Study population and study design
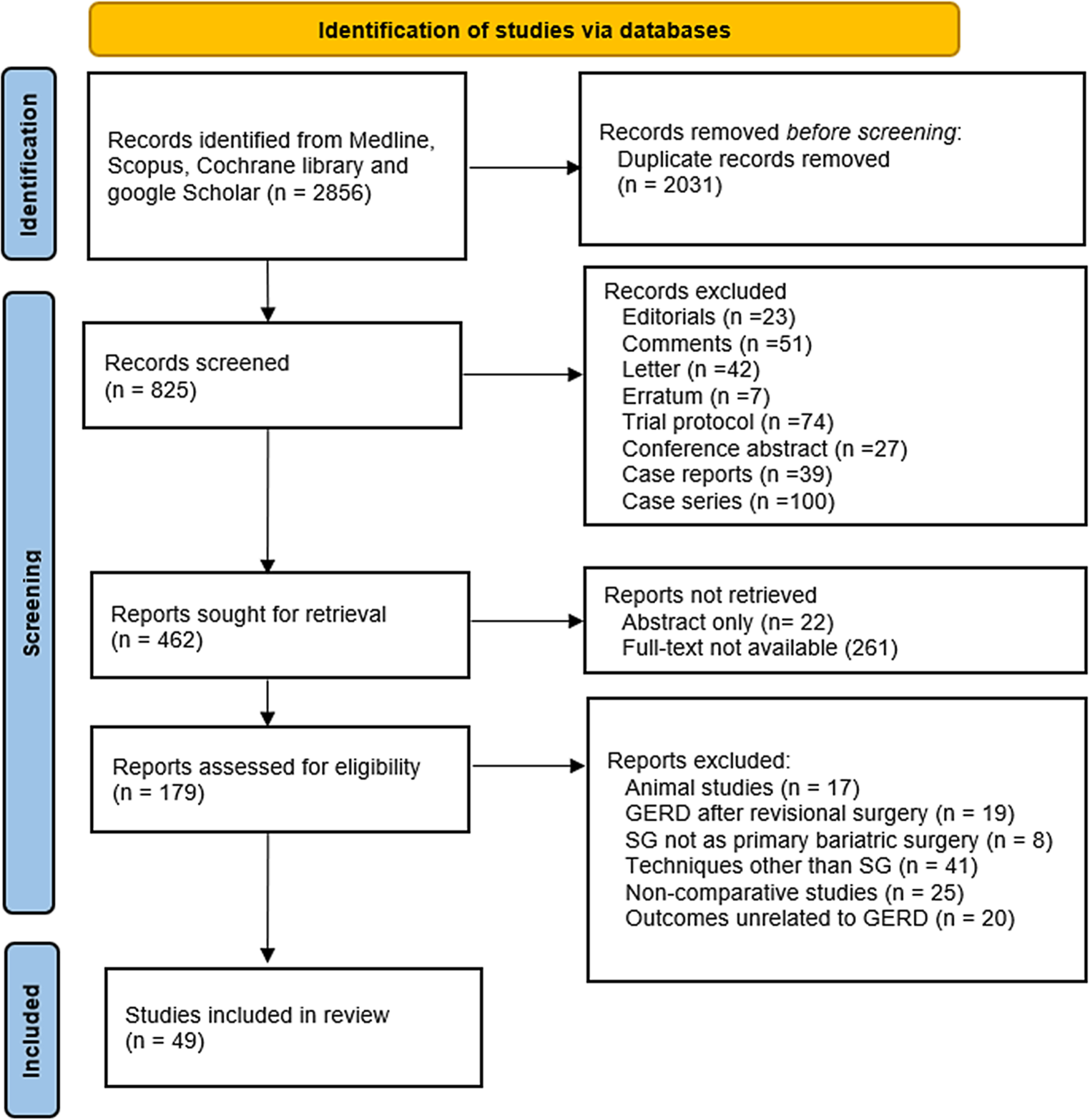
Of 171 patients who underwent Ivor Lewis esophagectomy between 2010 and 2022 at the University Hospital Oldenburg (Klinikum Oldenburg) in the Department of General and Visceral Surgery, 71 were included in this retrospective study after excluding incomplete datasets.
All histological types of esophageal cancer were included in the analysis (squamous cell carcinoma, adenocarcinoma, and undifferentiated carcinoma). Incomplete data such that the O‑POSSUM score could not be generated were excluded. Variables that were collected more than 6 months before the operation were also excluded, as recent values should be used wherever possible.
O-POSSUM score
The O‑POSSUM score is a scoring system used for preoperative risk analysis in esophageal surgery. The score contains physical components and surgical components. The physical variables include age, age group, pre-existing cardiac conditions, and pre-existing respiratory conditions, as well as electrocardiogram (ECG) changes, systolic blood pressure, pulse rate, and the Glasgow Coma Scale. Laboratory values are also included: the hemoglobin value, the number of leukocytes, the urea value, the sodium value, and the potassium value. Operative variables of the score are the surgical procedure, the urgency of the operation (classified as emergency or elective), and malignancy [14, 17].
Statistical analysis
Demographic variables such as gender, age, and tumor histology were collected, along with the surgical procedure, type of surgery, TNM stage, and the Clavien–Dindo grade. The O‑POSSUM score was calculated for the 71 patients included in the study, and mortality probability was determined based on the score using a calculator [17]. The primary endpoint considered was 30-day mortality. Binary logistic regression was used to compare mortality predicted by the O‑POSSUM score with the observed mortality. Goodness of fit was assessed using the Hosmer–Lemeshow test. A receiver operating characteristic curve (ROC curve) was constructed, and the area under the curve (AUC) was determined.
To investigate morbidity, complications were categorized according to the morbidity scale of Dindo and colleagues. Kendall’s tau was employed to assess the relationship between the points allotted by the O‑POSSUM score and the Clavien–Dindo classification. Clavien–Dindo grades were further divided into minor complications (grade I–IIIa) and major complications (grade IIIb-V), with Kendall’s tau used to test for an association between minor and major complications and the O‑POSSUM score [13, 18].
Data were obtained from the clinical database of the University Department of General and Visceral Surgery, Oldenburg Hospital. Approval from the Ethics Committee of the University of Oldenburg was obtained (approval number: AZ 2022-118). Statistical analysis was performed using IBM SPSS Statistics version 29.0 (IBM Corp., Armonk, NY, USA).




Comments (0)