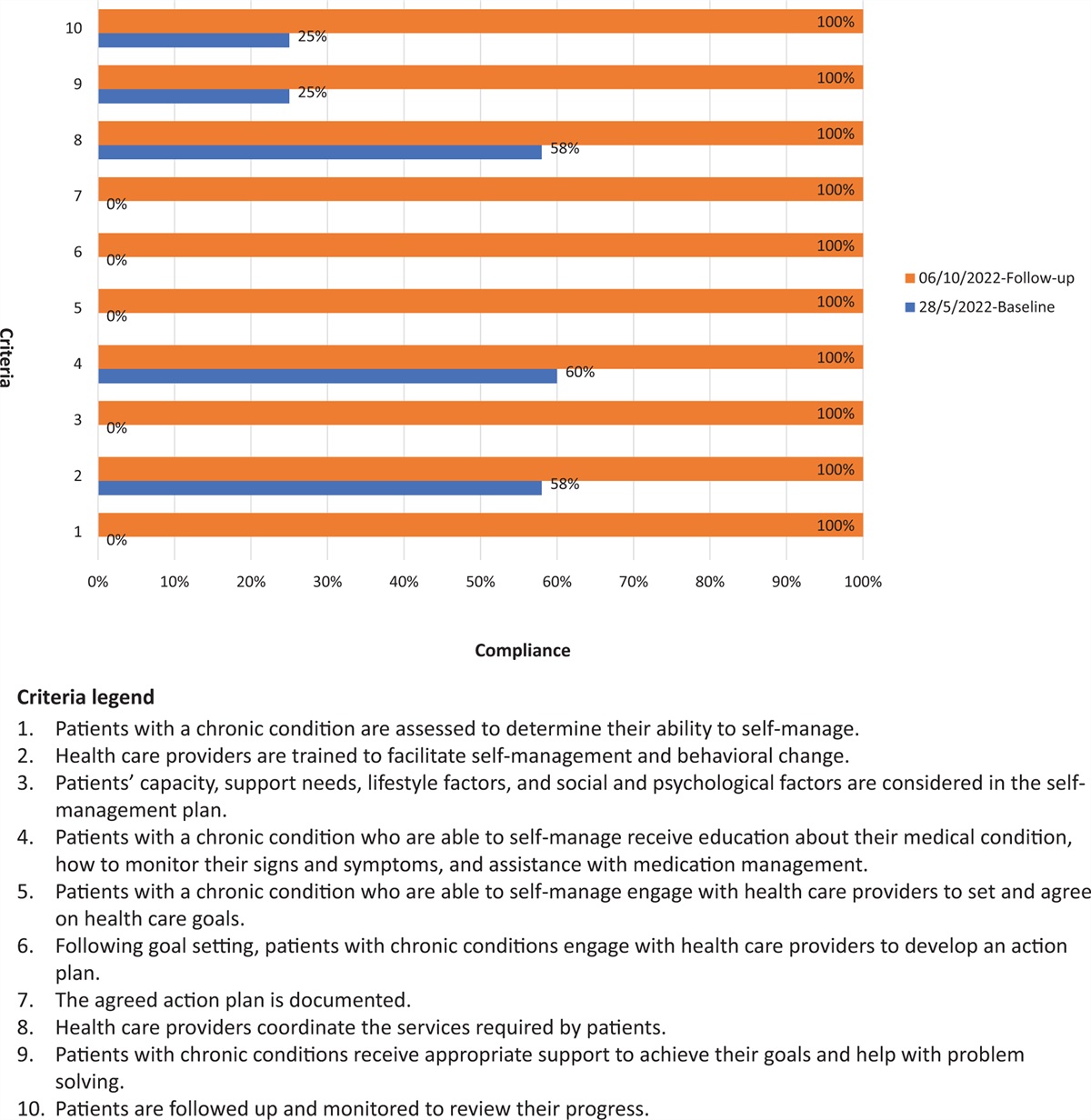
Finally, the nurses complied with almost 100% of the standards set out in the JBI guidelines regarding proper CVAD care skills in both baseline and follow-up audits (Fig. 4).
 Figure 4:
Figure 4: Compliance with best practice for skills of CVAD care by nurses at baseline and follow-up according to JBI guideline. CVAD, central venous access devices.
Strategies for Getting Research into PracticeBased on the findings of the baseline audit, the team members interviewed the residents and nurses about the possible barriers they faced. The results of the GRiP matrix are shown in Table 2.
Table 2 - Getting Research into Practice matrix Barriers Strategy Resource Outcomes Both physicians and nurses had insufficient knowledge of CVC insertion and dressing.The transformational leadership method17,18 was used to promote this project. The strategies that were determined are as follows:
(1) Providing ongoing education programs on CVAD care. (2) Establishing a dedicated CVAD care team. (3) Innovating and improving devices to provide CVAD care (Appendix I, Supplemental Digital Content, https://links.lww.com/IJEBH/A134 and Appendix II, Supplemental Digital Content, https://links.lww.com/IJEBH/A135). Follow-up impact evaluation and sustainability (Phases 6–7)The follow-up evaluations were conducted between December 2021 and January 2022. All items showed improvement after implementation of the evidence-based project (Figs. 1–4). Overall, the rate of CLABSI decreased to 3.9 BSIs/1000 CVAD-days during Phase 3 (Fig. 5).
 Figure 5:
Figure 5: The rate of CLABSI in the project. CLABSI, central line-associated bloodstream infections; MICU, medical ICU.
DiscussionOur project resulted in a decrease in the CLABSI rate, which dropped from 8.38 to 3.90 BSIs/1000 CVAD-days, using well established evidence and education programs through transformational leadership and team resource management.
Improving the competence of healthcare providers in providing central venous access device careThe first improvement achieved by this project was related to hand hygiene, in the context of insertion protocols, dressings, and securement dressings. The physicians’ compliance rate for I5 improved from 50% to 85.71%. The nurses’ compliance rate for D7 was 100%. We designed a musical timer to remind both nurses and physicians when washing their hands, equipped with a countdown feature lasting at least 20 s, which has been confirmed to increase the likelihood of inactivating pathogens.19
Furthermore, the nurses created a CVAD cart to facilitate CVAD care work. The cart is convenient and saves time. Finally, training programs on applying and caring for dressings were developed based on multiple workshops in which nurses were taught how to conduct daily wound assessments and change dressings according to the protocol. Nurse practitioners and leaders regularly audited the CVAD care procedure, which contributed to ensuring the consistency of care.
Improving the competence of healthcare providers in inserting a central venous access deviceHand hygiene and aseptic procedures are important during CVC insertion. However, item I5 only improved from 50% to 85.71%. The reason for this poor result may be that physicians neglected to sanitize the ultrasound probe used to evaluate the appropriateness of the potential insertion points. Residents may have been concerned about the potential risk of pneumothorax; therefore, they may have chosen the femoral vein rather than the jugular or subclavian vein. The project team employed a senior attendant physician who helped ensure the successful insertion of the CVAD. A nurse practitioner regularly audited handwashing and skin disinfectants to maximize sterile barrier precautions. This ensured aseptic technique execution during the insertion procedure. Thus, item I3 achieved 100% compliance.
Success factors of this projectThe baseline audit conducted in phase 1 showed that the initial level of knowledge and skills of physicians and nurses was not sufficient to achieve the goal of decreasing the CLABSI rate. In view of this finding, the JBI guidelines were used to design a relevant training program with the objective of strengthening participants’ knowledge and skills related to CVAD care. Five strategies were implemented to achieve a positive outcome: providing ongoing training in CVAD care techniques, establishing a CVAD care team, developing a CVAD insertion instructional video, regularly auditing compliance with the procedure promoted, and innovating and improving devices used for CVAD care.
Three success factors were identified: leadership, education and monitoring, and innovation.
1. Leadership and team resource management: Leadership and team resource management are essential components for achieving organizational goals.17,18 Although a clinical setting in the ICU is often uncertain and complex, many studies have found that transformational leaders can motivate employees to identify and work toward reaching organizational goals17,18,20 Establishing good relationships among team members is a critical factor. A trusting relationship was built between the team leader (nursing faculty) and senior attendant physicians, based on past cooperation. Thus, young physicians and nurses can follow the goals of the project and reach consensus on the discussion plan for CVC removal.
2. Education and monitoring: Based on evidence-based recommendations related to CVAD care contained in the JBI guidelines and hospital policies, an assessment tool for evaluating the relevant knowledge and skills of the healthcare providers was developed. To enhance their knowledge, all participants had to attend lectures on the indications for CVAD insertion, assessment of CVC dressings, and procedures for CVAD insertion and care. In addition, the participants’ skills improved by repeatedly practicing the overall process of CVAD care. The training was based on a learning-through-play approach and its effectiveness was assessed using baseline and follow-up audits. Finally, nurse partitioners continuously monitored physicians and nurses during the CVAD insertion and care.
3. Innovation during implementation: We developed an innovative system consisting of a CVAD knowledge package and CVAD care devices. The content of the package was critical for providing effective CVAD care, with reminders and flowcharts posted on the ICU walls. The instructional materials and devices were integrated into a CVAD care-designated cart to reduce preparation time. Finally, an innovative device to ensure proper hand washing was created to alert staff members and encourage them to wash their hands for an adequate time.
Challenges of this projectSome challenges were encountered during this project. First, some patients had allergic reactions to the chlorhexidine gluconate (CHG)-impregnated dressings. The CHG-impregnated dressing required an out-of-pocket cost of approximately NT$ 400. Clinical observations suggest that CVAD wounds frequently become damp, start oozing, or otherwise become soiled. This requires the dressing to be replaced even more frequently, making traditional gauze dressing a much more cost-effective option than CHG-impregnated dressings. It is essential to inspect a CVAD dressing regularly throughout the day. A second challenge was that communication between the team and participants required considerable time and effort. The team leader had to check the CVAD wound, lead the discussion on early CVAD removal, and coordinate the tasks to be performed. The team leader and nurse practitioner had good relationships with both physicians and nurses, and reached consensus on early CVAD removal. The final challenge was the grant application process. The team leader had to identify the right stakeholders. Moreover, preparations for launching the project had to begin 3 months before the estimated launch date.
Future implicationsBased on the implementation results, several important considerations emerged for further implications. First, adopting systematic strategies such as JBI PACES can help ensure compliance with CVAD bundle care practices. The project implementation experience can influence healthcare policymaking. Second, equipment innovation can increase effectiveness and efficiency in the work environment. Finally, activities aimed at the continuous improvement of quality should be encouraged and promoted in all units of the hospital.
ConclusionsThis project was successful in decreasing the CLABSI rate, improved the competence of healthcare providers to provide CVAD care assisted in distinguishing the type of dressing application in different circumstances. The project was also successful in identifying best practices for providing clinical care based on evidence-based suggestions, team resource management, and innovative activities. The development of team resource management capabilities should involve not only training the teamwork skills of physicians, nurse practitioners, and nurses but also enhancing their competence in using the best practices to ensure optimal CVAD insertion procedures and dressing care.
AcknowledgmentsThe authors appreciate the residents, nursing leaders, and registered nurses working in medical ICU-2 at the National Cheng Kung University Hospital for providing support for this project.
Funding for this project was provided by National Cheng Kung University Hospital (NCKUH-11107012).
Conflicts of interestThere is no conflict of interest to declare for this project.
References 1. Kolikof J, Peterson K, Baker AM. Central venous catheter. StatPearls Publishing; 2022. 2. Gahlot R, Nigam C, Kumar V, Yadav G, Anupurba S. Catheter-related bloodstream infections. Int J Crit Illn Inj Sci 2014; 4:162–167. 3. Al-Khawaja S, Saeed NK, Al-Khawaja S, Azzam N, Al-Biltagi M. Trends of central line-associated bloodstream infections in the intensive care unit in the Kingdom of Bahrain: four years’ experience. World J Crit Care Med 2021; 10:220–231. 4. Berwick DM, Calkins DR, McCannon CJ, Hackbarth AD. The 100,000 lives campaign: setting a goal and a deadline for improving healthcare quality. JAMA 2006; 295:324–327. 5. Furuya EY, Dick A, Perencevich EN, Pogorzelska M, Goldmann D, Stone PW. Central line bundle implementation in US intensive care units and impact on bloodstream infections. PLoS One 2011; 6:e15452. 6. Kaur M, Gupta V, Gombar S, Chander J, Sahoo T. Incidence, risk factors, microbiology of venous catheter associated bloodstream infections – a prospective study from a tertiary care hospital. Indian J Med Microbiol 2015; 33:248–254. 7. Ergönül Ö, Aydin M, Azap A, Başaran S, Tekin S, Kaya Ş, et al. Turkish Society of Clinical Microbiology and Infectious Diseases, Healthcare-Related Infections Study Group. Healthcare-associated Gram-negative bloodstream infections: antibiotic resistance and predictors of mortality. J Hosp Infect 2016; 94:381–385. 8. Zimlichman E, Henderson D, Tamir O, Franz C, Song P, Yamin CK, et al. Healthcare-associated infections: a meta-analysis of costs and financial impact on the US healthcare system. JAMA Intern Med 2013; 173:2039–2046. 9. Wang YC, Shih SM, Chen YT, Hsiung CA, Kuo SC. Clinical and economic impact of intensive care unit-acquired bloodstream infections in Taiwan: a nationwide population-based retrospective cohort study. BMJ Open 2020; 10:e037484. 10. Taiwan healthcare-associated infection and antimicrobial resistance surveillance [internet]. Taiwan Centers for Disease Control [internet]. 2021 [cited 2022 Sep 15]. Available at: https://www.cdc.gov.tw/En/File/Get/ES6Cw0u0egHUWks4hyrijg. 11. Gavin NC, Webster J, Chan RJ, Rickard CM. Frequency of dressing changes for central venous access devices on catheter-related infections. Cochrane Database Syst Rev 2016; 2:CD009213. 12. Ferreira JDN, Dos Santos KB, Siqueira EC, Gomes EP, Martini L, Fraga JBP, et al. Central venous catheter insertion in adult patients: a best practice implementation project. JBI Evid Implement 2020; 19:296–305. 13. Puig-Asensio M, Marra AR, Childs CA, Kukla ME, Perencevich EN, Schweizer ML. Effectiveness of chlorhexidine dressings to prevent catheter-related bloodstream infections. Does one size fit all? A systematic literature review and meta-analysis. Infect Control Hosp Epidemiol 2020; 41:1388–1395. 14. Lai NM, Chaiyakunapruk N, Lai NA, O’Riordan E, Pau WS, Saint S. Catheter impregnation, coating or bonding for reducing central venous catheter-related infections in adults. Cochrane Database Syst Rev 2016; 3:CD007878. 15. Buetti N, Ruckly S, Schwebel C, Mimoz O, Souweine B, Lucet JC, et al. Chlorhexidine-impregnated sponge versus chlorhexidine gel dressing for short-term intravascular catheters: which one is better? Crit Care 2020; 24:458. 16. Lai NM, Lai NA, O’Riordan E, Chaiyakunapruk N, Taylor JE, Tan K. Skin antisepsis for reducing central venous catheter-related infections. Cochrane Database Syst Rev 2016; 7:CD010140. 17. Peng S, Liao Y, Sun R. The influence of transformational leadership on employees’ affective organizational commitment in public and nonprofit organizations: a moderated mediation model. Public Personnel Manage 2019; 49:29–56. 18. Keskes I, Sallan JM, Simo P, Fernandez V. Transformational leadership and organizational commitment: mediating role of leader-member exchange. J Manage Dev 2018; 37:271–284. 19. Ijaz MK, Nims RW, de Szalay S, Rubino JR. Soap, water, and severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2): an ancient handwashing strategy for preventing dissemination of a novel virus. PeerJ 2021; 9:e12041. 20. Buil I, Martínez E, Matute J. Transformational leadership and employee performance: the role of identification, engagement and proactive personality. Int J Hosp Manage 2019; 77:64–75.
Comments (0)