
Remember me



Calcaneal fractures comprise between 2% and 3% of all fractures and are among the most common fractures involving the major tarsal bones.1,2 Calcaneal fractures most often result from high-energy injuries and often involve a young labor-intensive population.3
These fractures can be devastating, life-altering events for patients, with long recovery periods and permanent loss of function.4 The optimal treatment of calcaneus fractures has been a topic of ongoing debate with controversies regarding the best treatment options and algorithms.5
The most adopted management is open reduction internal fixation (ORIF), utilizing the extensile lateral approach6–9; emerging options include a limited sinus tarsi approach with ORIF, percutaneous fixation with or without arthroscopy, external fixation, primary subtalar arthrodesis, and nonoperative management.6,10–15 While the aforementioned surgical interventions have their differences, each are utilized to: (1) restore the height, length, width, and alignment of the calcaneus; (2) correct the disrupted relationship of the tuberosity to the subtalar joint; and (3) to restore the congruence of the subtalar facet joint surfaces. The goals of treatment include improvement of pain on ambulation, ability to wear normal shoes, return to work, and avoidance of major surgical complications.8,16
While there are references for the utilization of external fixation for the treatment of calcaneus fractures, there are few papers that examine the role of external fixation in the maintenance of bony alignment from time of initial reduction (application of external fixation) to definitive surgery or utilizing external fixation as the definitive and sole surgical management.
This retrospective analysis comprises 26 patients (28 calcaneal fractures) treated in a level I trauma teaching hospital over the period of 7 years (from April 2004 to May 2011). We utilized a 3-pin medially based external fixator placed at the initial surgery for the treatment of selected patients with high-energy displaced intra-articular calcaneus fractures. We describe the surgical technique with a focus upon anatomic landmarks of pin placement and the areas of concern involved in the application of a 3-pin external fixation for the temporary or definitive distraction of intra-articular calcaneal fractures. The purpose of this study is to evaluate the role of provisional external fixation in the management of calcaneal fractures. Our radiographic measurements of key anatomic features of the calcaneus before and after definitive fixation and at the end of external fixation management (inclusive of complications over a mean duration of 26.3 mo) are reported and analyzed.
INDICATIONS AND CONTRAINDICATIONSIndications for calcaneal external fixation in this study include initial treatment of open or closed comminuted joint depression fractures of the calcaneus with prominent soft tissue swelling or compromise. Radiographic imaging assessment include plain radiographs and/or computed tomography (CT) scans showing flattening of Böhler angle, loss of calcaneal height, and hindfoot varus deformity (Figs. 1, 2).
 FIGURE 1:
FIGURE 1: Preoperative plain x-ray showing flattening of Böhler angle, loss of calcaneal height, and hindfoot varus deformity of the injured side joint depression calcaneus fracture.
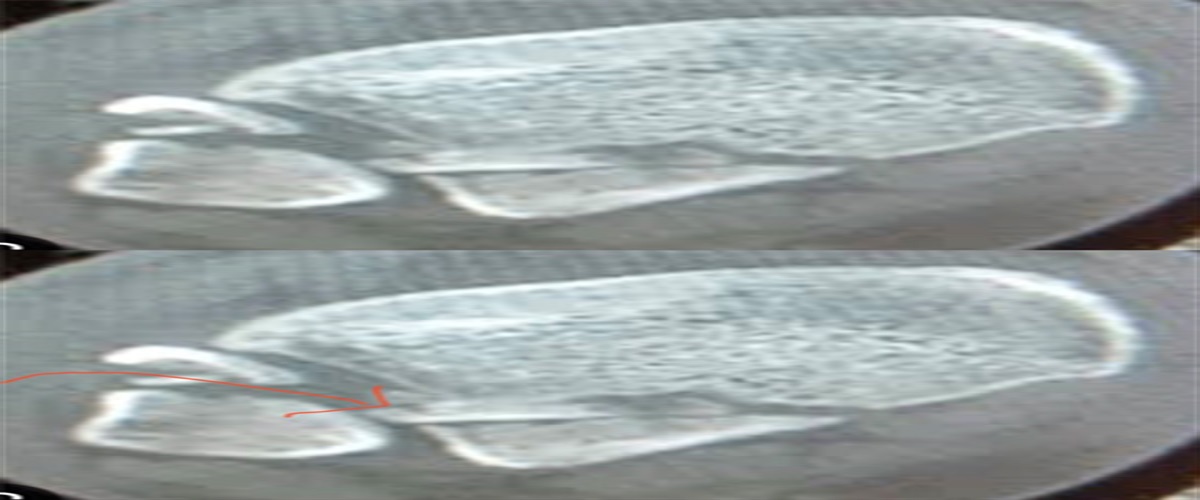
 FIGURE 2:
FIGURE 2: Preoperative computed tomography showing Sanders III intra-articular calcaneus fracture with posterior facet depression, comminution (A and B), loss of calcaneal height (B), and hindfoot varus deformity (C).
To be noted, the decision of operative versus nonoperative management was also made based on the surgeon’s overall consideration of the patient’s risk factors, including but not limited to age, fracture type, associated comorbidities, and injury pattern. There were 3 surgeons who utilized this technique during the time of this study. The goals for using this closed external fixation technique are to (1) restore alignment, length, and height of the calcaneal morphology; (2) reestablish proper tension to the skin integument during resolution of lymphatic engorgement and edema which results from displaced and angulated fragments; and (3) to provide a better alternative than nonoperative management altogether in the nonsurgical candidate.
Contraindications included skeletal immaturity with an incompletely ossified calcaneus, chronic foot ulcers, and nondisplaced fractures with good articular congruency. Smoking, diabetes, and open fractures were not considered contraindications in our cohort.
PREOPERATIVE PLANNINGLateral calcaneus and Harris axial views of the injured and noninjured sides were obtained preoperatively for surgical planning. CT scans were obtained to improve understanding the fracture patterns in all cases.
All external fixation (for closed and open calcaneus fractures) were performed urgently or emergently.
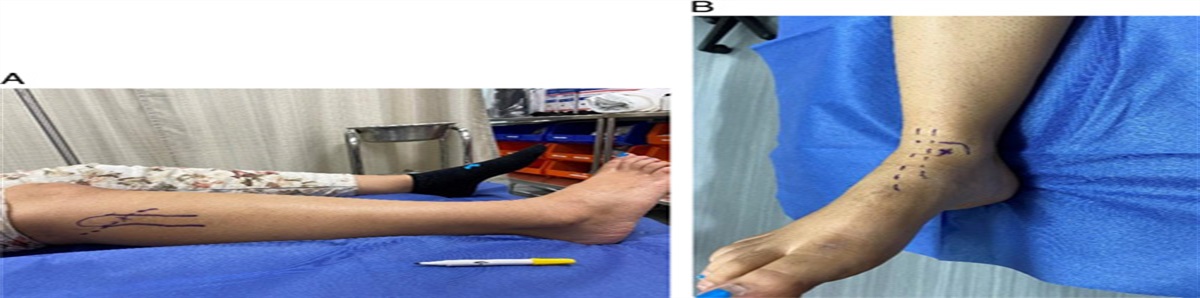
TECHNIQUEThe patient is positioned floppy lateral decubitus on the operating table. Using preoperative radiographs of the uninjured hindfoot, the surgeon aims to reproduce anatomic alignment of the calcaneus via fracture fragment distraction and ligamentotaxis. Application of pins start with a terminally threaded, self-drilling Schanz pin of 5 mm thickness placed from medial to lateral at the calcaneal tuberosity within the safe zone; this allows for a reduction to take place, drawing the deformed calcaneus out of its typical varus position (Fig. 3).
 FIGURE 3:
FIGURE 3: Intraoperative imaging of medially based 3-pin external fixation construct showing restored calcaneal height, length, Böhler angle, and out of varus deformity plus the fourth pin from the posterior superior of tuberosity to the under the surface of the depressed posterior facet for reduction of joint depression with Essex-Lopresti Maneuver.
It is important that the pin is perpendicular to the tuber calcaneus, as it is often in varus and needs correction. The pin is advanced to the far cortex of the calcaneus, and its position should be verified with C-arm fluoroscopy. A second 5 mm Schanz is then placed into the medial distal tibia approximately proximal to the fibular incisura. This pin is placed from medial to lateral, parallel to the joint line and perpendicular to the anatomic axis of the tibia. It should be placed bicortically, with the position being verified using C-arm fluoroscopy. The foot is then placed into an oblique position with the knee flexed. A 4 mm Schanz pin is then placed into the base of the first metatarsal (or medial cuneiform). This too should be placed bicortically and verified with C-arm fluoroscopy.
A fourth pin is added in the case of the tongue-type variant. This is inserted from the posterior superior corner of the calcaneal tuberosity towards the lateral and inferior portion of the depressed posterior facet. The Essex-Lopresti Maneuver is utilized to reduce the varus deformity and disimpact the posterior facet joint16 (Figs. 3, 4).
 FIGURE 4:
FIGURE 4: Postoperative computed tomography showing restored calcaneal length, height, and reduced posterior facet depression and tongue-type fragment.
At this time, the external fixator bars and clamps should be applied to prepare for the reduction maneuvers. Different manufacturers may provide different benefits, but the principles remain the same. The benefits of expandable tubes are the allowance of the distraction to be titrated to the desired reduction and the ease of manipulation after tightening of the joints (Fig. 5).
 FIGURE 5:
FIGURE 5: Medially based calcaneal fracture external fixation with distraction tubes and pin to bar kick stand after provisional reduction.
First, the distracting tubes should be placed from the tibial pin to the calcaneal pin to restore proper height. It is paramount to reduce the calcaneal tube alignment, which is most often in varus during this aspect of the procedure. A second tube is then placed from the calcaneal pin to the first metatarsal or medial cuneiform pin for distraction to provide length; intraoperative lateral and Harris axial views should then be used to verify restoration of calcaneal height and correction of the varus positioning of the hindfoot.
The contralateral images should be used as templates for goals of reduction. Restoration of calcaneal height, length, and neutral alignment are desired endpoints. Note, in most cases, the restoration a normal Böhler angle is nearly unattainable because of the impacted position into the tuber calcanei. Due to tenting, the skin at the insertion pin sites must be relaxed with an incision at the base after the correction. A third bar is then placed from the tibia to the first metatarsal Schanz pin to capture and stabilize the reduction while providing a plantigrade foot. At this point, the pins can be dressed with Xeroform, 4×4 sponges, and anchoring clips to complete the surgical procedure. A pin to bar kickstand can be added if the fourth pin is used at the posterior hindfoot for reduction of posterior facet joint depression.
CLINICAL CASE SERIESThis study was approved by our institutional review board to retrospectively review consecutive patients with intra-articular calcaneus fractures treated with the application of a medial multiplanar external fixator with subsequent removal (± conversion to ORIF). Over a period of 7 years (between April 2004 and May 2011), a cohort of 26 patients with 28 fractures were identified and reviewed (Table 1). The mean time from injury to the application of an external fixator was 4.5 days (SD±6.2).
TABLE 1 - Patient Demographics Variables Frequency (N=26) [n (%)] Fracture cases 28 Age [mean (range)] (y) 43.6 (20-80) Sex (male) 24 (92) Injury mechanism Fall from height 18 (69.2) Motor vehicle accident 8 (30.8) Injury, closed (open) 20 (8) Follow-up time [mean (range)] (mo) 26.3 (1.5-93.8) Smoker 13 (50.0) Diabetes 2 (7.7) Peripheral vascular disease 0 (0) ORIF definitive management 16 Non-ORIF definitive management 12 Essex-Lopresi fracture pattern Joint depression 22 (78.6) Tongue type 2 (7.1) Depression and tongue 4 (14.3) Sanders fracture pattern Type 2 1 (3.6) Type 3 14 (50.0) Type 4 13 (46.4)ORIF, open reduction internal fixation.
All patients included in this study are adults (age 20 to 82 y old) with open or closed intra-articular calcaneal fractures with nonpathologic conditions and direct results of trauma. Patient radiographs were reviewed by the senior author (P.A.C.) and 2 fellowship-trained orthopedic traumatologists using images from our institutional picture archiving and communication system (PACS). Measurements were taken at the time of injury, after the application of external fixation, at first follow-up after application of external fixator (5 to 20 d), and at the time of removal of the external fixator—whether that be conversion to ORIF or removal of external fixator after bony healing in the context of closed management. In addition, radiographic images of the contralateral calcaneus were taken as a basis for comparison. Specifically, lateral and Harris axial views were performed at all time points, and Böhler angle and calcaneal varus angles were measured.
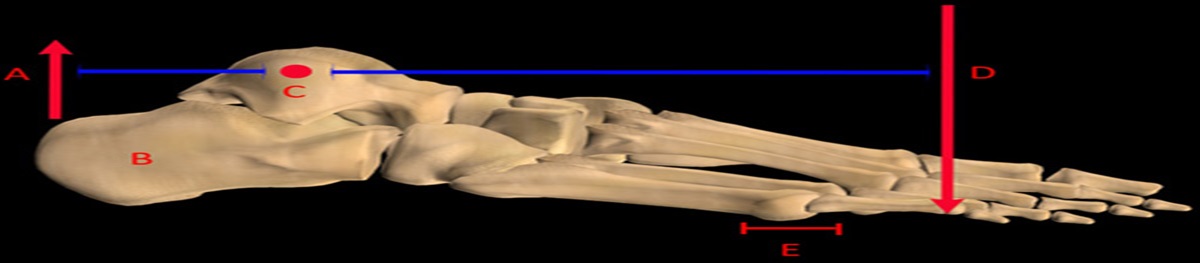
Böhler angle was defined as the intersection of the line drawn along the upper contour of the tuberosity—the line drawn from the highest point of the anterior process to the highest point of the posterior articular surface17 (Fig. 6). To describe calcaneal varus angulation, we used the Harris axial images and measured calcaneal tuber-varus angulation via the angle created through the intersection of a line tangent to the medial wall of the calcaneus with the line tangent to the turning slope of the sustentaculum tali (identified with consistency in all cases) (Fig. 7).
 FIGURE 6:
FIGURE 6: Böhler angle measured 20 degrees after reduction and placement of medial-based external fixation.
 FIGURE 7:
FIGURE 7: Tuber varus angle measurement as the angle at the intersection of the line tangent to the turning slope of the medial surface of the sustentaculum tali and the line tangent to the medial wall of the calcaneal tuberosity. Tuber-varus angle of 13 degrees was measured in this case.
Fracture patterns were classified using the Sanders classification system via CT imaging.18 Sixteen patients had contralateral imaging; the measurements at the described time points were compared with the corresponding measurement taken on the contralateral side to assess the quality of the anatomic reduction (defined as both calcanei equal measurement). In addition, the measurements taken immediately after the application of the external fixator were compared with the same measurements taken at the first follow-up after the application of that external fixator. In this way, we were able to assess whether the external fixator maintained alignment over time. Using descriptive statistics, the mean change across the total patient population between the following measurements were performed: (1) the difference between initial external fixator application measurement and contralateral side measurement, (2) change between definitive fixation measurement and contralateral side measurement, (3) change between initial application external fixator measurement and definitive fixation measurement, and (4) the change between initial application external fixator measurement and first follow-up after application of that external fixator. For patients without contralateral imaging, a comparison of their individual measurements was made to the literature accepted measurement values (Böhler angle of 25 to 40 degrees).17,19 Utilizing the accepted measurement values, reductions could be assessed to be in the anatomic zone. In addition, patient’s records were reviewed to identify and record complications after surgery.
RESULTSOf the 26 patients deemed eligible for this study, 2 had bilateral calcaneus fractures, for a total of 28 calcaneus fractures enrolled in this study (Table 1).
The majority of patients were male (24 males; 2 females), with an average age at the time of injury of 43.6 years (range: 20 to 82 y). Of the 28 fractures, 14 were right-sided injuries, and 14 were left. Eight were open fractures, and 20 were closed. In terms of patient comorbidities, there were 2 diabetic patients (7.7%), 13 smokers (50%), and 0 (0%) with known peripheral vascular disease.
The mechanism for all injuries was high-energy impact trauma. Eighteen patients (69.2%) sustained their injuries due to a fall from height, while the remaining 8 patients (30.8%) sustained their injuries in motor vehicle accidents. Twenty-two (78.6%) were Essex-Lopresti joint depression type, 2 (7.1%) were Essex-Lopresti tongue type, and 4 (14.3%) cases were combined joint depression and tongue type of fracture. With Sanders CT-based classification, 1 (3.6%) was type II, 14 (50%) were type III, and 13 (46.4%) cases were type IV calcaneus fractures.
External fixator constructs were constructed using 3 hospital-contracted vendor systems with similar configurations and mechanisms: 13 Synthes (Synthes), 14 Hoffman II (Stryker), and 1 Zimmer (Zimmer). The external fixators were in place for an average of 6.3 weeks in the group that had definitive management with the external fixation and 2.6 weeks (range: 0.4 to 5.7 wk) in the group that underwent subsequent ORIF. For 12 of the fractured calcanei, the external fixation was the definitive management for their injury, while 16 calcanei went on to receive ORIF with an extensile lateral approach. In addition, 3 cases required flap coverage, and 7 cases required serial irrigation and debridement for the open fracture.
Böhler angle and the tuber-varus angle during the course of treatment are demonstrated in Tables 2 and 3 (external fixator group and ORIF conversion group, respectively). There was no significant loss of Böhler angle in the patients managed definitively with external fixation (P=0.44) or those managed with subsequent ORIF (P=0.51) during the course of treatment with the external fixator (Figs. 8, 9). In addition, there was no significant loss of tuber-varus angle in either group (P=0.89 and 0.94) during the course of external fixation.
TABLE 2 - Böhler Angle and Varus Angulation During Course of Treatment in the Definitive External Fixation Group Measurement [Mean (±SD)] (deg.) Interval Böhler Angle Tuber-Varus Angulation Initial injury 17.3 (±12.5) 29.7 (±13.5) Initial external fixator 18.7 (±9.4) 14.4 (±9.8) Final external fixator 15.3 (±11.0) 15.0 (±10.0) Final follow-up 8.7 (±11.8) 14.4 (±9.1)ORIF, open reduction internal fixation.
 FIGURE 8:
FIGURE 8: External fixation to open reduction internal fixation (ORIF) group. Demonstrates no significant loss of Böhler angle (P=0.51) or tuber-varus angulation (P=0.94) during the course of external fixation or during the period after ORIF to final follow-up (P=0.09 and 0.75, respectively).
 FIGURE 9:
FIGURE 9: External fixation only group. Demonstrates no significant loss of Böhler angle (P=0.51) or tuber-varus angulation (P=0.94) during the course of external fixation. However, there was a significant loss of Böhler angle (P=0.03), but not tuber-varus angulation (P=1.00) during the period of initial external fixation to final follow-up.
There was, however, a significant loss of Böhler angle (P=0.03) during the period of initial external fixation to final follow-up, as the initially obtained correction failed to maintain after the external fixation was removed.
COMPLICATIONSA total of 7 of 28 fractures exhibited signs of infection (superficial or deep) or wound dehiscence; 4 occurred in patients who had open injuries, and treatment was initiated before external fixation. Two complications were directly related to external fixation including a deep pin tract infection requiring formal irrigation and debridement in an open fracture and a superficial pin tract infection which was successfully managed with short-term oral antibiotics. There was 1 case of deep infection occurring after definitive ORIF. It was also managed with irrigation and debridement and intravenous antibiotics to resolution.
Four patients experienced local wound dehiscence. Of the 7 complications, 5 cases required to return to the operating room. Of those cases, 2 were solely for wound dehiscence, 2 were for patients with both pin tract infection and wound dehiscence, and 1 was solely for a pin tract infection. Of the reported cases with complications, there was only 1 patient who did not have significant comorbidities. Of the 4 patients that developed wound dehiscence, 1 was diabetic, and 2 were smokers. Of the 3 patients that developed a wound tract infection, 2 were smokers.
POSTOPERATIVE MANAGEMENTPostoperatively, pin sites were frequently observed daily to avoid pin tract infection. Showering was permitted with soap and water over the external fixation. Patients were instructed to elevate their injured leg on a foam positioner. Active and passive range of motion with toe stretching was instituted as soon as patients could tolerate it.
External fixation was kept on for an average of 7 weeks for those treated with definitive closed management. Upon removal, patients were progressed to weight-bearing as tolerated. In patients who went on to ORIF through the extensile lateral approach, the external fixation was removed and discarded.
POSSIBLE CONCERNS, FUTURE OF THE TECHNIQUEBased on the indications and individualized risk factors, intra-articular calcaneus fracture can be managed with the following options: (1) nonoperative management, (2) extensile approach ORIF, (3) minimally invasive reduction and fixation, and (4) primary subtalar arthrodesis.10 There has been much debate as to whether to operate or not in displaced, intra-articular calcaneal fractures due to the high risk of complications, especially with the extensile open approach.20,21 Multiple clinical studies have described operative treatment without significant benefit over closed management.8,18,22–30 However, in the last 3 decades, operative fixation is the commonly agreed management of displaced intra-articular calcaneus fractures in younger patient’s population, nonsmoker, nonworkers compensation patients, and those without heavy workloads.5,10,23,31–33 It is essential to achieve anatomic reduction and stable fixation for a desirable outcome.34 Properly performed ORIF (joint-first approach) to restore the overall shape and joint surfaces is necessary to achieve favorable long-term outcomes with minimal alterations in activities of daily living and work. However, those with initial severe joint destruction may likely need primary or future arthrodesis surgery.6–9,35
There continues to be substantial concern regarding the high complication rates associated with ORIF. Wound breakdown and infection remain the most concerning postoperative complications, reportedly from 0% in smaller sample studies to as high as 31% in some series.34,36–42 However, Benirschke and Kramer38 concluded that a properly done ORIF does not expose patients to undue risk of serious infection. Folk and Starr43 concluded that smokers, diabetics, and patients who sustained open fractures had an increased risk for wound complications after conventional ORIF through an extensile lateral incision technique. The condition of the soft tissue envelope is a critical factor in the determination of the fate of wound healing after surgical fixation. The typical soft tissue rest time from initial injury to definitive surgical fixation is usually around 10 to 14 days except for emergency surgery for tongue-type fractures with threatened posterior soft tissues or open fractures.29 As the time interval to definitive ORIF increases, however, fracture consolidation and soft tissue contracture make reduction more difficult. Some authors suggest that surgery should not be delayed beyond 14 days after initial injury; this may be associated with more postoperative soft tissue problems associated with tissue stretch after bony reduction.29,44
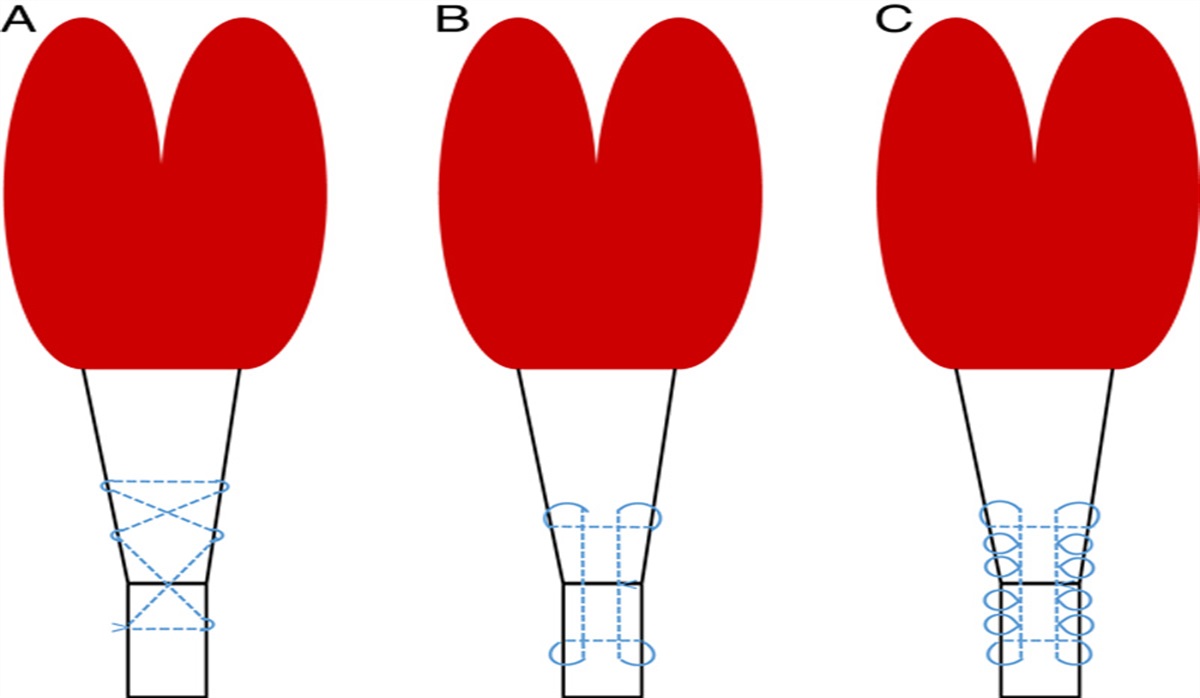
In this case series, we employed the use of a medially based 3-pin external fixator for intra-articular calcaneus fractures (fourth pin added in tongue-type variation), which relies on the surgeon’s attention to proper strategic pin placement and sequential reduction maneuvers. The deforming forces and complexity of the lateral vascularity of the calcaneus has made medial approaches to external fixation safe and optimal. Borrelli and Lashgari45 highlighted 3 major arteries of concern in the lateral calcaneal flap: the lateral calcaneal artery, the lateral malleolar artery, and the lateral tarsal artery. The lateral calcaneal artery was shown to be the most vulnerable and a key player in wound complications after surgical intervention in intra-articular calcaneal fractures.
The medially based frame also facilitates the lengthening of the calcaneal tuber as well as correcting the varus deformity through ligamentotaxis. When performing medial percutaneous pin placement in the calcaneus, one must be cautious to avoid disrupting the medial neurovascular bundle and the medial calcaneal nerve (which is considered the area of highest concern). Gamie et al46 described a “safe zone” for medial pin placement in the calcaneus. Using anatomic landmarks, he described the zone as being posterior to 75% of the distance of the lines bordered between the inferior tip of the medial malleolus and the posterior superior portion of the calcaneal tuberosity; the navicular tuberosity and the medial process of the calcaneal tuberosity; the inferior tip of the medial malleolus and the medial process of the calcaneal tuberosity; and, the navicular tuberosity and the posterior superior portion of the calcaneal tuberosity. Special attention must be placed on being aware of this “safe zone” to avoid neurovascular or sensory damage.
Baumgaertel and Gotzen47 reported on the use of a 2-stage medial external fixation protocol for the treatment of displaced intra-articular calcaneal fractures. The first stage utilized a 5-mm Schanz screw placed medially into the most posterior portion of the calcaneal tuber, followed by a second Schanz screw placed medially at right angles into the lower third of the tibia. The pins are percutaneously placed and then connected by an external fixation system. The second stage was carried out by removing the fixator and performing formal ORIF through a lateral approach. Similarly, Kuner et al48 reported their findings on 45 intra-articular calcaneal fractures treated with provisional medially based, 2 pin, external fixation. Similar to Baumgaertel and Gotzen, a medially based external fixator was placed temporarily while soft tissue swelling abated, allowing for definitive fixation using principles of ORIF. In their study, 71% of the 45 patients achieved very good and good results according to the Merle d’Aubigne scoring system. Magnan et al49 reported comparable clinical results and reduced risks to open reduction and internal fixation in their 54 cases of closed articular displaced calcaneal fracture with Sanders type II, III, and IV treated definitively with external fixation and percutaneous reduction in a 6-year follow-up period. Elgamal and colleagues described a temporary external fixator as an intraoperative aid in open reduction and internal fixation of intra-articular calcaneal fractures. The controlled distractive force harnessed provided improved exposure of the subtalar joint, correction of angulation, and maintenance of temporary stability before definitive fixation. Their construct of the 2-pin external fixator is laterally based.50
A very similar 2-stage approach to severely displaced calcaneus fracture was described by Githens et al51; the approach is characterized by closed reduction and medial-based calcaneal external fixation performed in a stepwise fashion to restore the calcaneal key anatomic alignments and maintain proper soft tissue envelop tension, which is a major contributing factor in wound healing complications in traditional delayed-fashion ORIF. It should be noted that open fractures were not included in their. However, as stated by the authors, they also adopted the technique based on Baumgaertel and Gotzen’s47 medial 2-pin technique with modification for both open and closed fractures. The series demonstrated favorable results on closed calcaneal fractures only.
We acknowledge the contributions of these previous studies in the development of our 3-pin technique. We believe that the addition of a third pin allows the distraction to maintain a correcting vector of varus deformity as well as lengthening that the 2-pin construct could not always accomplish. We believe the medial-based external fixation to be highly beneficial for patients with high risks for potential wound healing issues including open fractures and patient with risk factors like diabetes and smokers. Consistent with the findings from Baumgaertel and Gotzen47 and Githens et al51 our results showed safe, effective restoration of morphology and anatomic reduction of joint surfaces; thus, mitigating later difficulties and potential issues of malunion in both open and closed calcaneal fracture patients. Similar to Githens et al’s51 findings, Bohler angle restoration, and maintenance after removal were not satisfactory with our methods of external fixation. However, our results demonstrated reliable restoration of calcaneal height, length, and axial alignment out of varus.
Our 3-pin construct did not demonstrate the ability to disimpact the posterior facet joint depression, and therefore we added fourth pin as described as modified Essex Lopressti maneuver12,52 if a tongue-type variant with joint depression at subtalar posterior facet was present. When the resolution of soft tissue swelling was acceptable for surgical intervention, we proceeded with an extensile lateral approach for definitive fixation for our cases. The exception were cases with residual high risks factors or severe polytrauma situations preventing from timely management of calcaneus fracture. In those cases, external fixation was opted for definitive management.
The current practice of utilizing a bulky Jones-type resting splint does not address issues of fracture consolidation and soft tissue contracture. There are a few previous reports in the literature regarding the use of provisional external fixation for displaced intra-articular calcaneal fractures. Borowsky53 presented a case report of 2 patients treated with ORIF with medial external fixator placement used for indirect reduction. In this case report, external fixation was performed at the time of definitive surgery. The authors concluded that medial external fixation is effective in correcting the middle facet area, which was not attainable with the standard lateral extensile approach. Furthermore, they postulated that the medial reduction had the ability to prevent the need for major open reduction from the lateral side by reducing key fragments initially blocking reduction.
Schwartsman and Schwartsman54 reported their technique of reduction using an Ilizarov frame for calcaneal fractures. Similar techniques have been reported by Paley and Hall55 and McGarvey et al,56 in which definitive fixation was carried out with the use of a thin wire hybrid Ilizarov frame to restore subtalar joint congruity, calcaneal height, length, and neutral alignment. These studies demonstrated that this technique achieves satisfactory anatomic restoration of the calcaneus (in particular the subtalar joint), while giving the benefits of shorter time to surgery, decreased invasiveness, earlier weight-bearing (desensitization of the footpad for deceased heel pain).
Minimally invasive techniques have also been explored over the last few decades.15,16,57–66 These techniques have shown evidence to be advantageous for patients that have early threats to the skin and other risk factors but require reduction and fixation. However, minimally invasive techniques are technically demanding, require the use of intraoperative image intensifiers and small incisions to place tools for proper reduction, and are typically limited to by timeframes beyond 14 days (as anatomic reduction becomes harder as healing progresses).
Our results show that adequate reduction can be obtained and maintained with a medially based, 3-pin construct with one pin placed in the tibial metaphysis, one placed in the calcaneal tuber, and a third placed in the medial column (either in the first metatarsal or the medial cuneiform). This construct allows for multiplanar correction in a way that a 2-pin fixator cannot. The construct is capable of restoring length, height, and varus/valgus alignment to the calcaneus. In addition, the medially placed pins preserve soft tissue envelop, especially the lateral soft tissues for a future limited or open approach utilizing the extensile approach first described by Stephenson,67 then later modified by Benirshke and Sangeorzan.23
Overall, the medially placed 3-pin (4 pin in displaced tongue-type fracture) external fixation construct has the advantage of placing soft tissues at rest in a more anatomic position to improve lymphatic drainage—similar to external fixation in pilon and plateau fractures. Our construct places skin at native resting length rather than allowing the skin to contract over the site (which later must be stretched for the reduction). With the external fixation construct placed urgently, it allows time for further evaluation of the patient’s healing potential, amenability to postsurgical care, and improves heel tuber position in the event of nonoperative treatment in the poor surgical candidate.
However, it is important to acknowledge the rather minimal improvement and maintenance of correction in Böhler angle after frame removal. We considered that in most calcaneal fractures with joint depression, the facet is driven down and rotated forward. Therefore, pulling on the tuber does not change the direction of the facet, even though it yields height through stretching of the Achilles tendon. Thus, even minimal improvement in Böhler angle is important. A fourth pin addition with Essex-Lopresti maneuver will be useful in the provisional or definitive reduction and fixation. A similar conclusion was seen also from the report of Githens et al51 with a 3-pin medially based external fixation construct.
Limitations of this study include single surgeon experience, relatively small numbers of cases, and lack of a comparative cohort. However, decisions on operative versus conservative treatments for intra-articular calcaneus fractures were not our primary concern in this study. To that end, Sutherland’s Cochrane review addresses such questions.13 The present study instead sought to detail a surgical method that is both safe and effective.
In summary, intra-articular fractures of the calcaneus are devastating injuries resulting from high-energy trauma. We have described a technique for provisional placement of a medial-based 3-pin (or 4 pin) construct via the method described herein, which has been used efficaciously with minimal complications in our cohort of patients. The technique provides initial reduction and alignment maintenance while preserving the soft tissue envelope before definitive surgery.
REFERENCES 1. Lance EM, Carey EJ, Wade PA. Fractures of the os calcis: treatment by early mobilization. Clin Orthop Relat Res. 1963;30:76–90. 2. O’Connell F, Mital MA, Rowe CR. Evaluation of modern management of fractures of the os calcis. Clin Orthop Relat Res. 1972;83:214–223. 3. Sanders R. Current concepts review-displaced intra-articular fractures of the calcaneus. J Bone Joint Surg. 2000;82:225–250. 4. Tufescu TV, Buckley R. Age, gender, work capability, and worker’s compensation in patients with displaced intraarticular calcaneal fractures. J Orthop Trauma. 2001;15:275–279. 5. Thordarson DB, Krieger LE. Operative vs. nonoperative treatment of intra-articular fractures of the calcaneus: a prospective randomized trial. Foot Ankle Int. 1996;17:2–9. 6. Buckley R, Tough S, McCormack R, et al. Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: a prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am. 2002;84:1733–1744. 7. Ågren P-H, Mukka S, Tullberg T, et al. Factors affecting long-term treatment results of displaced intraarticular calcaneal fractures: a post hoc analysis of a prospective, randomized, controlled multicenter trial. J Orthop Trauma. 2014;28:564–568. 8. Sanders R, Vaupel ZM, Erdogan M, et al. Operative treatment of displaced intraarticular calcaneal fractures: long-term (10–20 years) results in 108 fractures using a prognostic CT classification. J Orthop Trauma. 2014;28:551–563. 9. Buckley R, Leighton R, Sanders D, et al. Open reduction and internal fixation compared with ORIF and primary subtalar arthrodesis for treatment of Sanders type IV calcaneal fractures: a randomized multicenter trial. J Orthop Trauma. 2014;28:577–583. 10. Sharr P, Mangupli M, Winson I, et al. Current management options for displaced intra-articular calcaneal fractures: non-operative, ORIF, minimally invasive reduction and fixation or primary ORIF and subtalar arthrodesis. A contemporary review. Foot Ankle Surg. 2016;22:1–8. 11. Sivakumar BS, Wong P, Dick CG, et al. Arthroscopic reduction and percutaneous fixation of selected calcaneus fractures: surgical technique and early results. J Orthop Trauma. 2014;28:569–576. 12. Essex-LoPresti P. The mechanism, reduction technique, and results in fractures of the os calcis. Br J Surg. 1952;39:395–419. 13. Bruce J, Sutherland A. Surgical versus conservative interventions for displaced intra-articular calcaneal fractures. Cochrane Database Syst Rev. 2013;1:CD008628. 14. DeWall M, Henderson CE, McKinley TO, et al. Percutaneous reduction and fixation of displaced intra-articular calcaneus fractures. J Orthop Trauma. 2010;24:466–472. 15. Kikuchi C, Charlton TP, Thordarson DB. Limited sinus tarsi approach for intra-articular calcaneus fractures. Foot Ankle Int. 2013;34:1689–1694. 16. Tornetta P III. The Essex-Lopresti reduction for calcaneal fractures revisited. J Orthop Trauma. 1998;12:469–473. 17. Böhler L. Diagnosis, pathology, and treatment of fractures of the os calcis. J Bone Joint Surg. 1931;13:75–89. 18. Sanders R, Fortin P, DiPasquale T, et al. Operative treatment in 120 displaced intraarticular calcaneal fractures. Results using a prognostic computed tomography scan classification. Clin Orthop Relat Res. 1993;290:87–95. 19. Su Y, Chen W, Zhang T, et al. Bohler’s angle’s role in assessing the injury severity and functional outcome of internal fixation for displaced intra-articular calcaneal fractures: a retrospective study. BMC Surg. 2013;13:40. 20. Rammelt S, Sangeorzan BJ, Swords MP. Calcaneal fractures—should we or should we not operate? Indian J Orthop. 2018;52:220–230. 21. Rammelt S, Zwipp H. Fractures of the calcaneus: current treatment strategies. Acta Chir Orthop Traumatol Cech. 2014;81:177–196. 22. Makki D, Alnajjar HM, Walkay S, et al. Osteosynthesis of displaced intra-articular fractures of the calcaneum. J Bone Joint Surg Br. 2010;92-B:693–700. 23. Benirschke SK, Sangeorzan BJ. Extensive intraarticular fractures of the foot. Surgical management of calcaneal fractures. Clin Orthop Relat Res. 1993;292:128–134. 24. Potter MQ, Nunley JA. Long-term functional outcomes after operative treatment for intra-articular fractures of the calcaneus. J Bo
Comments (0)