
Remember me


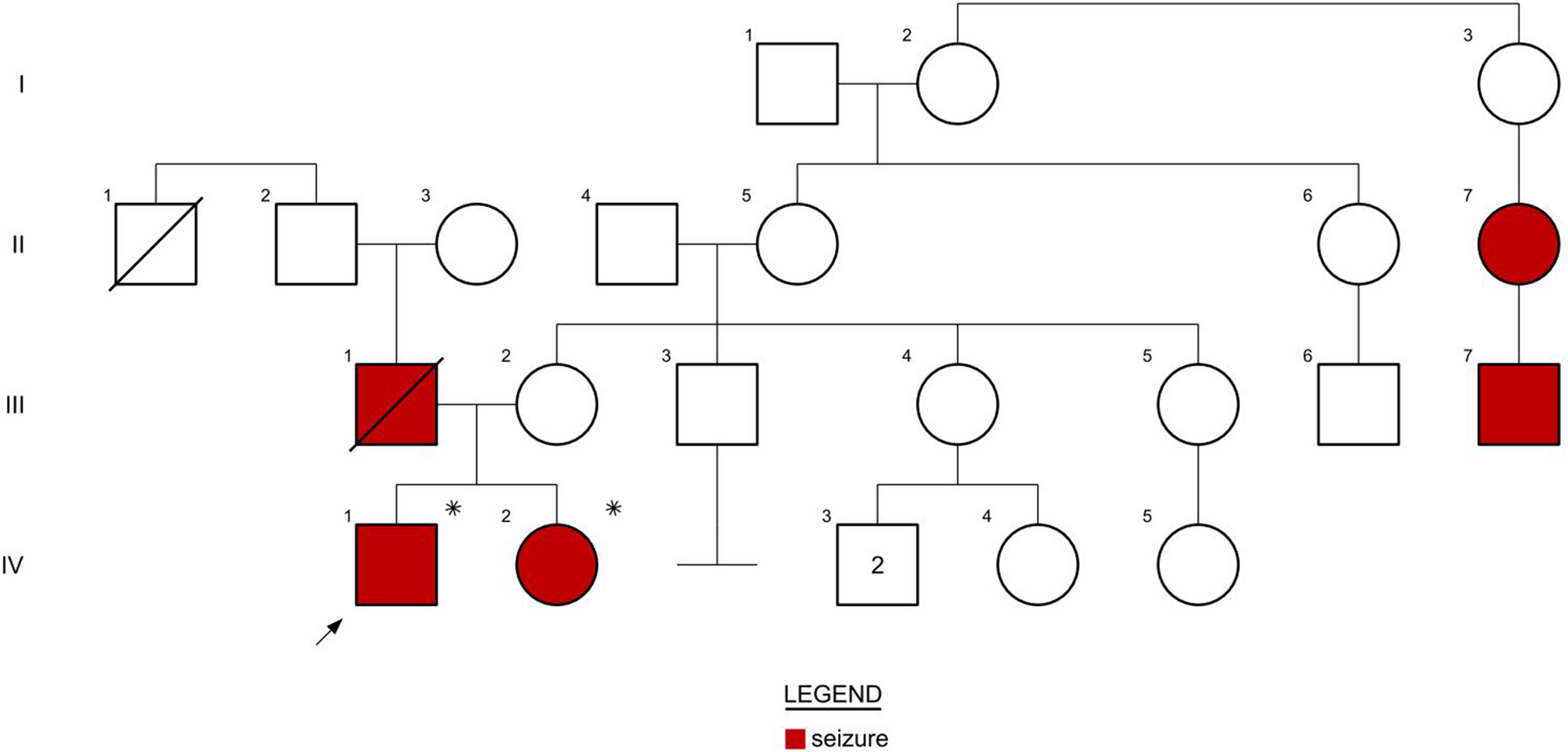


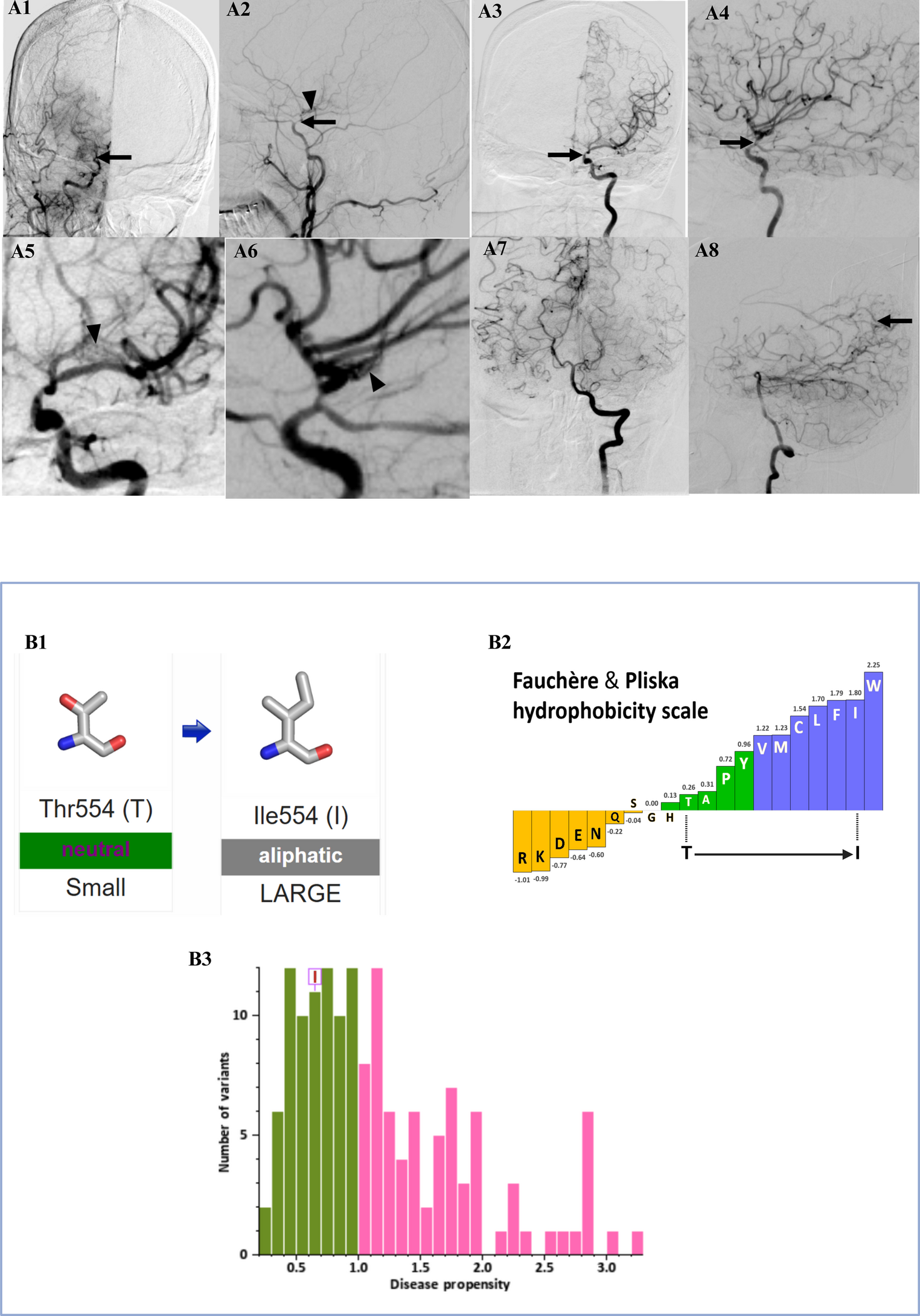
Twenty-eight (n = 28) participants were referred to the study, 26 of whom were eligible to participate. Seven participants did not provide consent to participate in the study, and three participants consented but were subsequently lost to follow up. The two participants who were not eligible did not have SETBP1 variants in or adjacent to the SGS 12 amino acid hot spot degron. Data was obtained for 16 participants (male = 9, female = 7) with pathogenic SETBP1 missense variants (Fig. 1; Table 1). Participants were from the United States (n = 7), the United Kingdom (n = 4), one participant each from Argentina, Canada, Denmark, Hong Kong, and Serbia. Several participants shared the same missense variant, as depicted in Fig. 1. Participants 1–4 had atypical SGS with variants just outside the SGS degron (outside amino acid residues 868 to 871, Fig. 1; Table 1). Four participants had passed away between one (n = 2) and six years (n = 2) prior to the study, with their caregivers providing retrospective information on their child (Table 1). The median age for all 16 children was 5 years 7 months (Q1-Q3 = 1 year 10 months – 7 years 9 months), and the median age for the 12 living children was also 5 years 7 months (Q1-Q3 = 1 year 3 months − 8 years 1 month). Participant 2 also had a confirmed pathogenic compound heterozygote in GJB2, which is implicated in autosomal recessive hearing loss.
Table 1 Genotype and demographic information of 16 individuals with Schinzel-Giedion syndromeMedicalAll participants completed the CombinedBrain medical survey (Table 1). Participants 5, 6, 9 and 13 had died (4/16, 25%) between the aged of 3 years, 10 months to 7 years, 10 months. Causes of death were cardiac arrest (participants 5 and 9) and seizures (participants 6 and 13).
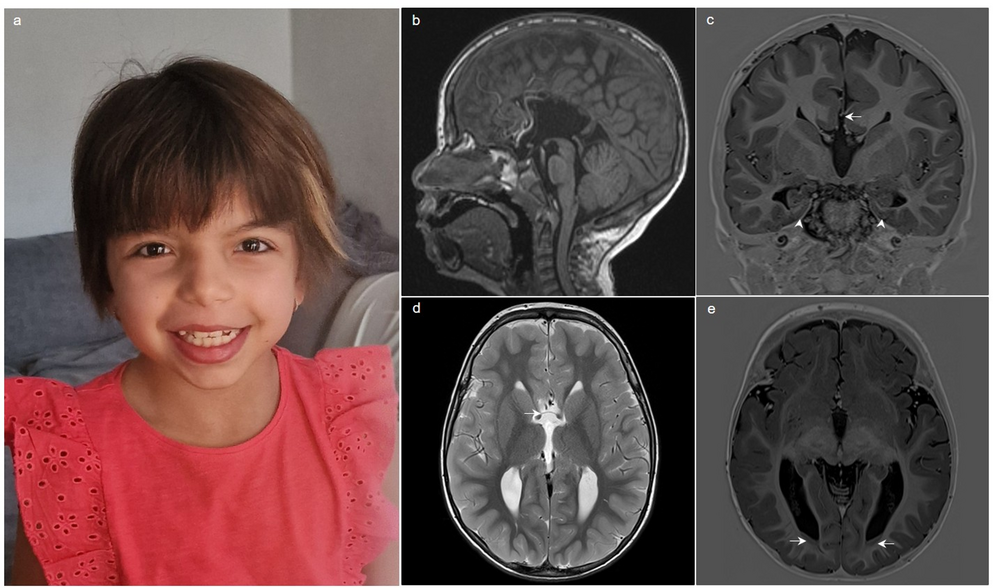
Visual impairment was common (14/16, 88%) and in the remaining participants, 1/16 (6%) caregiver was unsure if their child had a visual impairment and participant 15 did not have a visual impairment. The nature of the visual impairment included cortical visual impairment (4/16, 25%), optic nerve atrophy (3/16, 19%) and myopia (3/16, 19%). Hearing impairment was less common (9/16, 56%). Participants 9 and 15 had cancer (2/16, 13%), both malignant tumours as the base of the spine. 14/16 (88%) participants had urogenital conditions and 13/16 (81%) had musculoskeletal conditions.
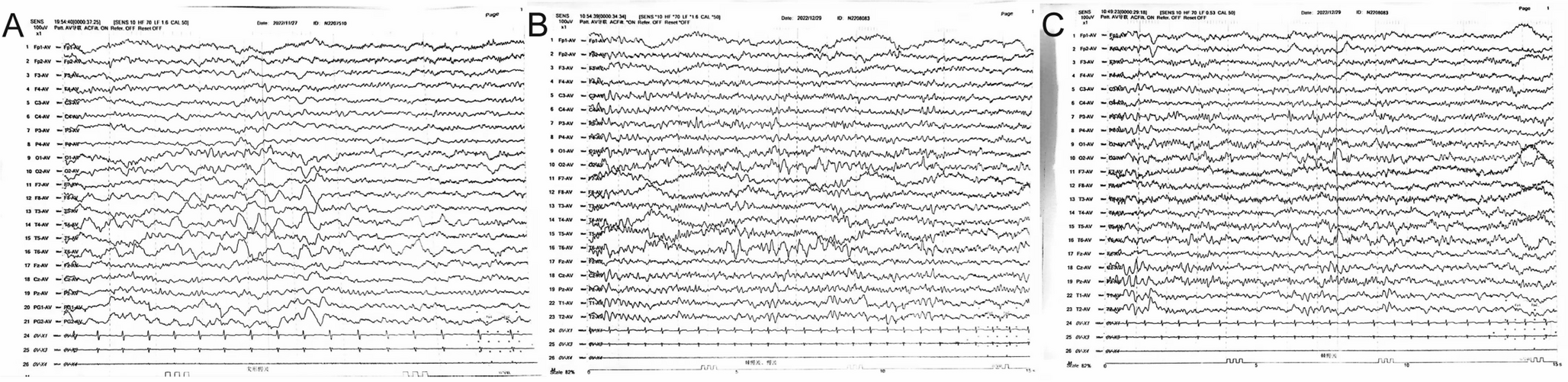
All participants had seizures apart from participant 2 who had atypical Schinzel-Giedion Syndrome outside 12 amino acid hot spot degron (15/16, 94%). Seizure onset was at 0 to 3 months (8/16, 50%), 4 to 7 months (2/16, 13%), 8 to 11 months (2/16, 13%), 2 years old (1/16, 6%, participant 7) and 7 years old (1/16, 6%, participant 1). Age at seizure onset was not specified for participant 5. 14/16 (88%) caregivers provided detailed information on additional neurological features. Hypotonia was more common (11/14, 79%) than hypertonia (9/14, 64%). 4/14 (29%) had encephalopathy.
FeedingDigestive issues were frequent (15/16, 94%), with only participant 3 unaffected. Details of digestive issues were provided by 14/16 (88%) participants, and included oesophageal (6/14, 43%), stomach (6/14, 43%), intestinal (6/14, 43%) and liver (1/14, 7%) concerns. 11/14 (79%) participants provided data on oral health, and several (6/11, 55%) participants had oral health concerns.
Fourteen caregivers completed the PASSFP (Fig. 2). 8/14 (57%) children had some food or drink orally (Fig. 2) with 3/8 (38%) children could only take small tastes of food. Most (9/14, 64%) relied on tube feeding for nutrition. One-quarter of children (4/14, 29%) ate orally with special modifications without enteral feeding, one child (1/14, 7%) primarily fed orally but had some supplemental enteral feeding. All children who could eat orally (8/8, 100%) could eat liquid and puree consistencies, preferably at room temperature. Participants 1 and 11 could eat foods of a variety of temperatures, and a range of consistencies; from liquids to soft chewable foods (e.g., potato chips). Participant 9 could also eat hard chewable foods (e.g., apples). Due to the open mouth position, dysmorphology that is characteristic of SGS [28], most children opened their mouth to accept a bottle or spoon (5/8, 63%). Children coughed, choked, or gagged ‘sometimes’ when eating orally (4/8, 50%) and many children ‘always’ had anterior spillage (3/8, 38%). Six (6/14, 43%) participants could have any food or drink orally. The average PASSFP score was 25 (SD = 14, ranging 7–43 out of possible total of 66, Table 1, Fig. 2).
Fig. 2
Feeding skills of 14 individuals with Schinzel-Giedion Syndrome children ≥ 1 year of age as measured by the Paediatric Assessment Scale for Severe Feeding Problems (PASSFP).* = items scoring reversed. Red = more severe feeding impairment, green = less severe feeding impairment
Adaptive behaviour and motor skillsVineland-3 scores were severely impaired across all domains (standard score normative mean = 100, standard score normative SD = 15). Daily living skills (standard score median = 44, Q1-Q3 = 38–53) ranged from age equivalents of 0 months to 9 months old (Table 2). In terms of specific daily living skills, 4/16 (25%) individuals ‘sometimes’ cooperated with parents dressing and undressing them. Individuals could ‘sometimes’ (3/16, 19%) and ‘usually/often’ (2/16, 13%) cooperate with hand and face washing. Participant 3 could feed themselves with a spoon, and participant 1 could ‘sometimes’ do this (2/16,13%). Participant 3 could ‘sometimes’ drink from a cup (1/16, 6%).
Table 2 Age equivalent scores (years: months) on the vineland adaptive behaviour scales 3rd editionSocialisation skills (standard score median = 32, Q1-Q3 = 28–45) ranged from 0 to 9 months old when relating to others, and 0 to 7 months old with play and leisure skills (Table 2). Half of the participants (8/16, 50%) had interpersonal and leisure skills at an age equivalent of 0-months-old. Caregivers identified that most children recognised familiar people (13/16, 81%), and all participants could exhibit at least three emotions such as happy, sad, surprised, afraid (16/16, 100%). Figure 3 illustrates commonly displayed Socialisation and Motor skills.
Fig. 3
Key skills in 16 individuals with Schinzel-Giedion Syndrome as measured by the Vineland Adaptive Behaviour Scales 3rd Edition. Black shading indicates ‘usually/often’ and grey shading indicates ‘sometimes’. * = age passed away
Motor skills mirrored Daily living and Socialisation (standard score median = 20, Q1-Q3 = 20–40), across fine (v-scale subdomain score median = 1, Q1-Q3 = 1–3) and gross motor skills (v-scale subdomain score median = 1, Q1-Q3 = 1–4, v-scale subdomain score normative mean = 15, v-scale subdomain normative SD = 3). Participant 7 was the only participant who could walk (16 months old age equivalent fine motor, 7 months old age equivalent gross motor), and five participants (5/16, 31%) could scoot across the floor using all four limbs (Fig. 3). Two children used a standing frame (2/16, 13%), Whilst motor skills ranged across the group, for most individuals gross motor skills were limited to sitting with back support. In terms of fine motor skills, some participants could reach for objects (10/16, 63%) and pick up objects (6/16, 37%). Across the group, average age equivalents were 4 months old for fine motor skills (age equivalent SD = 4 months), and 2 months for gross motor skills (age equivalent SD = 2 months). Overall, the Adaptive Behaviour Composite scores across the group were also low (standard score median = 39, Q1-Q3 = 32–48).
CommunicationCommunication skills on the Vineland-3 were also severely impaired (n = 16, standard score median = 25, Q1-Q3 = 20–37, standard score normative mean = 100, standard score normative SD = 15), with most individuals having receptive and expressive language age equivalents to a 0- to 1-month-old (Table 2). Some participants exhibited receptive (v-scale subdomain score median = 1, Q1-Q3 = 1–3, v-scale subdomain score normative mean = 15, v-scale subdomain score normative SD = 3) and expressive (v-scale subdomain score median = 1, Q1-Q3 = 1–2) language skills equivalent to a 7-month-old child (Participant 1, Table 2). Average age equivalents for expressive and receptive language were 1-month-old (both age equivalent SD = 2 months). Participant age and age equivalent scores on receptive (p = 0.95, R2 = 0.00033, CI −0.32 to 0.30) and expressive (p = 0.22, R2 = 0.11, CI −0.12 to 0.47) subdomains were not associated.
Many children (13/16, 81%) could attend to someone’s voice and make happy sounds (15/16, 94%, Fig. 3). Some children would respond to their name (14/16, 88%). Participant 7 could follow simple directions, and 3/16 (19%) children responded to tone of voice (e.g., an angry or a happy tone of voice).
On the Communication Matrix (n = 16), all children used pre-intentional communication (e.g., Level 1, caregivers interpret an individual’s behaviours) to express discomfort, comfort, and interest in other people (Fig. 4). Some children could communicate intentionally (Level 2). The average percept of Communication Matrix skills mastered by the group was low (mean = 9%, SD = 4%). Refusing was a relative strength (mean skills mastered = 30%, SD = 10%), followed by communication for obtaining (mean skills mastered = 8%, SD = 5%) and social reasons (mean skills mastered = 8.28%, SD = 4%). The highest level an individual communicated at was Level 3 (unconventional behaviours, Fig. 3) and no participants could communicate for information reasons (e.g., answering yes/no questions, making comments). Participants 12 and 15 were the only participants who could request more of an object, and Participant 10 could make choices (e.g., purposefully reaching towards preferred item). Participants had a range of communication skills in their repertoires, with some individuals having > 10 methods to communicate refusal or to obtain (e.g., head, body and limb movements, facial expressions and vocalisations such as crying and screaming,), whilst others had fewer methods (i.e., three skills including whole body movement) to communicate for these reasons (Supplemental Table 1).
Fig. 4
Communication skills of 16 individuals with Schinzel-Giedion Syndrome as measured by the Communication Matrix. Y/N = Yes/No
Eight participants were currently receiving speech therapy (8/16, 50%), primarily focussing on feeding skills, such as latching and oral stimulation for feeding purposes. Participant 2 had trialled an object-picture reference system (e.g., a spoon connected to a picture of eating to indicate food/mealtimes), and a high contrast yes/no choice board, although parents reported that neither of these systems were used successfully. Two participants (2/16, 13%) used switches for cause-and-effect play, such as activating a toy with lights. Some participants (3/6, 19%) had vision therapy, which included looking at high contrast black-and-white patterns, tracking objects and exposure to coloured lights. Two caregivers commented that their child could become overwhelmed if noise and visual stimulus (e.g., lights) were presented together, and appeared to prefer either noise or visual stimulus in isolation. For sensory play preferences, seven participants (7/16, 44%) enjoyed physical touch, and six participants enjoyed music (6/16, 38%).
In terms of loss of communication skills, some caregivers (5/16, 21%) commented that their child’s interaction with others had declined over time, including previously smiling (2/16, 13%) and humming and vocalising (1/16, 6%) with eventual loss of these skills. Several caregivers (8/16, 50%) observed that their child’s skills markedly fluctuated in response to seizures and general health and worsened over time.
Comments (0)