
Remember me



Femoral shaft fractures are one of the most common orthopedic injuries in pediatric patients. In children below 5 years of age, the gold standard for treatment of these injuries is closed reduction and hip spica casting.1 Although pediatric patients possess significant remodeling potential, it is not unlimited. Although Lovell and Winters criteria suggest acceptable parameters of <20 degrees angulation in any plane and <3 cm shortening,2 long-term follow-up data were lacking to definitively quantify how much deformity will ultimately remodel and may be safely accepted. American Academy of Orthopaedic Surgeons clinical practice guidelines recommend monitoring for maintenance of appropriate alignment but do not precisely define acceptable parameters. With this in mind, surgeons must be prepared to intervene operatively in cases where acceptable alignment cannot be maintained in a hip spica cast, even after remanipulation and/or cast wedging. Furthermore, length unstable and early healing may not allow for an adequate closed reduction with the use of less invasive techniques such as flexible intramedullary nailing. In these cases, when a child is subjected to the increased risk of an open procedure along with the associated disruption of soft tissue and fracture callus, it is even more critical to achieve an accurate reduction. Unfortunately, the deforming forces associated with these injuries make this technically challenging. The purpose of this acticle is to illustrate the technique and effectiveness of combining a Jungbluth clamp with a cerclage wire to achieve an anatomic reduction in the setting of a pediatric femur fracture.
SURGICAL TECHNIQUEA 4-year-old female presented to the emergency department after a fall off monkey bars sustaining an isolated closed left femoral shaft fracture (Fig. 1A) (OTA/AO 32-D/5.1).3
 FIGURE 1:
FIGURE 1: A, Injury films depicting left femoral shaft fracture. B, Closed reduction and spica casting of left femoral shaft fracture.
Within 24 hours of presentation, the patient was treated with a closed reduction and left-sided one-and-one-half hip spica casting (Fig. 1B). One week later, the patient presented to the outpatient office, and the decision was made to continue with close observation (Fig. 2A). The malalignment persisted at the 2-week visit (Fig. 2B), and cast wedging was performed at that time (Fig. 2C).
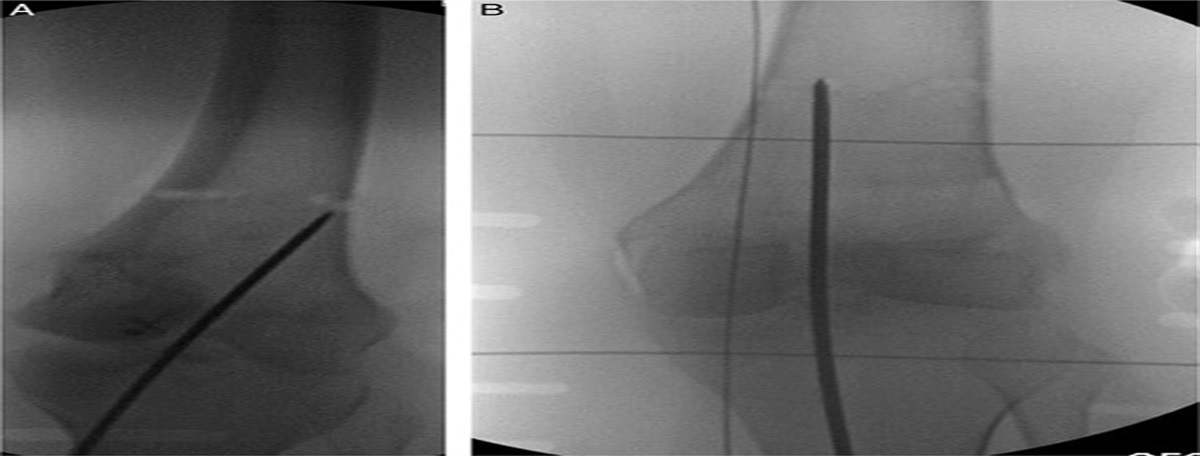
 FIGURE 2:
FIGURE 2: Follow-up films at 1 week postinjury (A), 2 weeks postinjury (B), and 2 weeks postinjury (C) after cast wedging.
At the 3-week visit, the patient was found to have worsening varus angulation of 20 degrees, apex anterior angulation of 25 degrees, and 2 cm of shortening. After discussing options, including continued observation with possible future corrective surgery and acute open reduction internal fixation, the family chose to proceed with the latter.
The patient was brought to the operating room for open reduction internal fixation of the left femur 27 days after the initial injury. The spica cast was removed, and the patient was placed supine on a radiolucent table. No instability of the fracture was noted with manipulation.
A lateral incision was made centered over the fracture site. Dissection was carried down to the level of the iliotibial band. The iliotibial band was split, and a subvastus approach was utilized to visualize the fracture. There was a significant callus formation at the fracture site, which was debrided, yielding clean fracture ends. Multiple attempts using gross traction and serrated clamps failed to restore anatomic length and overall reduction. At this point, a Jungbluth pelvic reduction clamp was affixed to the anterolateral aspect of each fragment using two 3.5-mm cortical screws. After several failed attempts to obtain an anatomic reduction, a circumferential cerclage wire was placed around the oblique fracture fragments. As the Jungbluth clamp was used to distract the fracture fragments, the cerclage wire was tightened to aid in reduction. Once an anatomic reduction was obtained, the cerclage wire was finally tightened to allow for the removal of the Jungbluth clamp (Fig. 3A). A 3.5-mm limited contact-dynamic compression plate was then applied with 3 bicortical screws on either side of the fracture using the dynamic holes to compress the fracture. The cerclage wire was then removed for concern for potential boney overgrowth and subsequent difficulty should the hardware need to be removed in the future. Lastly, given the long obliquity of the fracture, a 3.5-mm lag screw was then placed through the plate to augment the compression of the fragments (Fig. 3B).
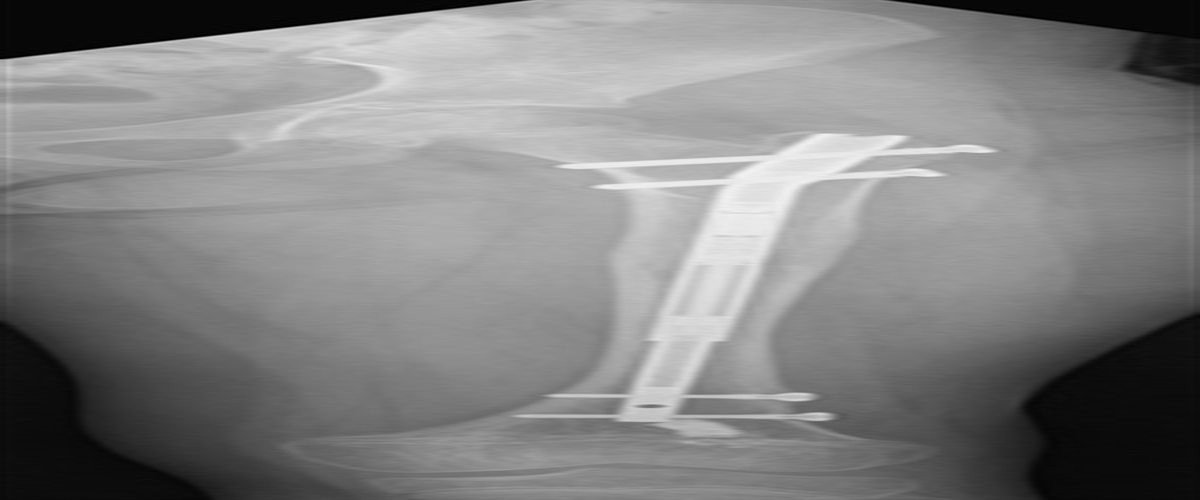
 FIGURE 3:
FIGURE 3: A, Intraoperative x-ray with two 3.5-mm screws in proximal/distal fracture fragments Jungbluth clamp in place and cerclage wire maintaining anatomic reduction. B, Image taken before the removal of Jungbluth clamp. C, Final fixation utilizing a 3.5 mm limited contact-dynamic compression plate screw construct.
After all fixation was in place, final orthogonal fluoroscopic views were obtained before routine closure and dressing. Postoperatively, the patient was made non–weight-bearing on the injured extremity with plans to follow up in the office in 2 weeks. At 2 weeks, the patient was allowed to begin protected weight-bearing. She was then examined in the office at 6 weeks to be walking without a limp and without aid. x-Rays at the time of the final evaluation showed a healed left femur fracture (Fig. 3C).
EXPECTED OUTCOMESIn femoral shaft fractures, the restoration of coronal, sagittal, and axial alignment can be challenging because of powerful deforming forces. Adding to these, challenges in pediatric patients are concerns for growth disturbance, inability to use fracture table, delay in surgical treatment due to initial attempts at nonoperative management, and accelerated fracture healing. Current guidelines suggest spica casting, submuscular plating, or intramedullary nailing; however, successful implementation of any of these strategies is predicated upon achieving the reduction of the fracture within acceptable parameters. In cases where adequate reduction cannot be achieved or maintained with closed methods or when reducing a fracture that has partially healed, the Jungbluth clamp used with a cerclage cable is a powerful technique. Compared with other fracture reduction methods, such as the femoral distractor, the size, and shape of the Jungbluth clamp, are optimized for working in confined spaces in pelvic and acetabular surgery, making it ideal for use in pediatric patients. Along the same lines, 3.5 mm screws used with the Jungbluth clamp fit more readily in smaller pediatric femurs than 4.0 or 5.0 mm Schanz pins. In addition, when using a Jungbluth clamp, a torsional force can be applied to the handles by the surgeon to further improve the reduction. Other reduction techniques, including using a push-pull screw or an articulated tension device, require the plate to be placed before reduction, which can be difficult and lead to plate malposition. In addition, these 2 previously mentioned techniques require a considerable increase in soft tissue dissection, whereas the method we described limits the dissection to an area that would otherwise be exposed for fracture site debridement and or plate placement.
Open reduction in this manner combined with plate fixation maintains length, and as Li et al4 found, the treatment of length unstable femoral shaft fractures with plate fixation in the pediatric population is associated with better outcome scores and lower complication rates compared with the treatment with titanium elastic nails.
Surgeons must be prepared to perform open reduction of these injuries, particularly in the setting of delayed surgical intervention and in fractures involving the proximal or distal ends of the femoral shaft. As shown here, when necessary, the Jungbluth clamp combined with a cerclage wire can be a valuable part of the surgeon’s armamentarium for this purpose.
COMPLICATIONSWith any open reduction internal fixation procedure, the risks of bleeding, infection, malunion, and damage to nearby neurovascular structures are present and must be discussed during the consent process. As with the use of any reduction clamp, there is a risk of iatrogenic fracture. However, with the Jungbluth clamp, this risk can be minimized by placing bicortical screws away from the fracture site and in favorable positions to gain the reduction and allow for an unobstructive plating of the fracture.
REFERENCES 1. Flynn JM, Schwend RM. Management of pediatric femoral shaft fractures. J Am Acad Orthop Surg. 2004;12:347–359. 2. Misaghi A, Mahmoud MAH, Arkader A, et al. Fracture characteristics predict suboptimal alignment in preschool femoral shaft fractures treated with spica casting: a retrospective chart review. Curr Orthop Pract. 2020;31:379–384. 3. AO pediatric comprehensive classification of long bone fractures (PCCF). J Orthop Trauma. 2018;32:S117–S140. 4. Li Y, Heyworth BE, Glotzbecker M, et al. Comparison of titanium elastic nail and plate fixation of pediatric subtrochanteric femur fractures. J Pediatr Orthop. 2013;33:232–238.
Comments (0)