
Remember me

As global progress continues toward controlling the HIV epidemic, increased support for nurses and midwives providing frontline service delivery is essential (Michaels-Strasser et al., 2018). Beyond increasing the number of nurses and midwives, investments to improve the quality of their working environment, to ensure evidence-based education for continuing professional development, and to align policies to standardize scopes of practice should be considered (World Health Organization [WHO], 2016). Authorization of nurse-initiated and managed antiretroviral therapy (NIMART) has expanded nurses' scopes of practice to include viral load testing and interpretation, management of treatment failure, prevention of mother-to-child transmission (PMTCT) services, and prophylaxis for infants and opportunistic infections (Zuber et al., 2014). As NIMART becomes more widespread, incorporating clinical mentorship to reinforce didactic knowledge coupled with hands-on training can strengthen continuous quality improvement programs for nurses and midwives. The International Training and Education Center for Health (I-TECH) describes clinical mentorship as the bridge between classroom education and independent clinical practice, which includes five main concepts: relationship building, identification of improvement areas, coaching and modeling best practices, advocating for supportive work environments (e.g., systems-level enhancements), and data collection and monitoring (I-TECH, 2008). Our goal is to provide a method to assess the implementation of a mentorship program for nurses' and midwives' expanded scope of practice in HIV care with an emphasis on maternal child nursing.
The World Health Organization's Global Strategy for Nursing and Midwifery 2016–2020 promoted collaboration across national, regional, and community levels to continuously support nurses and midwives in advanced practice (WHO, 2016). The African Regional Collaborative for Nurses and Midwives (ARC) initiative, funded by the US President's Emergency Fund for AIDS Relief, implemented health system interventions to improve HIV service delivery. ARC convened nursing and midwifery leadership teams from 18 countries across East, Central, and Southern Africa to advance nursing practice and regulation. Results from the initiative's regulatory collaborative (2011–2016) were published previously (Gross et al., 2018). In 2016, ARC pivoted from focusing on regulatory enhancements to quality clinical care, launching a new collaborative to improve the confidence and competence of nurses and midwives delivering HIV services by leveraging existing national and cross-country networks.
ARC's mixed method baseline assessment across 11 countries revealed gaps in supportive supervision and clinical mentorship among nurses, midwives, and nurse midwives, especially related to performance feedback on the provision of pediatric HIV services (MacKay et al., 2020). The ARC quality improvement initiative awarded 1-year small grants to five teams for the development of quality improvement projects from August 2016 to July 2017. Kenya, Lesotho, Malawi, Rwanda, and Zambia implemented clinical mentorship projects with their ARC grants to strengthen nurse-led and midwifery-led HIV care. Projects aimed to increase nurses' and midwives' competence in health services delivered to HIV-positive pregnant and breastfeeding women (PBFW), HIV-exposed infants (HEI), and children and adolescents living with HIV (PEDS). Therefore, the teams' efforts focused on improving quality of PMTCT services, through services to HIV-positive PBFW and their HEIs, as well as to children and adolescents living with HIV, or PEDS. Country teams chose specific goals and activities for their clinical mentorship projects, focusing on one or more of the specific patient populations aforementioned (Table 1). Thus, providers received clinical mentorship on the patient populations (i.e., PBFW, HEI, PEDS) identified by their country team.
Table 1. - Clinical Mentorship Projects by Country and Patient Population Country Activities Population Kenya • Established continuous quality improvement systems (CQI) at priority sitesNote. HEI = HIV-exposed infants; NIMART = nurse-initiated and managed antiretroviral therapy; PBFW = pregnant and breastfeeding women.
Nursing leadership teams from each country led project development and implementation of NIMART needs for the specific patient populations. National nursing and midwifery leadership teams included the Chief Nursing Officer (Ministry of Health [MOH]), Registrar (Nursing and Midwifery Regulatory Council, academic representative (Health Professional Training Institutions), and the president (National Nursing and Midwifery Professional Association). The Nell Hodgson School of Nursing at Emory University served as the implementing partner, assisting countries with project design, evaluation, and facilitation of collaborative efforts. The US Centers for Disease Control and Prevention (CDC) provided technical assistance. Other key partners included the ARC Secretariat in Nairobi, Kenya, East Central and Southern Africa College of Nursing, the Commonwealth Nurses and Midwives Federation, and Emory University's Lillian Carter Center.
A site-level tool, the nursing practice framework (NPF; Appendix A, https://links.lww.com/JNC/A36), was used to evaluate the implementation of tailored mentorship programs in Kenya, Lesotho, Malawi, Rwanda, and Zambia. The NPF is an adaptation of a capability maturity model, which is used to evaluate an organization's capacity to perform necessary functions in a structured, sequential manner (McCarthy et al., 2014). Models are created by determining the operational needs of an organization and describing the maturation of each function by advancing along a linear scale of increasing capability (McCarthy et al., 2014).
 Figure 1.:
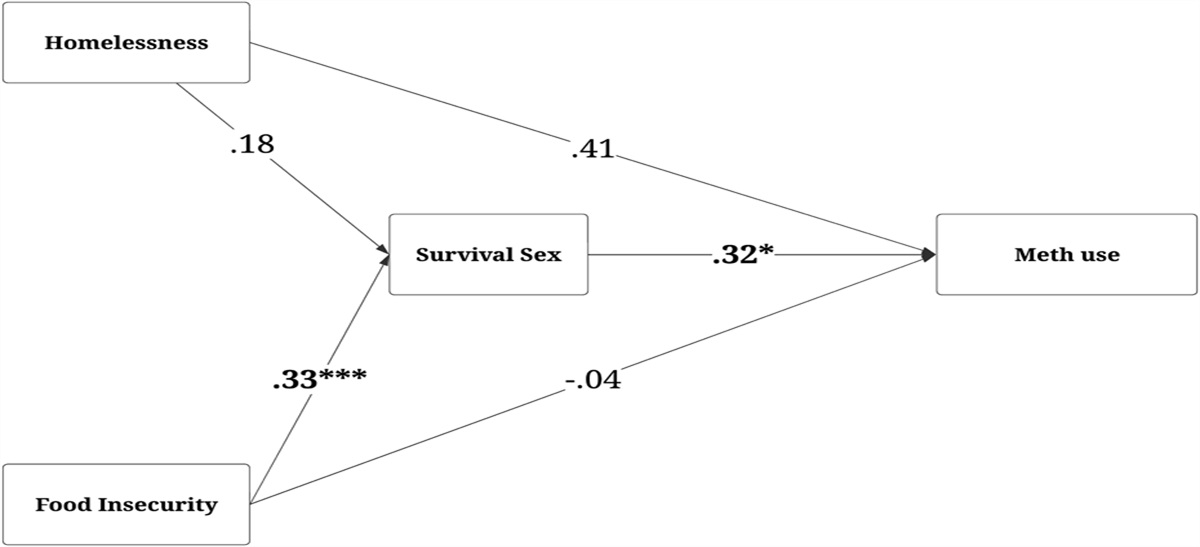
Figure 1.: Nursing Practice Framework (NPF) stage progression in PMTCT and PEDS. PMTCT = prevention of mother-to-child transmission.
Five stages comprised the NPF for clinical mentorship program evaluation. Stage 1 indicated that a facility did not have a clinical mentorship program or that there was ongoing planning for a clinical mentorship program. Stage 2 documented an existing mentorship program. Stage 3 indicated routine activities, such as mentor feedback on clinical care practice. Stage 4 represented an improved program with increased supportive supervision or mentor involvement in case reviews. Stage 5 demonstrated an optimized program that transitioned nurses and midwives into the role of new clinical mentors. A key outcome of Stage 5 is demonstration of competencies by new mentors, which would include understanding clinical knowledge followed by real-world application. Therefore, a knowledge assessment was used to measure nurses' and midwives' competencies in areas of maternal, infant, and pediatric HIV care. This article describes use of the NPF to assess implementation of clinical mentorship projects and presents a discussion on the potential workforce challenges during the process, both of which contribute to quality improvement needs for HIV service delivery at the site level.
 Figure 2.:
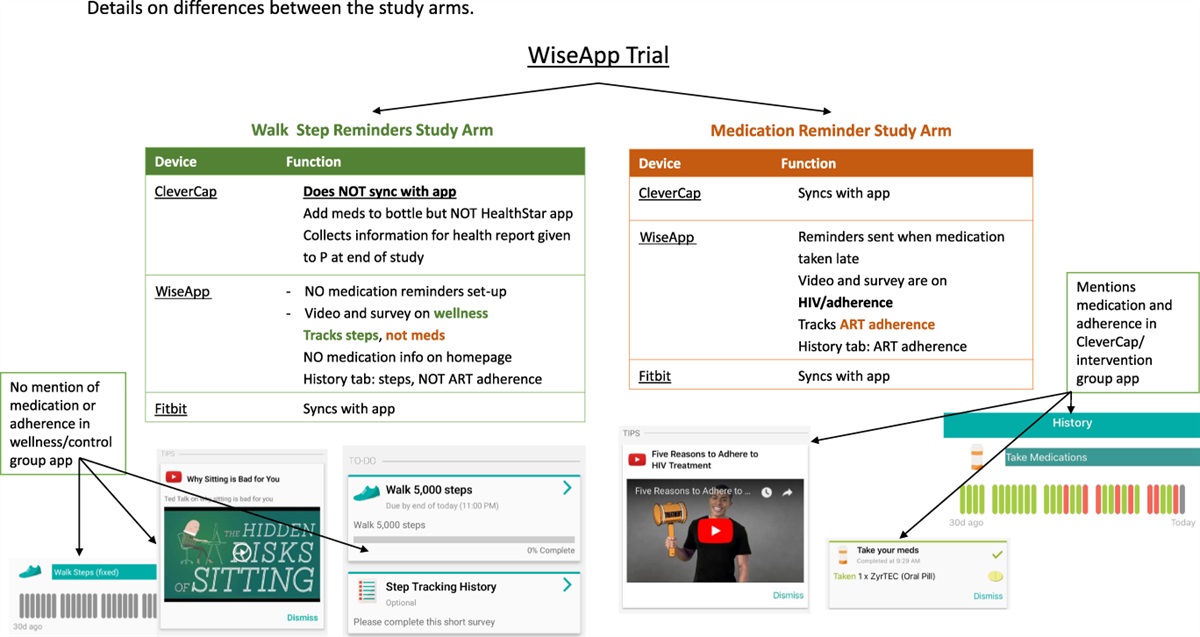
Figure 2.: Knowledge assessment scores for nurses and midwives pre- and postimplementation by country and patient population.
MethodsThe ARC initiative conducted facility assessments using the NPF and knowledge assessments of individual providers. These assessments measured (a) the maturity of each facility's clinical mentorship programs based on the capability maturity model and (b) nurses' and midwives' knowledge of clinical competencies linked to the NPF for on-going mentorship. Each country's MOH provided approval for the facility assessments, and informed consent was required for individual interviews and knowledge assessments. The protocol was approved by the Institutional Review Bord (IRB) at the Emory University as nonresearch, and this project was reviewed in accordance with CDC human research protection procedures and was determined to be a nonresearch public health program activity.
Facility-Level Assessment: Nursing Practice FrameworkAlthough the NPF evaluated six domains of structural maturity, including continuing professional development, clinical mentorship, scope of practice and task sharing, patient provider interaction, quality improvement and assurance, and data use and data quality (Appendix A, https://links.lww.com/JNC/A36), this analysis only included an assessment of pre-/postperformance on the clinical mentorship domain because this was the focus of the intervention projects. Clinical mentorship activities for PBFW and HEI were classified as PMTCT and for children living with HIV as PEDS HIV service delivery. Data were collected before and after the implementation period. Facilities received stage designations at both the pre- and post implementation periods based on the responses. Outcomes were presented as an improvement, regression, or no change.
Eight facilities were included in the NPF analysis to describe the maturation of clinical mentorship programs at each facility. Teams chose facilities based on HIV service provision needs for selected patient populations. Facility types included four hospitals, two clinics, and two health centers. Facility breakdown by country included the following: a hospital in Kenya; hospital and clinic in Lesotho; two health centers in Rwanda; hospital and clinic in Zambia; and a hospital in Malawi. Facility assessments were conducted with nursing and midwifery supervisors or clinical managers knowledgeable of facility-level support structures for nursing and midwifery practice in HIV care. The assessment consisted of structured interviews as well as review of relevant facility documents. Training was provided to all ARC country team members through instruction manuals, virtual training sessions, and in-person (face-to-face) meetings on how to conduct the facility assessments.
Nursing and midwifery leadership interviewed supervisors or clinical managers individually in a private setting at their intervention sites on the establishment of practices for six clinical support structures: continuing professional development, clinical mentorship, scope of practice and task sharing, patient–provider interaction, quality improvement and assurance, and data use and data quality, using the NPF.
Completed questionnaires were scanned into a password-protected computer and further stored on a password-protected hard drive as designated by the facility assessment team leader. Each interview (one per facility) was transcribed onto an electronic, protected-word document data form. The electronic data forms were saved on a password-protected computer and then saved to a password-protected hard drive designated for backup. The teams were instructed to backup all files. Once assessments were complete for the select facilities, an ARC country team member sent completed data to ARC faculty at the Emory University. These data were entered into an Excel spreadsheet categorized by service types: PMTCT or PEDS HIV. A descriptive analysis was conducted by CDC-Emory analysts by developing a codebook for the responses and coding in alignment with the NPF to assess program maturity from Stage 1 to Stage 5.
Provider-Level AssessmentNurses and midwives at each country teams' priority intervention sites completed the same knowledge assessment before and after the implementation period from August 2016 to September 2017. A convenience sample of 147 nurses and midwives who were providing PMTCT and pediatric HIV services, present at the time of the pre- and postassessments at high priority sites implementing clinical mentorship program improvement projects, completed the provider-level knowledge assessments. There were 54 participants at preimplementation and 93 at postimplementation due to changes in provider staffing and availability at these sites. The knowledge assessment was divided into three sections on clinical competencies for each patient population, with 11 questions on PBFW, 11 questions on HEI, and seven questions on PEDS HIV care. The assessment was administered in a proctored group setting; providers took the assessment at various times based on clinical workload.
The knowledge assessment, developed in consultation with CDC subject matter experts and in accordance with clinical practice guidelines and US President's Emergency Fund for AIDS Relief guidance for HIV prevention, care, and treatment services for PBFW, HEI, and children living with HIV, was not externally validated. Clinical competencies tested for PBFW included the following: perinatal HIV transmission, Option B+ services, guidance on provider-initiated counseling, HIV rapid testing, HIV posttest counseling, WHO regimen recommendations for antiretroviral (ARV), antiretroviral therapy (ART) initiation, supportive strategies for ART adherence counseling, HIV viral load monitoring, partner testing, and counseling services. Knowledge for HEIs comprised early infant diagnosis (EID) testing, understanding results for the management of medications, ARV prophylaxis for breastfeeding mothers, WHO testing recommendations, early testing, breastfeeding counseling (exclusive), routine care for infants with mothers with HIV, types of HIV tests, dried blood spot technique, and prescribing ARVs. Pediatric competencies tested included the following: ART initiation, HIV viral load testing, recognition of ART treatment failure, supportive management for children to maintain therapeutic regimens, transitioning to adult care, postexposure prophylaxis for victims of sexual violence, and guidance on age-appropriate status disclosure.
Results were analyzed before and after the implementation of the clinical mentorship interventions to compare performance in competencies. Individual participant scores were calculated for each section. Next, the participant scores were averaged for each section, and the standard deviation (SD) for each section was calculated for all sites included in the country team.
ResultsAt the facility level, structural improvements (i.e., changes in maturity) for clinical mentorship programs were evident for PEDS and PMTCT for each country team (Figure 1). At the provider level, there was an increase in the number of participants from pre- to posttest knowledge assessments across the three professions: at pretest, there were 15 nurses with an increase to 38; a total of 2 midwives increased to 11, and 37 nurse-midwives increased to 42 at posttest. Results are presented by country team describing (a) each facility's change in maturity for their clinical mentorship program by NPF stage and population area (i.e., PMTCT or PEDS) and (b) changes in provider-level competencies by population area (i.e., PBFW, HEI, or PEDS) (Figure 2).
Country Team ResultsThe country team in Kenya established a clinical mentorship program for both PMTCT and PEDS at their intervention site. PEDS was the primary focus for which there was an improvement to Stage 4 and Stage 5 for PMTCT. Only nurse-midwives completed the assessment with 13 at pretest and 12 at posttest. Participant scores increased in PBFW, HEI, and PEDS sections—most notably their HEI scores improved by double from 48% (SD 21) to 85% (SD 5).
Intervention sites in Lesotho progressed to Stage 5 for PMTCT and PEDS programs. These sites reported activities to promote mentor availability by collaborating with their MOH. Mentors at one facility assisted staff with case reviews, patient documentation, and follow-up care. Both facilities had a mix of nurses and nurse-midwives who completed the assessment. Before implementation, there were 13 nurse midwives. After implementation, there were 13 nurse midwives and 4 nurses. Average scores remained above 85% in each competency area. PBFW scores slightly increased, and HEI and PEDS scores remained within 2–4% pre- to posttest. Participants' averages remained well above 80% despite slight decreases in HEI and PEDS sections.
Malawi's team implemented their program at one site that began at Stage 5 and was unchanged after implementation. Nurse midwives were the main cadre at the facility with 8 at pretest and 12 at posttest. Overall, there was a decrease in scores for each section. Participant scores in PBFW and HEI went down by 6–9%. PEDS scores had the lowest averages and remained within 1% from pre- to posttest: 77% (SD 17) and 76% (SD 21), respectively.
Rwanda's team established mentorship programs in two high-volume facilities. Both sites progressed to Stage 5 for both PMTCT and PEDS programs. This team's approach included integration with the MOH similar to Lesotho's facilities. Scheduling weekly visits/phone calls with district mentors appeared to be a helpful strategy to support mentees and the program. Only nurses participated in the knowledge assessment with four at pretest and nine during the posttest. The PBFW average score was 88% (SD 17) at pretest, which decreased to 81% (SD 18) at posttest. The pretest average scores for HEI and PEDS were lower (54–59%) but improved by 10–15% at posttest.
Zambia's team established a mentorship program at two sites for PMTCT and PEDS. One facility progressed to Stage 3 for the PEDS program, and the second facility progressed to Stage 5 in PMTCT. The facilities had the most diverse group of participants, which included nurses (11 pre; 25 post), nurse midwives (four pre; four post), and midwives (2 pre; 11 post). Facilities saw the largest increase in posttest participants that included 14 more nurses and nine more midwives. Scores from pre to post in all three areas declined with the largest change in PBFW: 88% (SD 17) to 71% (SD 24). HEI and PEDS average scores were in the mid 60–70% at pre and low to mid 60% at post.
DiscussionThe ARC quality improvement initiative demonstrates a descriptive assessment using a nurse-specific framework for the development and implementation of clinical mentorship programs focused on HIV care. Furthermore, a rapid evaluation of clinical competencies provides insight into the on-going mentorship needs for PBFW, HEI, and PEDS HIV populations. The NPF measured site-level structural maturity to describe the stage of a clinical mentorship program before and after the intervention. Most facilities began at Stage 1 and progressed to Stage 3 or higher for both PMTCT and PEDS. Overall, provider knowledge on PBFW had the highest averages, indicating higher levels of competency when caring for this population. HEI and PEDS competencies averaged lower than PBFW; of interest, PEDS HIV competencies were higher compared with HEI. More context about programmatic support is needed to support mentorship for infants and children. Programs can consider exploring ways to support improvement in clinical competencies for HIV-exposed infants and pediatric HIV care, specifically. Given the increased number of participants from the pretest to the posttest across all facilities, it is difficult to know how staff changes for each team affected implementation and/or the outcomes. Furthermore, NPF allows for an evaluation of workforce challenges, such as staffing and resource availability, which is described in previous studies. The country team in Kenya established a program that demonstrated a positive trend in program progression and increased average scores from pre to post in PBFW, HEI, and PEDS competencies. There was only one additional participant at posttest at the Kenya facility. This was a similar trend to the intervention site in Malawi, which added four participants at posttest, but there was a slight decrease in scores.
Malawi's team focus was to enhance mentorship that would improve EID as part of the HEI focus. The largest shift from pre- to posttest was that the HEI scores and the PEDS scores remained above 75% with 1% difference. This smaller change in scores and staff invites us to evaluate both staffing changes and specific mentorship needs. The notable program progression describes a positive step in the right direction.
Intervention sites in Rwanda experienced a similar staff change as the site in Malawi, but scores improved in HEI and PEDS competencies. Although the scores were low, the increase in scores demonstrates structural gains. In addition, the partnership with the MOH allows for implementing partners to provide clinical mentorship on new HIV guidelines, highlighting the benefits of integrating facility-based support programs into MOH structures that will remain, even after clinical support partners have gone (Goosby et al., 2012).
Integration of clinical mentorship programs into existing MOH structures have also demonstrated improvements in the quality of care along with cost-effectiveness in a previous study evaluating an antenatal program in Rwanda (Manzi et al., 2019). The evaluation noted a slight increase in cost, but improved quality of care and a more comprehensive program with lower overall projected health care costs (Manzi et al., 2019). Although cost was not evaluated in this study, it is an important factor that can be analyzed in Stages 1 or 2 of the NPF. Limited resources for a mentorship program often lead to fewer participants. In a previous study, increased funding for more consultation space, resources that reduced medication stock outs, and proper equipment for vital signs and health assessments improved provider needs (Chien et al., 2016). These changes resulted in higher mentee satisfaction and confidence, which improved patient–provider interactions.
Lesotho's team also collaborated with the country's MOH. Four more participants were noted at posttest, which is a small change. The program operated well with scores ranging well above 85%; therefore, individual-level factors may be more appropriate to consider in this case. At Stages 3 and 4, the NPF measures a program's ability to provide routine supportive activities to improve mentees' clinical skills. This is an opportunity to identify mentees' learning preferences, which could be more beneficial in their transition to becoming new mentors (Stage 5). Authors in a previous publication found three preferences: 48% of mentees preferred observation and immediate critique while completing the task, 42% preferred critiques after observation, and 42% preferred working alongside their mentor coupled with time for discussion (Chien et al., 2016).
Sites in Zambia established a mentorship program for PMTCT and PEDS with overall implementation improvements. Of interest, despite structural gains in the implementation of a clinical mentorship program, declines in competencies were noted. Also, facilities had the largest staff change during the knowledge assessment. These results highlight potential workforce challenges, such as retention and staff turnover, while implementing clinical mentorship and quality improvement programs. This can result in attrition of mentors or newly trained nurses and midwives. Past studies on mentorship evaluations in Malawi and Nigeria reported insufficient staffing for both mentorship and provision of care, which resulted in low availability to support mentees (Chien et al., 2016; Okereke et al., 2015). A more in-depth analysis is needed to understand the complexities of human resources for health and programmatic factors related to clinical mentorship and improved provider competencies.
This study had several limitations, including the use of a convenience sample, an inability to determine which participants participated in both pre- and posttest knowledge assessments, small sample size with no statistical power, and no outcome data on mentee satisfaction, improved quality of care, patient outcomes, or cost-effectiveness. Also, there was the potential for expectancy and social desirability bias during interviews with supervisors and managers on facility-level program maturation.
ConclusionThe ARC quality improvement initiative provided a useful framework to evaluate integration of quality nursing care into HIV service delivery. The NPF allows for a rapid assessment to identify trends and observations at the site level. Competency assessments linked to the framework can identify on-going needs for clinical practice and highlight staffing trends such as retention and attrition. Strengthening clinical mentorship programs may also require a design that incorporates health workforce data that includes role transitions and attrition; these data inform polices and investments to strengthen the nursing workforce as recommended in the State of the World's Nursing report 2020 (WHO, 2020). Addressing workforce challenges can facilitate an evaluation of more specific structural changes needed to sustain a cadre of mentors as NIMART expansion continues for many countries. Future analyses to effectively tailor mentorship to specific clinical areas would be stronger by incorporating the perspectives of nurses and midwives about their working conditions, learning environment, resource availability, and mentor accessibility. Sustained, high-quality HIV services delivered by nurses and midwives on the frontlines are essential to improve the well-being of women, infants, and children.
DisclaimerThe findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the funding agencies.
DisclosuresThe authors report no real or perceived vested interest related to this article that could be construed as a conflict of interest.
Author ContributionsAll authors on this paper meet the four criteria for authorship as identified by the International Committee of Medical Journal Editors; all authors have contributed to the drafting or been involved in revising it, reviewed the final version of this manuscript before submission, and agree to be accountable for all aspects of the work.
Specifically, using the CRediT taxonomy, the contributions of each author is as follows: Conceptualization of study design: C. Drayton, S.A. Spangler, and J. Gross; Data collection and management: S.A. Spangler, M. Mukenge, A. Waudo, T. Lipato; Data analysis and interpretation: C. Drayton and M. Robinson; Original manuscript draft: C. Drayton; Critical review and revisions: all coauthors. All coauthors reviewed and approved the final manuscript.Key Considerations The NPF demonstrated that each country team was able to develop and implement a clinical mentorship program at select high volume sites providing HIV specific care for the maternal, infant, and/or child population(s). HIV care for newborns and the pediatric population appears to be an area in need of on-going support for nurses and midwives because this is a highly specialized area. Multiple factors related to workforce challenges and resources can be explored with the NPF as a way to further advocate for the needs of nurses and midwives providing HIV care in maternal child nursing.
AcknowledgmentsThis research has been supported by the President's Emergency Plan for AIDS Relief (PEPFAR) through the Centers for Disease Control and Prevention (CDC) and the Public Health Institute under the terms of a Cooperative Agreement numbers 1U36OE000002 and NU2GGH002093-01-00. The authors acknowledge Michelle Dynes for her role in the development of the quantitative and qualitative facility assessment tools, and Jill Iliffe, Agnes Waudo, and Alphonce Kalula for the technical support they provided to ARC country teams, and Agnes Waudo and Nancy Ruto for their leadership in organizing and coordinating regional learning convenings. They also acknowledge Ken Hepburn for his leadership and thought partnership throughout the project and all members of the ARC country teams for their expertise and dedication to this program. They also thank Melinda Higgins for data analysis consultation.
References Chien E., Phiri K., Schooley A., Chivwala M., Hamilton J., Hoffman R. M. (2016). Successes and challenges of HIV mentoring in Malawi: The mentee perspective. Plos One, 11(6), e0158258. https://doi.org/10.1371/journal.pone.0158258 Goosby E., Von Zinkernagel D., Holmes C., Haroz D., Walsh T. (2012). Raising the bar: PEPFAR and new paradigms for global health. JAIDS Journal of Acquired Immune Deficiency Syndromes, 60(Suppl 3), S158-S162. https://doi.org/10.1097/QAI.0b013e31825d057c Gross J. M., McCarthy C. F., Verani A. R., Iliffe J., Kelley M. A., Hepburn K. W., Higgins M. K., Kalula A. T., Waudo A. N., Riley P. L. (2018). Evaluation of the impact of the ARC program on national nursing and midwifery regulations, leadership, and organizational capacity in East, Central, and Southern Africa. BMC Health Services Research, 18(1), 406. https://doi.org/10.1186/s12913-018-3233-4 International Training and Education Center for Health (2008, June). The I-TECH Approach to Clinical Mentoring. https://www.go2itech.org/HTML/CM08/toolkit/overview/index.html MacKay R. E., Gross J. M., Hepburn K. W., Spangler S. A., Spangler S. A. (2020). Nurse- and midwife-led HIV services in eastern and southern Africa: Challenges and opportunities for health facilities. The Journal of the Association of Nurses in AIDS Care: JANAC, 31(4), 392-404. https://doi.org/10.1097/JNC.0000000000000176 Manzi A., Mugunga J. C., Nyirazinyoye L., Iyer H. S., Hedt-Gauthier B., Hirschhorn L. R., Ntaganira J. (2019). Cost-effectiveness of a mentorship and quality improvement intervention to enhance the quality of antenatal care at rural health centers in Rwanda. International Journal for Quality in Health Care, 31(5), 359-364. https://doi.org/10.1093/intqhc/mzy179 McCarthy C. F., Kelley M. A., Verani A. R., St Louis M. E., Riley P. L. (2014). Development of a framework to measure health profession regulation strengthening. Evaluation and Program Planning, 46, 17-24. https://doi.org/10.1016/j.evalprogplan.2014.04.008 Michaels-Strasser S., Smith J., Khanyola J., Sutton R., Price T., El Sadr W. M. (2018). Strengthening the quality and quantity of the nursing and midwifery workforce: Report on eight years of the NEPI project. Annals of Global Health, 84(1), 31. https://doi.org/10.29024/aogh.6 Okereke E., Tukur J., Aminu A., Butera J., Mohammed B., Tanko M., Yisa I., Obonyo B., Egboh M. (2015). An innovation for improving maternal, newborn and child health (Mnch) service delivery in Jigawa State, northern Nigeria: A qualitative study of stakeholders' perceptions about clinical mentoring. BMC Health Services Research, 15(1), 64. https://doi.org/10.1186/s12913-015-0724-4 World Health Organization (2016). Global Strategic Directions for Strengthening Nursing and Midwifery (pp. 56). https://www.who.int/publications/i/item/9789241510455 World Health Organization (2020). State of the world's nursing 2020: Investing in education, jobs, and leadership. https://www.who.int/publications/i/item/9789240003279 Zuber A., McCarthy C. F., Verani A. R., Msidi E., Johnson C. (2014). A survey of nurse-initiated and -managed antiretroviral therapy (Nimart) in practice, education, policy, and regulation in east, central, and southern Africa. The Journal of the Association of Nurses in AIDS Care: JANAC, 25(6), 520-531. https://doi.org/10.1016/j.jana.2014.02.003
Comments (0)