
Remember me



Granular data on all fully robot-assisted extended total gastrectomies with a transthoracic long Roux limb reconstruction performed at the ZGT Hospital in Almelo, the Netherlands, in the time frame 2016–01–01 (inception)–2024–12–31 were collected from a prospective registry database and validated/supplemented from electronic medical records.
An extended Roux limb was defined as a jejunal Roux limb mobilized by selective division of proximal jejunal mesenteric vessels, allowing a tension-free esophagojejunostomy with increased effective limb reach compared with standard Roux-en-Y reconstruction.
Anastomotic leak was defined according to the ECCG criteria.
Pneumonia was defined as a new infiltrate on chest radiograph associated with clinical signs of infection.
StatisticsAll data were summarized in tables and categorized for patient, preoperative tumor characteristics, operative, postoperative, and pathology data.
Continuous values were presented as mean (± SD) or median (IQR) depending on their normality of distribution.
Kaplan–Meier analysis was used to evaluate survival outcomes.
All statistical analyses were performed using the IBM SPSS Statistics 30.0 (Build 172) software for Mac.
All statistical figures were created using Matplotlib for Python.
OutcomesThe aim of this study was to assess the feasibility and safety as well as oncologic and survival outcomes of this fully robotic approach.
A summarized point-by-point description of the procedureAll procedures were performed using the DaVinci Xi platform (Intuitive Surgical Inc) (Fig. 1).
Fig. 1
A Trocar positions for abdominal phase, B Circumferent esophageal mobilization high up in the mediastinum, C Transection of the esophagus high up in the mediastinum, D Isolation of jejunal vessels of the long roux limb, E Before division of jejunal vessels an ICG-control is performed with the vessels clamped to ensure adequate perfusion, F The long roux limb is brought up to the right pleura and sutured to the right crus, G Trocar positions for thoracic phase, H An end-to-side esophagojejunostomy is performed transthoracically
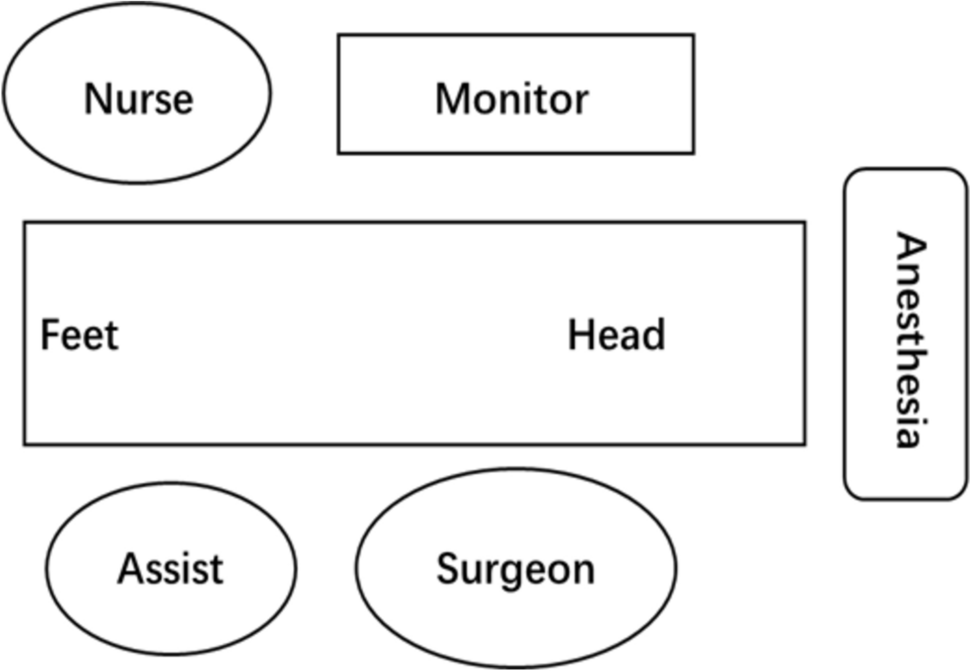
Abdominal phaseThe patient is positioned supine in the French position and tilted in slight anti-Trendelenburg (15–20°). Four robotic trocars (three 8 mm and one 12 mm) are inserted. Additional incisions include a 5-mm subcostal incision for the REVEEL® liver retractor (Microline Surgical, Inc., Beverly, MA, USA) and an 8 mm assistant port incision. See Fig. 1A for trocar positions. The dissection part of the abdominal phase is performed according to the standard technique for robot-assisted minimally invasive gastrectomy (RAMIG) [14]. The esophagus is then mobilized as high into the mediastinum as possible (Fig. 1B) and transected using the SureForm™ robotic stapler (Intuitive Surgical, Inc., Sunnyville, CA, USA) with a blue reload cartridge, either during this phase or later in the thoracic phase (Fig. 1C). A long Roux limb is created intracorporeally. Jejunal vessels arising directly from the superior mesenteric artery are identified, and one to three branches are divided depending on the required length (Fig. 1D). Prior to each division, the vessels are clamped, and indocyanine green (ICG; Verdye®, Diagnostic Green GmbH, Aschheim-Dornach, Germany) is injected intravenously to assess perfusion of the jejunal arcade (Fig. 1E). The right pleura is opened transhiatally under direct visualization, and the long Roux limb is introduced into the mediastinum, either in an ante- or retrocolic fashion. In order for it to not fall down or rotate during repositioning of the patient and to “know” how much you can pull it up in the thorax, it is secured to the right crus using a Vicryl® suture (Ethicon, Johnson & Johnson MedTech, Somerville, NJ, USA) (Fig. 1F). A stapled enteroanastomosis is then constructed approximately 60–70 cm distally of the level of the jejunal alimentary transection. A closed-suction Jackson-Pratt® drain (Cardinal Health, Dublin, OH, USA) is advanced to the mediastinum along the Roux limb. A feeding jejunal catheter is inserted. If the esophagus has already been transected in this phase, the specimen is extracted through a small Pfannenstiel incision, thereby completing the abdominal phase.
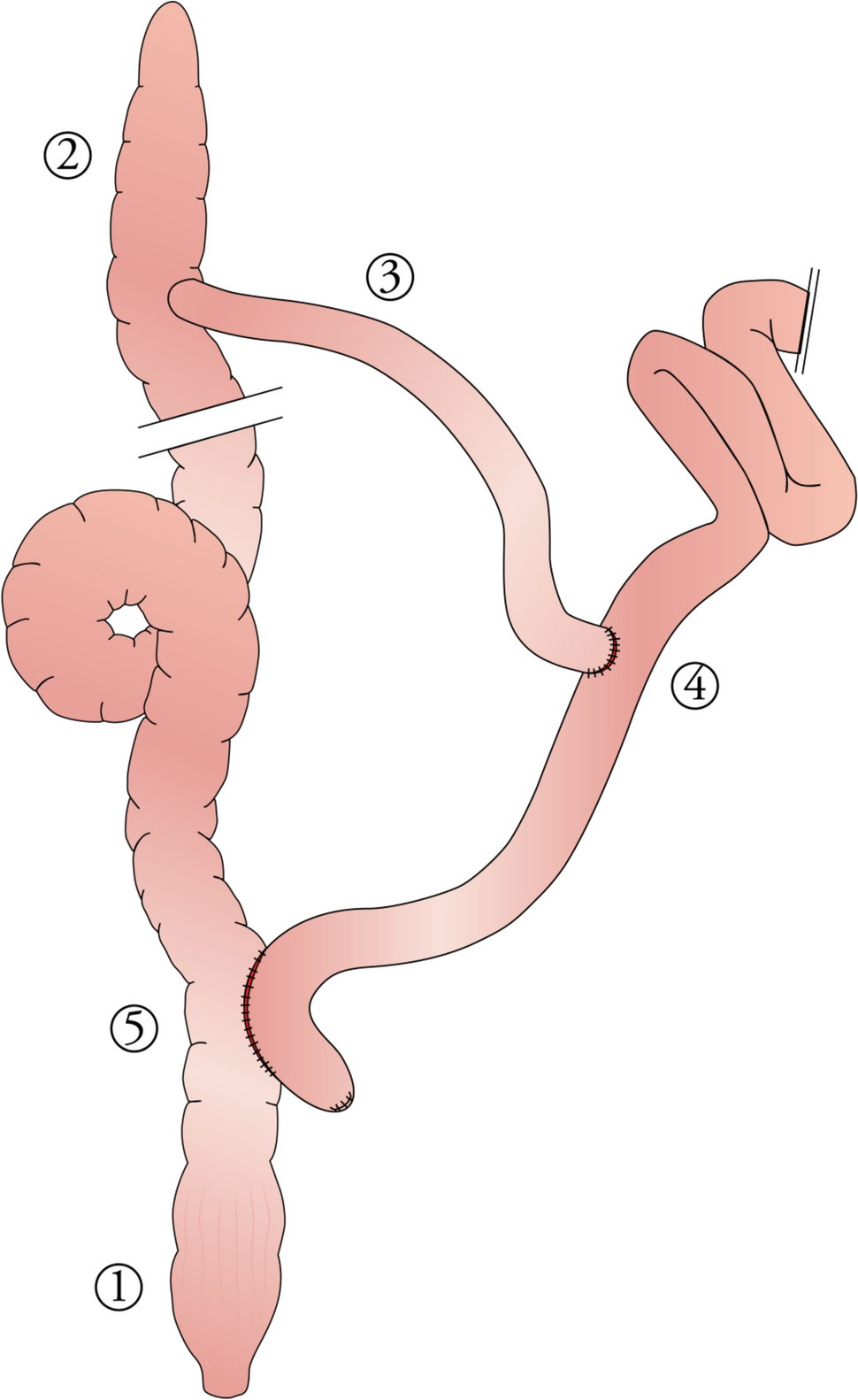
Fig. 2
The final result with an end-to-side esophagojejunostomy high up in the mediastinum, here with two divided jejunal arteries. © Adam Zeyara, MD
Thoracic phaseThe patient is repositioned to a semiprone “crawl” position, and single-lung ventilation is initiated. Robotic ports are placed (four 8 mm robotic ports, and if the specimen was not extracted during the abdominal phase, one of these should be a 12 mm port to allow for stapling), along with an 8 mm assistant port. See Fig. 1G for trocar positions. A paravertebral block catheter is inserted into the subpleural space for regional anesthesia. The esophageal mobilization is then completed, and a thoracic D2 lymphadenectomy is performed if indicated (paraesophageal and subcarinal stations). If not already divided, the esophagus is transected here using the SureForm™ robotic stapler (blue cartridge). An end-to-side hand-sewn esophagojejunostomy is created using two running 3–0 V-Loc™ barbed sutures (Medtronic, Minneapolis, MN, USA) and then reinforced with interrupted 4–0 PDS™ II monofilament sutures (Ethicon, Johnson & Johnson MedTech) (Fig. 1H). If the specimen has not been removed earlier, it is extracted through a small thoracotomy at the assistant port site using an Alexis® wound retractor (Applied Medical, Rancho Santa Margarita, CA, USA). The Jackson-Pratt® drain (introduced during the abdominal phase) is now positioned along the anastomosis. A pleural flap is sutured over the anastomosis with a running 4.0 PDS™. A schematic illustration of the final reconstruction is shown in Fig. 2.
Fig. 3
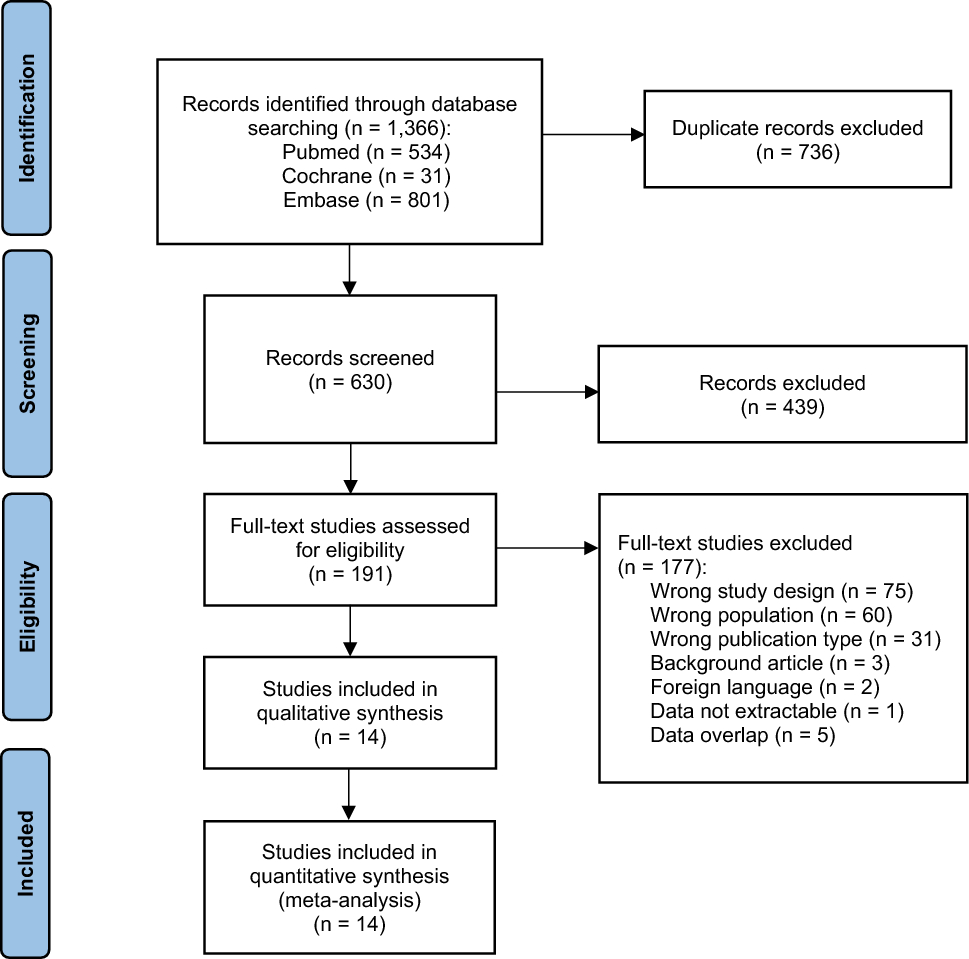
This algorithm/flowchart was made to contextualize the fully robotic extended total gastrectomy with transthoracic long Roux limb-reconstruction in the spectrum of treatment options of junctional cancers. As shown in the figure, the technique was solely employed for patients with junctional cancers where a gastric conduit was precluded (whatever the reason) and when there were proximal margin radicality concerns to such a degree that a safe abdominal/transhiatal esophagojejunostomy could not be performed. These patients would traditionally have been considered for open surgery with a long Roux-limb or a colonic interposition
Comments (0)