
Remember me



The DPC database includes administrative claims data for approximately 8 million inpatients discharged per year from more than 1000 acute care hospitals in Japan. The attending physicians are required to accurately record the diagnoses because these diagnoses are linked to a health insurance payment system. The DPC database contains patient information on the following variables: demographics and selected clinical information: admission and discharge, discharge status (deceased or living), diagnoses, surgeries and procedures performed, medications administered, and special reimbursements for specific conditions. The DPC database also includes dates of procedures and the dosages and dates of all drugs administered during hospitalization [13, 14].
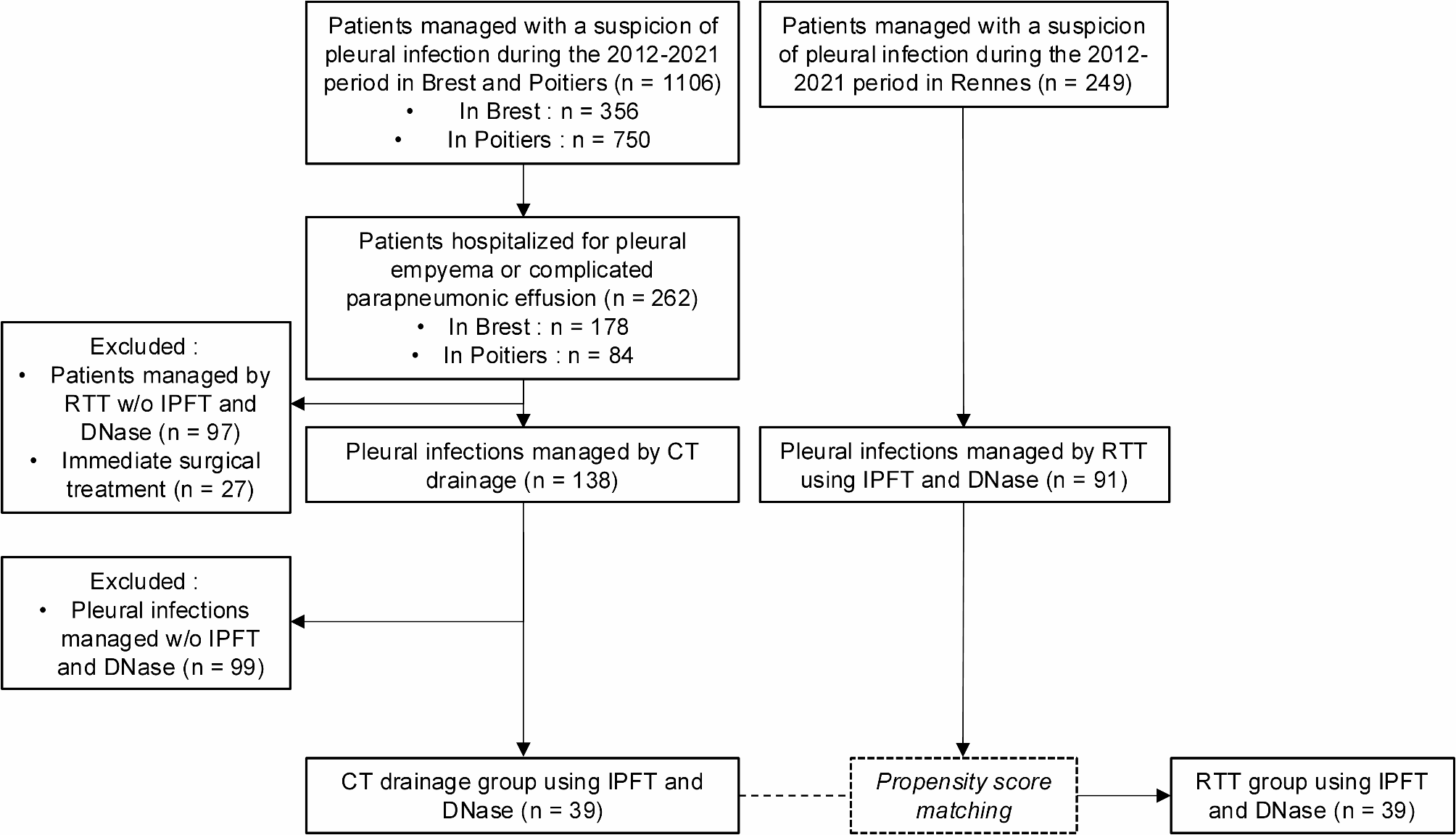
Patient selectionIn this retrospective cohort study, we identified severe CAP-associated ARDS, which was defined as mechanically ventilated patients who were diagnosed with sepsis and pneumonia and received β-lactam within hospital 2 days after admission between July 2010 and March 2015. Defining sepsis was based on the previous criteria (see Additional data 1) [14, 15]. Defining pneumonia was based on ICD-10 codes J13–J18, which is listed as the primary diagnosis or as comorbidities at admission. The patients required mechanical ventilation within hospital 2 days after admission. ARDS was defined as ICD-10 code J80 as the primary diagnosis or comorbidity at admission (Fig. 1).
Fig. 1
Flowchart of patient selection
The patients who meet the following criteria were excluded: < 18 years of age; discharge within hospital 2 days after admission; malignant neoplastic diseases; autoimmune disorders; intravenous erythromycin use within hospital 2 days after admission; and oral clarithromycin use within hospital 2 days after admission.
VariablesThe azithromycin group included only patients who received intravenous or oral azithromycin within hospital 2 days after admission, whereas the control group included only patients who did not receive azithromycin within hospital 2 days after admission.
Other variables that were assessed include age, sex, hospital type, hospital volume, comorbidities at admission, the Japan Coma Scale score, the age, dehydration, respiration, orientation, and blood pressure (A-DROP) system, and need for the procedures within hospital 2 days after admission. Hospital type was categorized as academic or nonacademic. Hospital volume was defined as the average annual number of mechanically ventilated patients with CAP within hospital 2 days after admission, in each hospital. The Japan Coma Scale score was recorded for all patients at admission; the level of consciousness was assessed on admission, which correlated well with the Glasgow Coma Scale [16]. We categorized the Japan Coma Scale score into four groups: 0 (alert), 1–3 (delirium), 10–30 (somnolence), and 100–300 (coma). We used the A-DROP system to assess the severity of CAP on admission. This scoring system is similar to the CURB-65 system of the British Thoracic Society and has been validated in the DPC database [17]. A-DROP severity scores were categorized into four groups: 0 (mild group), 1–2 (moderate group), 3 (severe group) and 4–5 (extremely severe group). Mild group was defined as patients who can be treated as outpatients. Moderate group was defined as patients who may be admitted to the hospital and treated. Severe group was defined as patients who should be admitted to the hospital and treated. Extremely severe group was defined as patients who require intensive care managements. Patients with missing data on A-DROP were categorized as missing on this variable. Need for the following procedures within hospital 2 days after admission was also examined: intermittent renal replacement therapy; continuous renal replacement therapy; extracorporeal membrane oxygenation; red blood cells transfusion; platelet concentrates transfusion; fresh-frozen plasma transfusion; intravenous noradrenalin; intravenous dopamine; intravenous dexamethasone; intravenous hydrocortisone; intravenous methyl prednisolone; intravenous prednisolone; intravenous antithrombin; intravenous recombinant human soluble thrombomodulin; intravenous immunoglobulin; intravenous sivelestat sodium; primary intravenous antibiotic used, divided into Ranks 1 to 5, drawing on a previous study [18] (see Additional data 2); intravenous anti-methicillin-resistant Staphylococcus aureus (MRSA) drugs; and intravenous fluoroquinolone.
Outcome measuresThe outcomes of this study were 28-day mortality and in-hospital mortality.
Statistical analysisDescriptive data are reported as numbers and percentages for categorical variables and as means and standard deviations for continuous variables. Descriptive statistics were assessed before and after propensity score matching and after inverse probability of treatment weighting (IPTW). We performed one-to-four propensity score matching to adjust for differences in baseline characteristics and disease severity on admission between the two groups. The probability that a patient received azithromycin was adjusted for potential confounders using the following characteristics: age, sex, hospital type, hospital volume, Japan Coma Scale scores, A-DROP, comorbidities at admission, renal replacement therapy, extracorporeal membrane oxygenation, transfusion, vasopressors, intravenous steroids, intravenous immunoglobulin, intravenous antithrombin, intravenous recombinant human soluble thrombomodulin, intravenous sivelestat sodium, and Rank 1-5 antibiotics, fluoroquinolone, and anti-MRSA drugs used. The following interaction terms were added to estimate the propensity score to achieve a better balance in patient characteristics between the two groups: age and mild A-DROP score, age and dopamine, age and somnolence as consciousness level and extracorporeal membrane oxygenation, and fluoroquinolone and anti-MRSA drugs. Several elements from the patients’ medical histories (severe liver disease, hemiplegia, or paraplegia) and initial use of several drugs (clindamycin, aminoglycoside, tetracycline, and anti-fungal drugs within hospital 2 days after admission,) were not included in this analysis because they were relevant only to a few patients. We used absolute standardized mean differences and assessed the balance in patient characteristics [19]. Absolute standardized mean differences of less than 0.1 were considered negligible imbalances in baseline characteristics and disease severity on admission between the groups [20]. Fisher’s exact test was performed to compare 28-day mortality and in-hospital mortality between the groups. We used IPTW to estimate the treatment effect [21]. We calculated risk differences and their 95% CIs between the before and after propensity score-matched, and after IPTW analyses [21]. The level of statistical significance was P < 0.05 for a two-sided test. Propensity score matching was conducted with the “matching” package, and IPTW analysis was conducted with the “survey” package in R statistical software, Version 3.1.3 (The R Foundation, Vienna, Austria). All other analyses were conducted using IBM SPSS, Version 25 (IBM SPSS, Armonk, NY).
Comments (0)