One essential characteristic of modern life is that we all depend on systems—on assemblages of people or technologies or both—and among our most profound difficulties is making them work. 1
Making things work is one of the most consistent challenges in healthcare. A large, disparate workforce, complex work environments, varied funding models – it seems the most consistent feature of healthcare is the pressure and pace with which staff need to become proficient. But who makes it work, how do they know it is ‘working’, and more importantly, how do they – the people who make it work – lead change to ensure it keeps working?
This issue of JBI Evidence Implementation includes key examples of making it work across diverse fields of practice, with a common conceptual basis. The JBI Model of EBHC (evidence-based healthcare) is a global point of reference for best practice.2 Audit and feedback as a change process informed by the JBI Model, demonstrates the relationship between healthcare needs, types of evidence, methods of synthesis and transfer, and how these drive implementation.3 The model is widely cited in implementation studies, emphasizing that evidence-based practice change involves access to synthesized evidence, rather than reliance on single studies. It also shows users how transfer mechanisms support implementation planning by building knowledge, capacity, and expertise through hands-on education, training, skill, and knowledge transfer.2 The model also explains how integrated approaches to EBHC can be developed.
Central to each implementation study in this issue are clinician–academic partnerships, and how drawing on evidence-based tools, resources, skills, and knowledge showcases local knowledge and expertise for evidence-based practice. JBI is a global leader in EBHC, with widely accessible online tools and resources to support implementation; enhance and enable capacity; add value and decrease costs; and enable clinicians to use their knowledge and expertise to improve safety and quality through evidence-based practice. These online tools can be used as stand-alone resources or they can be used through a toolbox approach, as favored by many health systems and services.4
Systems-based approaches that standardize EBHC pathways and processes while allowing for individual, patient-centered variation make our health services safer. Without these systems, patient experiences and outcomes would be dramatically lower. High-quality implementation methods share these characteristics of standardized methods and reliability while enabling localized change. How? By providing flexible systems and approaches that enable clinician-led, patient-centered care to drive practice change, whether at the small scale of a single ward or unit, or across multisite organizations.4
…the volume and complexity of what we know has exceeded our individual ability to deliver its benefits correctly, safely, or reliably. Knowledge has both saved us and burdened us.1
Making it work is the raison d’être, it is why we get out of bed and head into some of the most complex, challenging, and constrained work environments in the world. This desire to make it work stimulates innovation, research, and clinical practice; however, it also requires a diverse professional workforce to keep the system functional. We can have both. As this issue illustrates, we can reduce complexity, while improving safety and quality. This system improvement capacity is partly driven by implementation characteristics that are common across cultures, geographic regions, and health settings. The implementation projects in this issue span these diverse characteristics through a shared framework and evidence base. Some of these projects include bladder management for intrapartum and postpartum women at a maternity hospital, improved care for patients with radiation-induced trismus associated with nasopharyngeal carcinoma, pressure injury prevention, decreased central line-associated bloodstream infection, and assessment of hypertensive disorders during labor. These projects span the globe, reflecting distinctive cultural characteristics from Taiwan, Mississippi, China, Brazil, and Iran.
These reports demonstrate the value of nurses and practicing health professionals participating in evidence-based practice:
(1) Accessibility and opportunity have never been higher for nurses and practicing health professionals who want to embrace quality in professional practice.
(2) Diversity of populations, culture, variability in systems and organizational contexts based on common models, methods, and mechanisms of action enables shared, transferable knowledge.
(3) There is a patient-centered return on investment from the organizational imperative to create opportunities for nurses and practicing health professionals to embrace quality through ward-based or unit-based quality improvement activity.
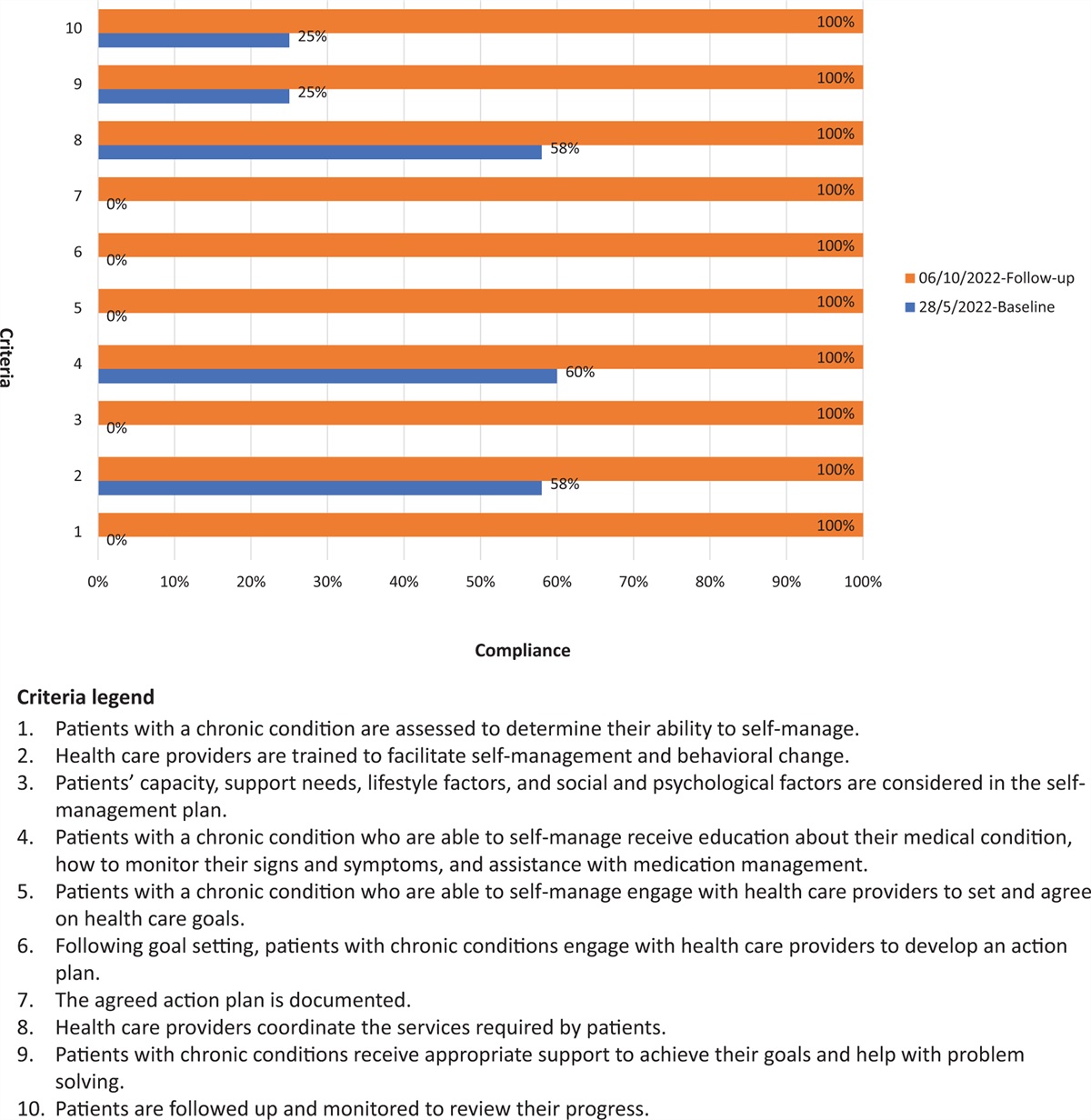
The consistency of model, method, and mechanism of action across diverse topics, geographic locations, and cultural settings is important. It indicates robust methods with a high degree of transferability. Implementation planning informed by baseline compliance data is how localization of global evidence, tools, and resources contribute to better quality care. JBI provides groups of practitioners with a ready-to-use framework for implementation planning, resolving uniquely local problems and supporting practice change through the evidence-based review.4 This raises the question: are these part of your individual or organizational toolbox for implementation?
Making audit and feedback work requires training, teamwork, skills, knowledge, and access to evidence-based resources. JBI offers these worldwide, enabling collaborating healthcare groups to develop locally relevant topics into evidence-based audit criteria. If your organization wants to be ready, gear up with a toolbox of consistent and transparent processes, with a focus on standards for practice and clinical implementation, this issue is for you. More importantly, JBI is for you.
Acknowledgements
I would like to thank Ms Camilla Smolicz, JBI Copy Editor who provided high-quality medical copy editing of the draft, which has improved the quality but not materially changed the context or direction of the submission.
I declare that this work as submitted is original, was conceptualized by C.S.L., has not been submitted or published elsewhere.
Conflicts of interest
There are no conflicts of interest.
References
1. Gawande A. The checklist manifesto: how to get things right. New York: Metropolitan Books; 2009.
2. Jordan Z, Lockwood C, Munn Z, Aromataris E. The updated Joanna Briggs Institute Model of Evidence-Based Healthcare. Int J Evid Based Healthc 2019; 17:58–71.
3. Khalid AF, Grimshaw JM. Preparing for audit and feedback: practical considerations. JBI Evid Implement 2022; 20:111–112.
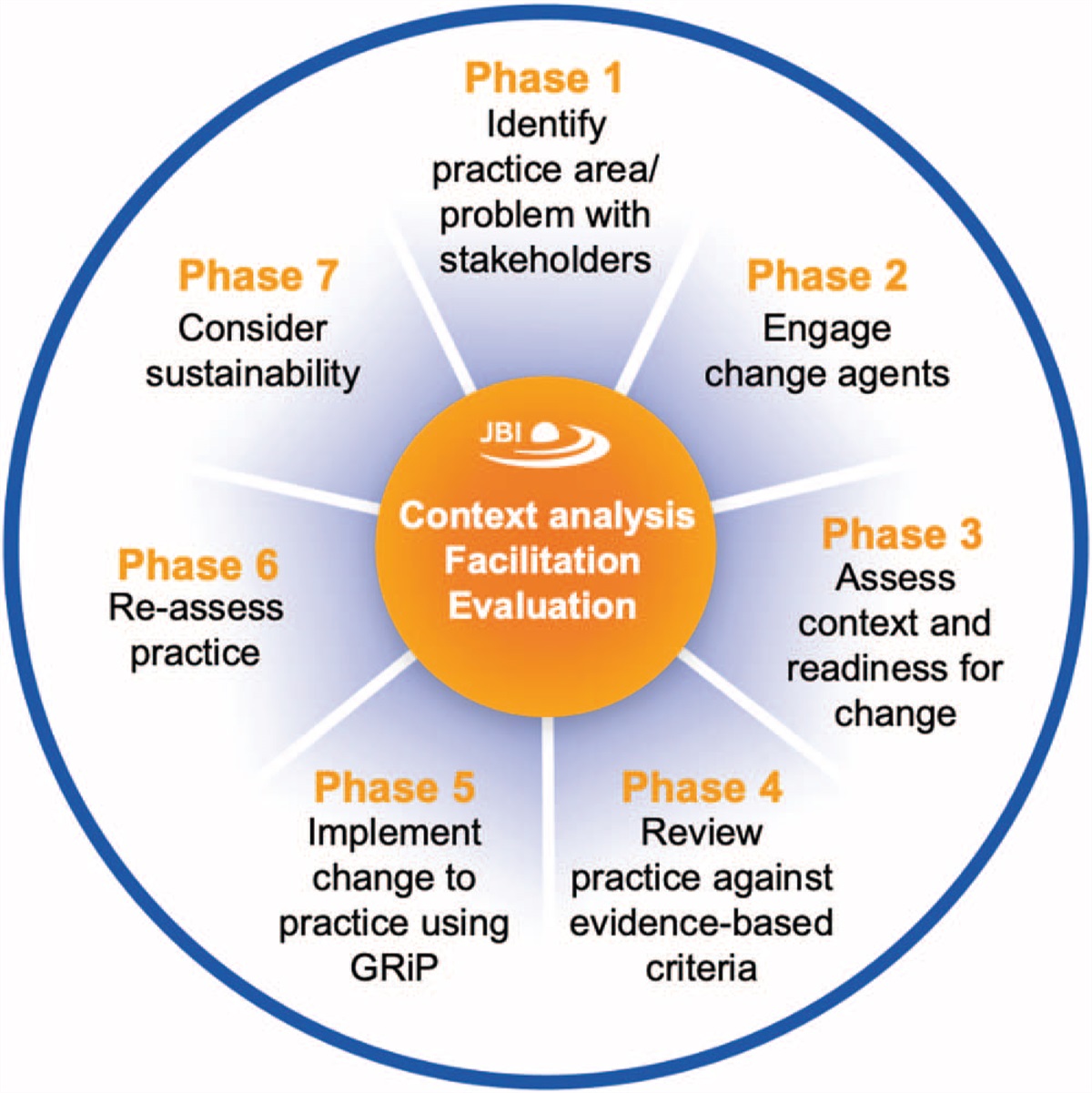
4. Porritt K, McArthur A, Lockwood C, Munn Z. JBI's approach to evidence implementation: a 7-phase process model to support and guide getting evidence into practice. JBI Evid Implement 2023; 21:3–13.




Comments (0)