
Remember me
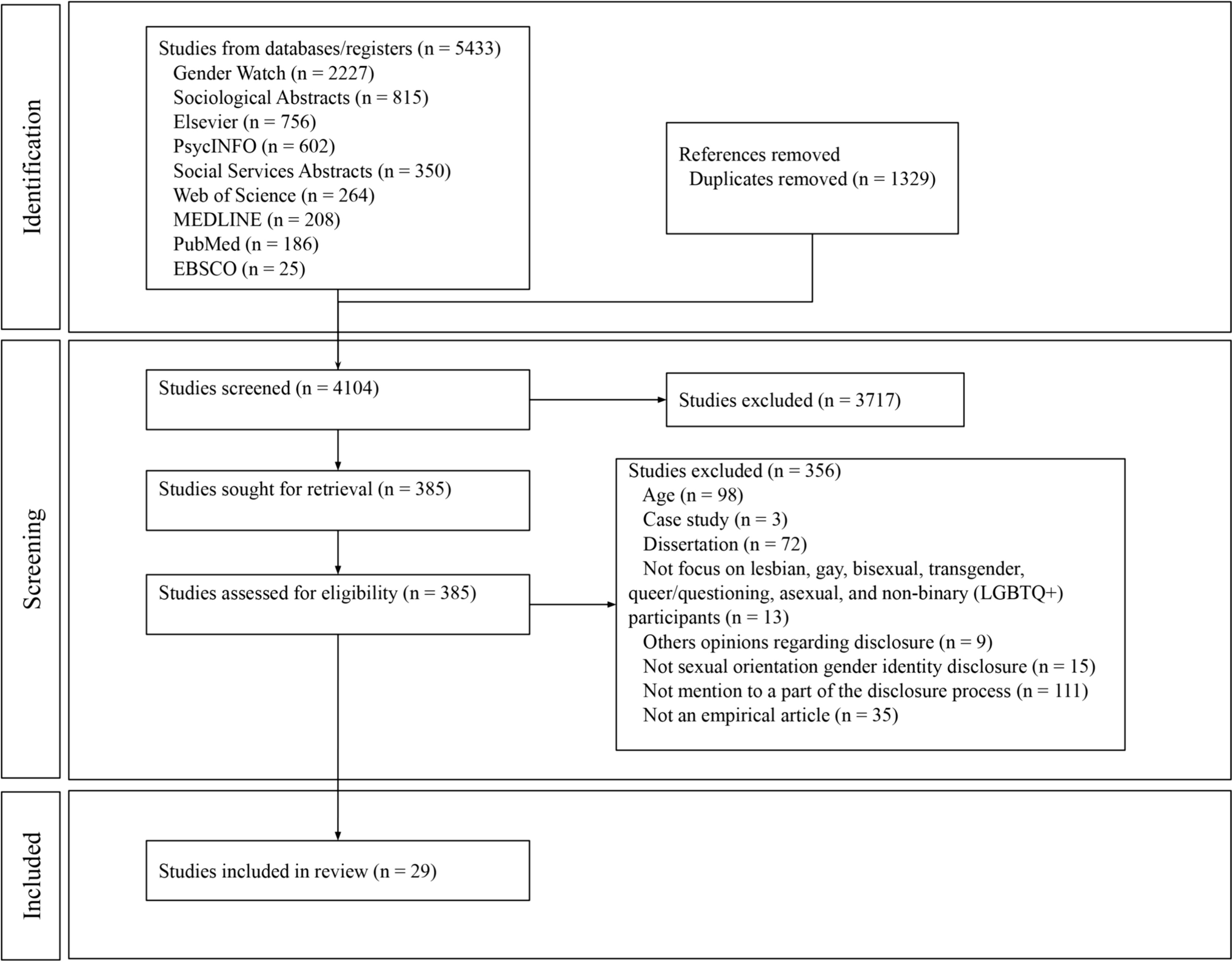
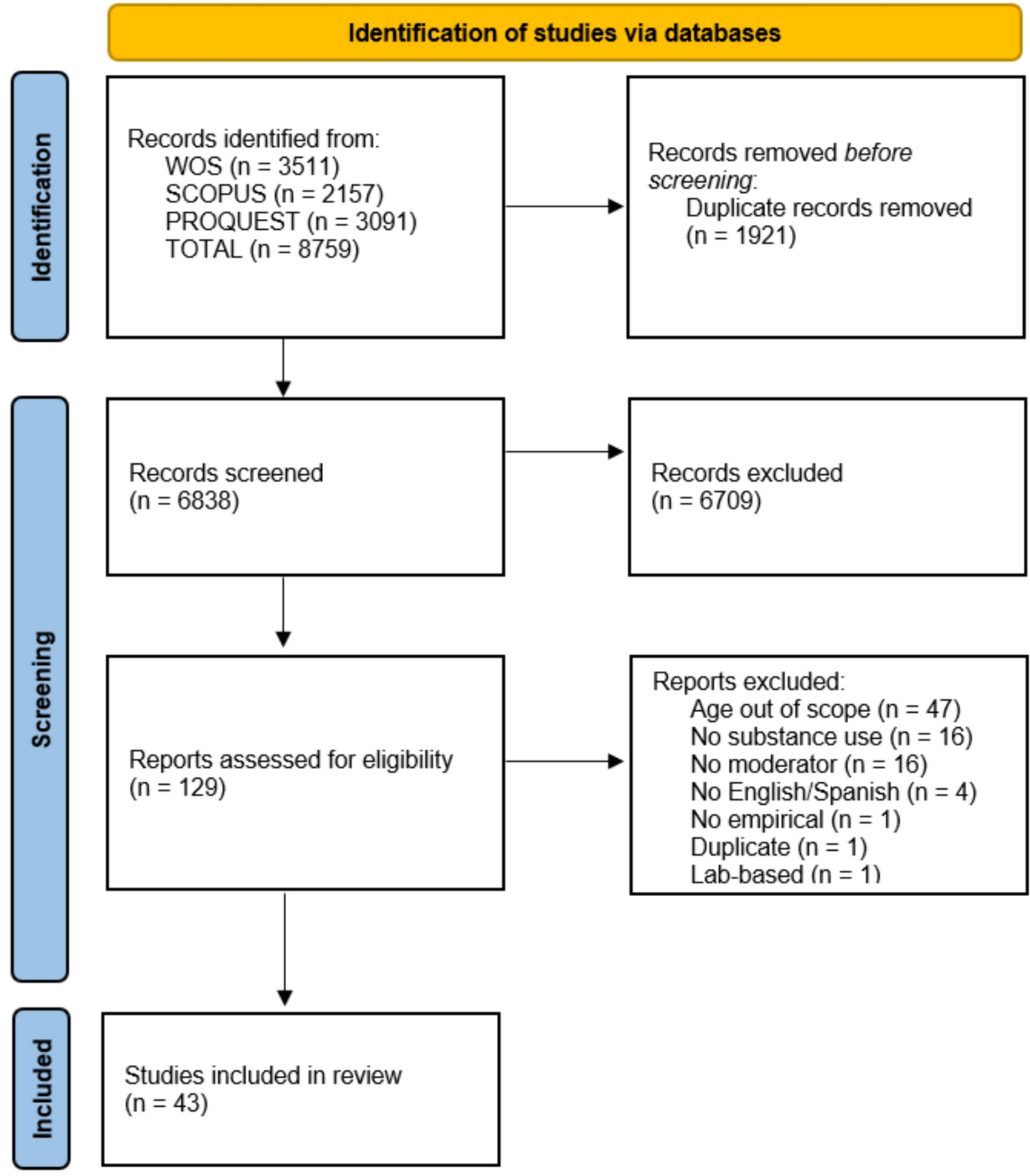
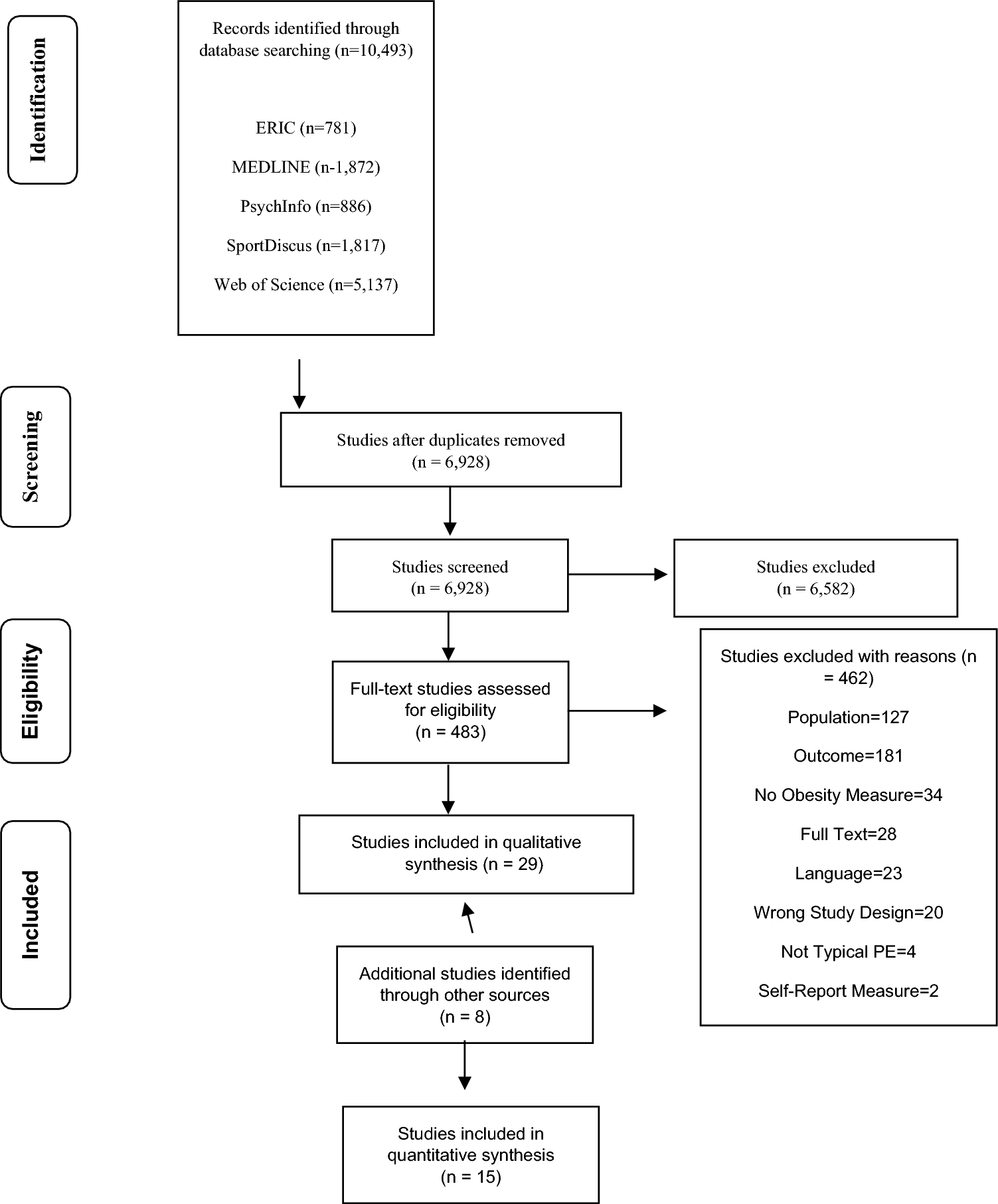
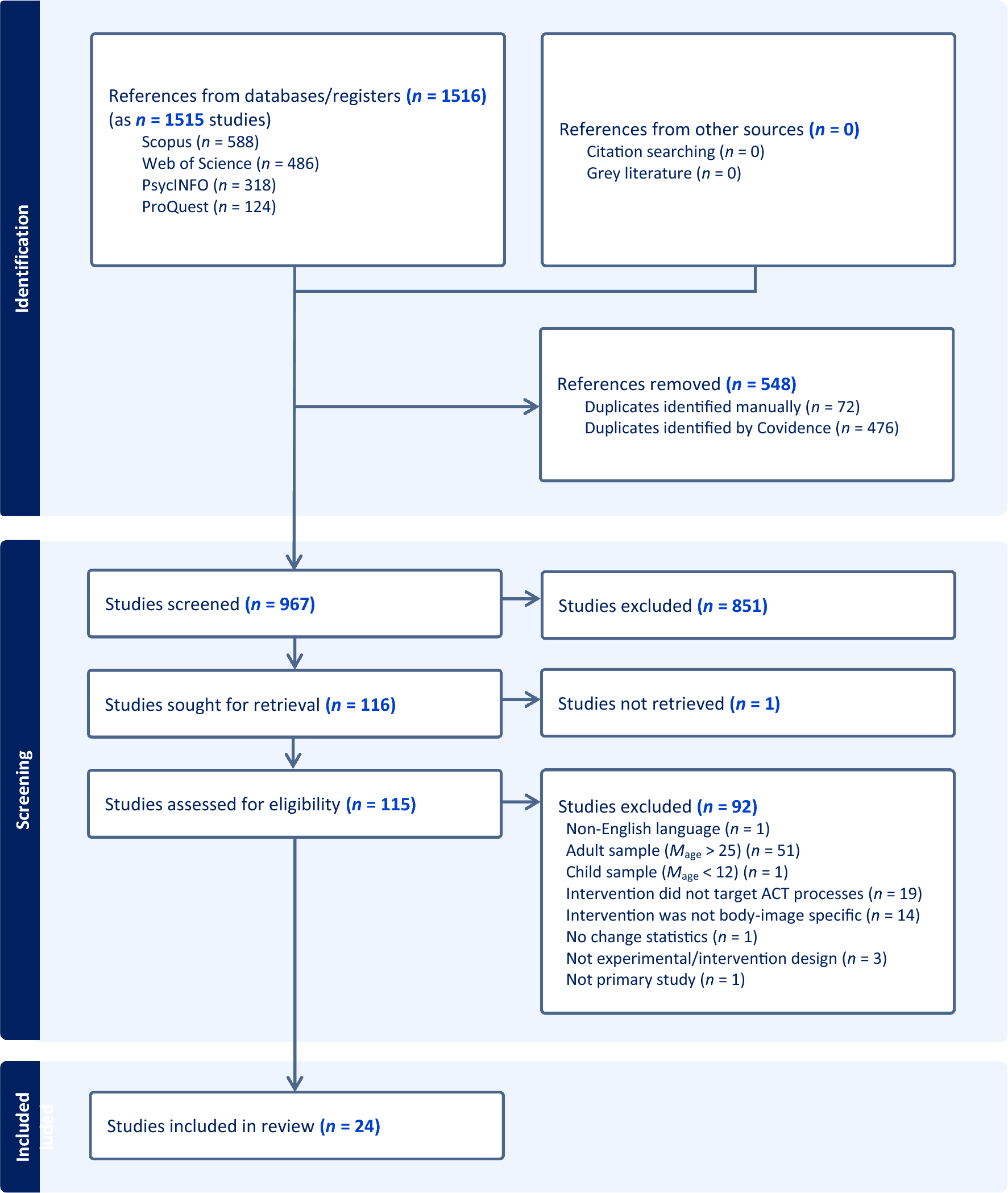

Through the review process, 18 studies from the 3,691 identified through initial searches were determined to be eligible for inclusion. Figure 1 illustrates the PRISMA flowchart which outlines the retention and exclusion of studies throughout the review process.
Table 2(at-risk) and Table 3(clinical) outline the characteristics of the 18 included studies. Six studies were conducted in the UK (33%), four in the USA (22%), two in Australia (11%), two in Canada (11%), two in Sweden (11%), and one each in Portugal (6%) and New Zealand (6%). Six studies used a clinical sample, and twelve used an at-risk sample. See Tables 2 and 3 for further details.
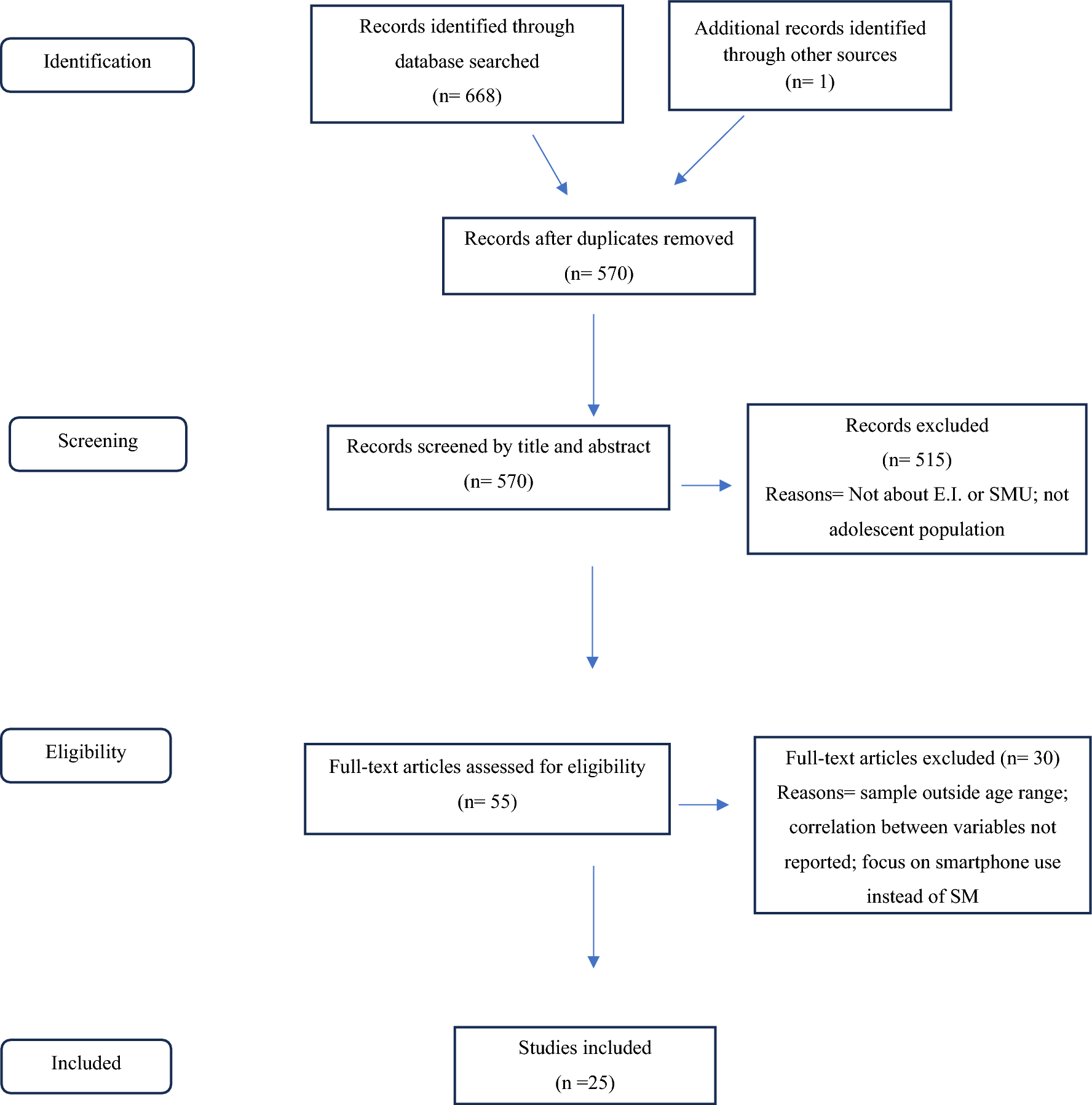
Category 1: Perceived Cause of Emotional Distress in at Risk and Clinical GroupsSix main themes were identified within this category: (1) challenging social factors and perceived difference; (2) problematic family dynamics; (3) cause is complex and multifaceted; (4) unfairness and perceived lack of agency; (5) concern for self and others; and, (6) coping with a mental health difficulty. Of these, challenging social factors and perceived difference, problematic family dynamics, and cause is complex and multifaceted were shared across both the at-risk group (ARG) and clinical group (CG). Several main themes were broad and captured the nuance of the content, some required subthemes for further clarification (see Fig. 2). The themes are presented to emulate the thematic map (see Fig. 2), with shared themes including ARG and CG findings, and divergent themes including findings only from the relevant group.
Fig. 2
Thematic map of perceived cause of emotional distress for the at-risk and clinical groups
Shared theme 1: challenging social factors and perceived difference. This shared theme illustrates that social pressure related to acceptance and feeling/being made to feel different were factors that young people felt contributed to the onset of distress. This includes pressure to emulate body “ideals” and not being able to live up to perceived beauty standards (Sabiston et al., 2007); family non-acceptance and personal non-acceptance regarding sexual orientation e.g., “[r]ight now, I’m not really, I don’t really accept it … it feels like there’s a weight on me” (Diamond et al., 2011 P.139); and, judgments and prejudices held by others based on the previous actions of the adolescents (King et al., 2014) or their background, for instance, “it seems that most people is afraid, they must be thinking that I’m a thug or something like that. Then, a robbery happens, and who is to blame? Me, of course. [and I feel] Outraged” (Magalhães et al., 2018, p.1809). Fear related to the judgments of others and the possible repercussions of those judgements, as well as fears for personal safety, worrying about others finding out, parents not being supportive, and being bullied were all noted as contributory factors for sexual minorities (Diamond et al., 2011). Other adolescents found that feeling alone (Majumder et al., 2015), being bullied/experiencing friendlessness as a result of being “different”, failing to feel “right” (Keyes et al., 2018), and a lack of authenticity from others (Crouch & Wright, 2004) as distressing. This included feeling like some people copied self-harming behavior to get attention, detracting from what they felt were the experiences of “authentic” self-harmers (Crouch & Wright, 2004). Similarly, nasty (Porteous et al., 2019) and derogatory comments, as well as ridicule in relation to racial and cultural identity, were also instances that young people identified as contributing to emotional distress (Edwards et al., 2019).
Shared theme 2: cause is complex and multi-faceted. Across both groups, adolescents identified multiple difficulties which, when combined, were perceived as causal, e.g. simultaneously dealing with factors like an ill loved one, financial/family/school/social-based stressors, and death of someone close (Porteous et al., 2019; McAndrew & Warne, 2014): “[i]t was just all at once: stress from school and stress from people, friends being horrible people, and the family arguing” (McAndrew & Warne 2014, p.573). While their personal circumstances may be different, for instance, being exposed to war and the associated difficulties – including the death of loved ones, extreme violence, seeing dead bodies, and having to leave their homes and families – (Majumder et al., 2015), or sexual minorities who may be dealing with the death of friends and family, rape, financial hardship, feeling unsupported and uncared for, family issues, and ill loved ones (Diamond et al., 2011), there is a recognition that emotional distress is not caused by a single factor. The multifaceted nature of causal attributions is also highlighted by some young people’s inability to understand what they are feeling or why they are feeling it (Wilmots et al., 2020), or that, for some, talking about the cause of their difficulties engenders further distress (Majumder et al., 2015). Indeed, coping strategies used to deal with distress may also subsequently become a cause of emotional distress; for instance, when talking about self-harm, one participant stated they “felt ashamed”, and another explained that “[a]fter the buzz had worn off, I felt terrible, guilty, bad” (McAndrew & Warne, p.573).
Shared theme 3: problematic family dynamics. Young people identified difficult home circumstances as emotionally distressing. This included witnessing parental abuse, “I wanted to kill myself ‘cause of shit between my mother and father” (Aymer, 2008, p.661), and fear of being abused in by paternal figures, “[h]e was so mean to us when he drank. I was scared he would hurt me” (Aymer, 2008, p.659). Parental conflicts, arguments, and financial stressors (Porteous et al., 2019; Ayme; Tinnfa ̈lt et al., 2011), as well as parental alcoholism (Aymer, 2008; Tinnfa ̈lt et al., 2011) were also identified. Other adolescents highlighted family conflict (Crouch & Wright, 2004), hostility in the family, parental divorce, separation, and arguments between parents, for instance: “I know there was arguments between (my) parents. Obviously, that does make you sad because you want them both to be happy” Keyes et al., 2018, p.180) as causal. Some young people even felt that if they were not dealing with family problems it would be transformative, for instance, “I think if my parents weren’t divorced and if my sister didn’t have cancer I would be a very, very different person and I would be smiley, happy” (Porteous et al., 2019, p.121).
At-risk group theme 1: concern for self and others. Some young people identified concern for themselves and those they care about as a source of emotional difficulties. This may include safety concerns due to the possible actions of an alcoholic paternal figure, or fear of gang-related violence: “I was afraid, ‘cause gang fights can start up again and, if you are around, you could be killed” (Aymer, 2008, p.660). Personal health related anxiety, feeling forgotten in the wake of a sibling having a terminal illness, as well as seeing a loved one in pain, and fearing they might die, may also be contributory (Phillips & Lewis, 2015; Porteous et al., 2019).
At-risk group theme 2: unfairness and perceived lack of agency. Feeling powerless and/or not having control over things happening in their lives, as well as being treated unfairly appeared to be causal factors for some adolescents. This included not being allowed to do what they wanted, leading to anger and subsequent aggression: “this morning I just punched a hole through my friggin [swear word] bedroom door… it helped” (Edwards et al., 2019, p.165), or teachers unfairly criticising young people (Edwards et al., 2019). Not receiving adequate educational support and subsequent concerns about not being able to secure a job, as well as being discriminated against or treated unfairly by the judicial system (Magalhães et al., 2018) also appeared to engender emotional distress. This extends to having other people make decisions about your life against your will, including reporting that you were the victim of an assault (Campbell et al., 2015). Additionally, not being kept informed about the treatment of an ill sibling may also be perceived as distressing: “You go into her room and it was like “what’s happening?” and she’s only getting x-rays, but I think she’s going into operation or something and it just made it difficult and it made me angry that they weren’t telling me anything” (Porteous et al., 2019, p.121).
Clinical group theme 1: coping with a mental health difficulty. Aspects of having a mental health difficulty were highlighted by some adolescents as a source of distress. This included stigma and shame around having a mental health difficulty; however, for some receiving a diagnosis was helpful in making them feel that they were not “crazy” (Keyes et al., 2018). The relentlessness of having a mental health difficulty was also raised as a factor in the onset of difficult affect: “[t]hat’s what made me cry, because I thought to myself, ‘Oh my god, this is a battle now” (Keyes et al., 2018, p.181). Indeed, living in fear of a “bad” feeling coming was noted as contributing to distress: “I find I am always scared of every day that comes because I am scared I am going to get depressed again. I am scared of that every day” (Woodgate, 2006, p.264).
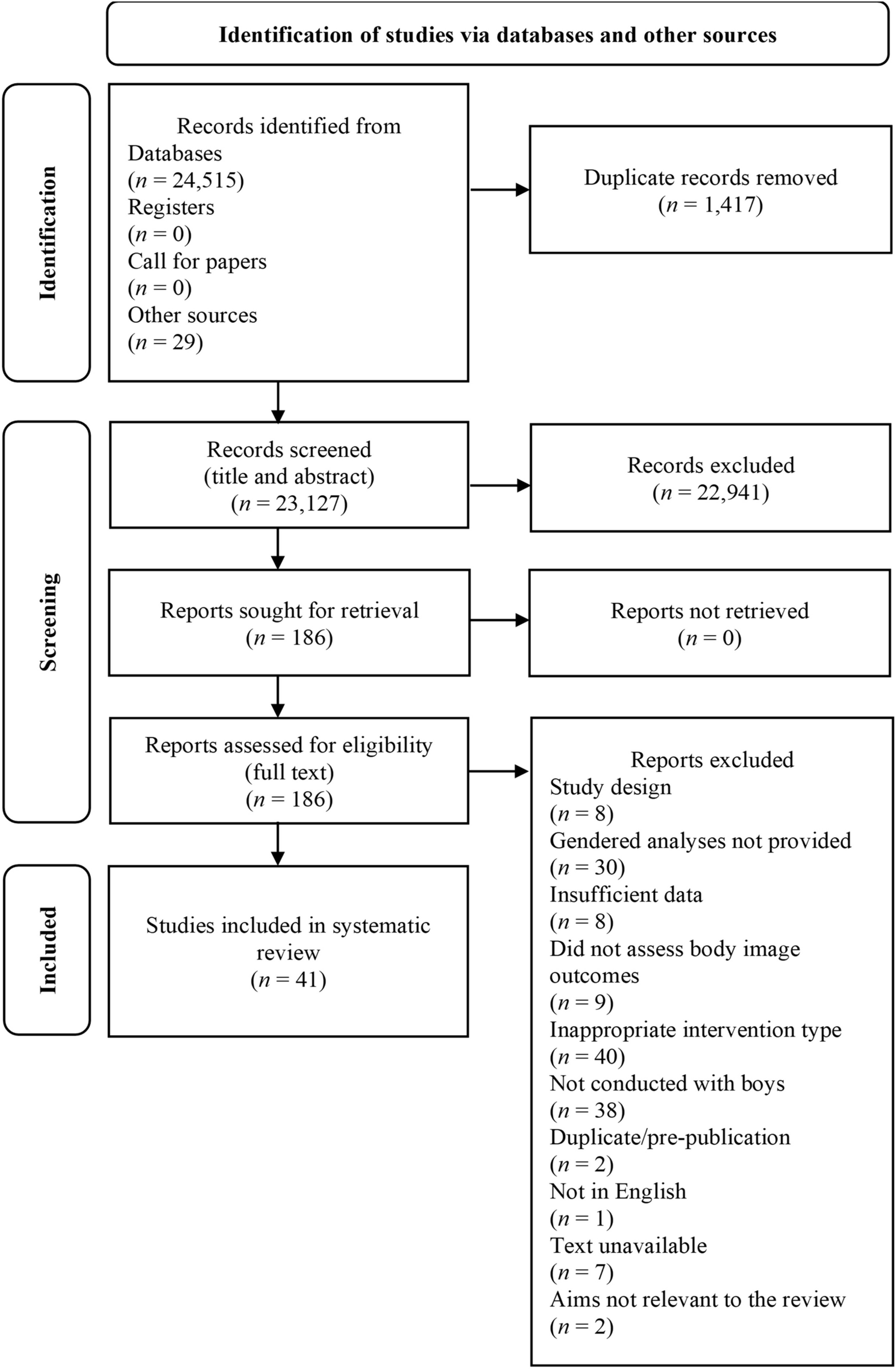
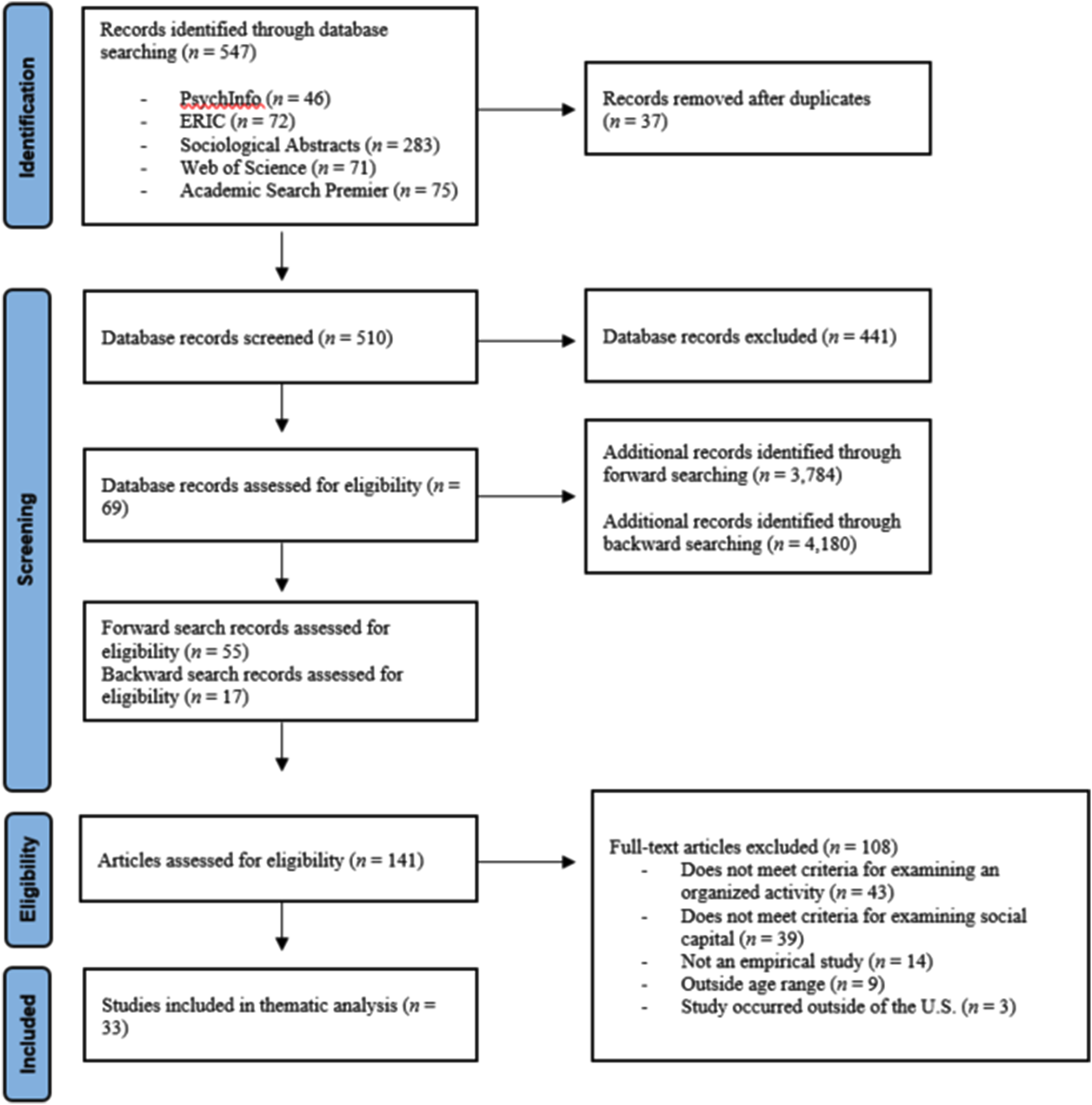
Category 2: Causal Perceptions and Their Influence on Help-seeking: Commonalities and Differences Among At-risk and Clinical GroupsFour themes were identified in this category, with accompanying subthemes. The main themes were as follows: cause and implications for self-preservation; the degree of personal and wider knowledge and understanding of cause; perceived extent of control in managing cause; and, cause having the potential to affect others. Explicit links between perceived cause and help-seeking were not required in the included studies. Rather, if there was information about help-seeking and perceived cause within the same sample, this was considered to be an association. Each main theme is relevant to both groups except cause having the potential to affect others, which applied only to the ARG. The remaining three themes are shared across the ARG and CG; however, there is divergence in the accompanying subthemes, which can be observed in Figs. 3 and 4. It is important to note that while the reporting of themes varies in length, this does not signify importance, but rather the fact that some are more complex and need more extensive explanation; therefore, the themes are only presented by group, in contrast to synthesis 1.
Fig. 3
Thematic map for the ways in which perceived cause(s) may influence help-seeking, at-risk group
Fig. 4
Thematic map for the ways in which perceived cause(s) may influence help-seeking, clinical group
At-risk group theme 1: cause and implications for self-preservation. The possible reactions and consequences of seeking help for the cause of their emotional difficulties may influence the ways in which young people seek help, or indeed if they seek help at all. For instance, adolescents may be hesitant to reveal the source out of fear that the cause may lead to bullying and ridicule (Porteous et al., 2019; Tinnfa¨lt et al., 2011), or concern that those they share with may betray their trust (King et al., 2014). Some may be hesitant to seek help due to fears that they may not be believed (Campbell et al., 2015; Tinnfa¨lt et al., 2011), or feel pressure to report their circumstances to make the cause more believable to others: “I hated how much pressure I was under to feel like I needed to prove to everyone that I wasn’t lying, so like I went and told” (Campbell et al., 2015, p. 835). There may also be concern that adults will be too quick to report disclosures to the authorities, which could result in negative consequences, such as being taken from their homes or upsetting their parents, which may prevent the disclosure of home-related difficulties (Tinnfa¨lt et al., 2011).
Similarly, concerns regarding perceived and possible judgment from others may affect how able young people feel to get help for their circumstances. As an example, adolescents with a sibling with cancer indicated that they would endure their experience in silence, which ranged from just not wanting to talk about it, due to the personal nature of the topic, to a way to manage impressions (Porteous et al., 2019); silence may also be used as a form of protection from bullies who might use the cause of their distress against them (Porteous et al., 2019; Tinnfa¨lt et al., 2011). However, some young people view school as a kind of respite from their problems: “[b]ecause sometimes I don’t want other people to know […] School is my break” (Grove et al., 2016, p.3062). Or may avoid discussing cause as a form of self-protection: “I guess my own fears, death really … stops me from talking about it” (Phillips & Lewis, 2015, p.855). Young people may eventually share their concerns with an adult, but may find it difficult to initiate the conversation, especially if they feel it is difficult for the adult to discuss (Phillips & Lewis, 2015; Porteous et al., 2019; Tinnfa¨lt et al., 2011).
At-risk group theme 2: the degree of personal and wider knowledge and understanding of cause. The value of shared experience and understanding of cause was identified as a factor in seeking support, whereas ignorance regarding cause appeared to be problematic. Young people may feel more comfortable reaching out for help and sharing their experiences with someone they feel has personal experience of the cause. In some instances, adolescents perceive their circumstances to be poorly understood by those without personal experience. They may also find themselves having to manage the ways in which they share their difficulties to avoid making others feel uncomfortable: “if panic arises you back off” (Tinnfa¨lt et al., 2011, p. 141). These kinds of reactions can lead to social isolation and avoidance of sharing difficulties to prevent the discomfort of others (Porteous et al., 2019). While shared experience of cause may be of value to the help-seeking process, some adolescents feel comfortable sharing with those without direct experience, provided they react in an understanding way: “I felt good [for sharing her placement in care with a friend], and my friends understood” (Magalhães et al., 2018, p.1810). In order to share their difficulties, young people need to know that their problems will be taken seriously (Tinnfa¨lt et al., 2011). Nonetheless, a lack of broader understanding of the issue may result in those they seek help from dismissing their problems as typical, possibly leading to disengagement with support (McAndrew & Warne, 2014).
Knowledge surrounding the cause of emotional distress might facilitate understanding and, therefore, may enable young people to feel more comfortable seeking help. Adolescents appear to recognise the benefits of extending knowledge relating to cause and would value information being made available more broadly (Grove et al., 2016). An increase in knowledge may even facilitate coping strategies: “I can cope better with help when I know what it is and how her illness works” (Grove et al., 2016, p. 3061). Indeed, some may notice a lack of resources, and indicate that this is problematic: “[t]here are posters all around school (for smoking), but then there’s nothing for counselling or anything like that” (McAndrew & Warne, 2014, p.575).
(Un)met expectations of support appear to contribute to distress. Adolescents indicate that having the opportunity to reflect on and discuss how they feel may decrease their embarrassment and encourage them to talk more openly, which may lead them to be able to resolve their own problems (Daniunaite et al., 2012). However, depending on the circumstances, some adolescents might attempt to communicate the cause of their distress in less obvious ways, and expect a teacher to realise that there is a problem (Tinnfa¨lt et al., 2011). Young people indicate that having individuals take an interest in them and ask questions was helpful for sharing, but not in a way that would overburden them (Phillips & Lewis, 2015; Porteous et al., 2019; Tinnfa¨lt et al., 2011). Being able to recognise the need for help personally in relation to cause may act as a foundation to help seeking; however, having people close to you confirm the need for help may play a factor in propelling towards change (Campbell et al., 2015; Daniunaite et al., 2012), but only if it is recognized by the young person first (Daniunaite et al., 2012).
In some instances, expectations of support may not be met, or adolescents may not feel that their difficulties are worthy of help: “I don’t really know why I keep my emotions to myself cos, I probably like, I know there must be people out there that’s worse off than me” (King et al., 2014, p.15). Young people may also feel that their teachers do not recognise their issues or feel that teachers know there is a problem but do not try to help (Tinnfa¨lt et al., 2011, p.143). Further, adolescents may feel the kind of support available is not suited to addressing the cause, for instance, not thinking of a GP as someone you can talk to about self-harming (McAndrew & Warne, 2014, p.574).
At-risk group theme 3: perceived extent of control in managing cause. Some young people expressed a desire to be involved in overcoming the factors influencing their difficult emotions. In some of these instances, it appears that adolescents who believe the cause of their emotional distress can be self-treated may avoid seeking help, opting instead for alternative approaches, e.g., attempting to treat body related anxiety by limiting food intake, excessive exercising, and using diet pills and laxatives to lose weight (Sabiston et al., 2007). Some may feel a sense of responsibility to take control over contributing factors, this might include recognising the issues and putting behaviors in place to address them rather than seeking help (Daniunaite et al., 2012). However, adolescents who do consider exploring options for help may perform a risk assessment on adults before disclosing, perhaps to maximise the extent they can remained involved (Tinnfa ̈lt et al., 2011). On the other hand, adolescents may feel they have no choice but to disclose, especially if they feel the cause has to be reported to the authorities and to do so will have to tell their parents (Campbell et al., 2015). Thus, the extent to which perceived cause for emotional distress might influence help seeking may depend on how much control young people feel they have in overcoming the cause.
The degree to which young people feel they can control their reactions to causal factors may also influence help seeking. For instance, young people appear to explore a number of strategies to help mitigate against the cause of emotional distress. Alternative coping strategies to manage how they react might include thinking positively and trying to expect the best outcome, thinking that others have worse problems than they do, as well as crying and angry outbursts (Porteous et al., 2019). Exercise and recreational activities (Aymer, 2008; Porteous et al., 2019) as well as self-harming as a way to manage/relieve stress and to feel pain elsewhere (Tinnfa ̈lt et al., 2011; McAndrew & Warne, 2014). Strategies may be recommended by peers, including self-harming to relieve stress (McAndrew & Warne, 2014). Some young people indicate they have available support systems around them but prefer self-management, and recognize that everyone has their own way of dealing with things (King et al., 2014). However, some young people may not want others to know about their self-management strategies, specifically self-harming due to associated shame; thus, some coping strategies can become a source of distress and shame surrounding this may delay help-seeking (Tinnfa ̈lt et al.,
Comments (0)