Case report: Ryle’s Tube Insertion into Pericardium Perforating the Internal Jugular and Right Atrium
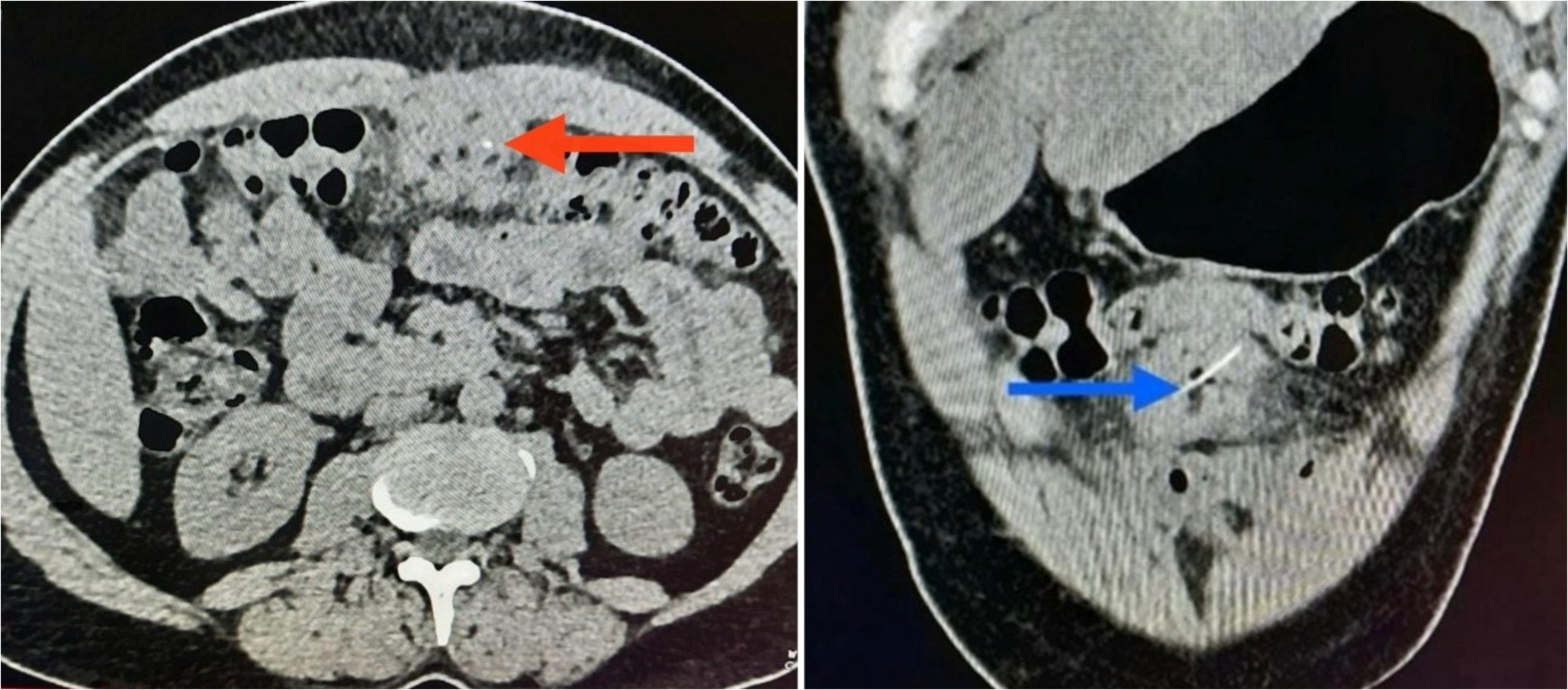
Nasogastric (Ryle’s) tube insertion is a common and typically safe bedside procedure performed for gastric decompression, feeding, or medication delivery. Complications are rare but can be serious, especially when the tube is inserted blindly. We present a life-threatening complication involving internal jugular and cardiac perforation by a Ryle’s tube. A 44-year-old female with epigastric pain was referred to our emergency department with a suspected hollow viscus perforation as per the CT scan already taken. She had undergone Ryle’s tube insertion after the CT scan from the referred hospital, following which she developed chest discomfort and back pain. Chest X-ray revealed the tube tip in the left hemithorax. A CT scan showed the Ryle’s tube had perforated the oropharynx, entered the right internal jugular vein, traversed the superior vena cava, pierced the right atrium, and terminated within the pericardium. Emergency sternotomy was performed to remove the tube. The puncture site at the atrial wall was secured, and a feeding jejunostomy was placed. Post-operative recovery was uneventful. Though nasogastric tube misplacement into the airway, pleural cavity, or even intracranially has been reported, direct cardiac injury is exceedingly rare and, to our knowledge, not previously described. This case highlights the importance of adhering to safe insertion protocols, confirming tube position radiographically when in doubt, and avoiding premature removal of malpositioned tubes without understanding their exact trajectory. This is an extremely rare case of a Ryle’s tube causing cardiac injury. Clinicians must remain vigilant during even routine procedures, and any resistance during insertion or patient discomfort should prompt reevaluation. Radiological confirmation should be obtained before repositioning or removing an atypically placed tube.










Comments (0)