
Remember me


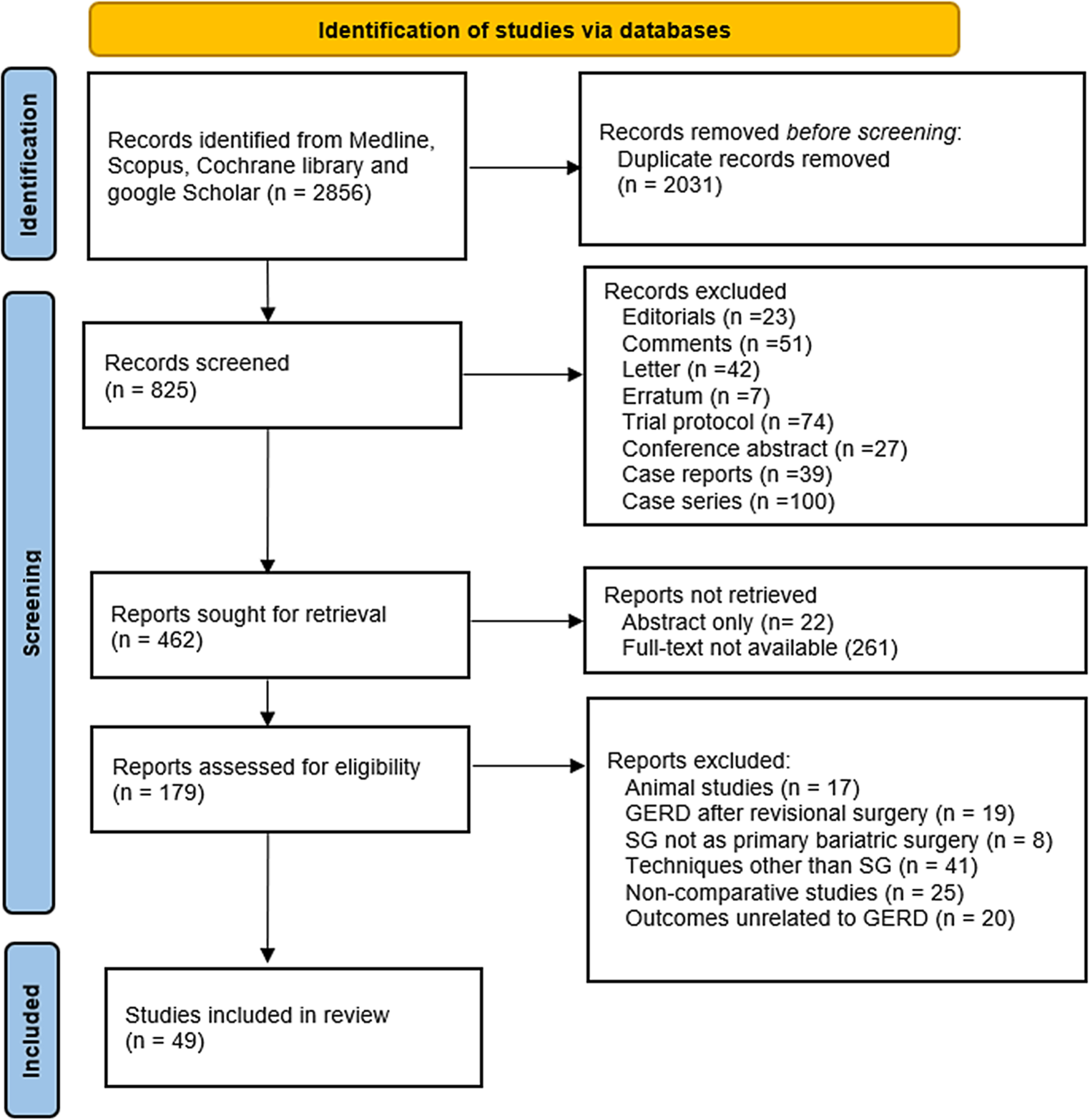

The literature search yielded 2814 studies. Following title and abstract screening, 288 studies were eligible for full-text screening, of which 37 were excluded after application of eligibility criteria because they included non-surgical cohorts (n = 16), they were letters/case reports/protocols (n = 4), they were retracted (n = 2), or the full text of the paper could not be accessed (n = 15). After manual screening of the reference lists of the included studies, 85 papers were additionally included, contributing to a total of 344 papers used for the review. The flowchart depicting the inclusion process is shown in Fig. 1.
Fig. 1
Systematic selection process for the literature review. This flowchart depicts the step-by-step process of selecting studies for the literature review, including identification, screening, eligibility assessment, and final inclusion based on predefined criteria (asterisk: excluded studies according to eligibility criteria after full-text review; circumflex accent: added studies after manual screening of reference lists of included papers)
Nutritional screening and assessmentPrevalence of malnutrition in major surgical proceduresMalnutrition is a common condition among patients undergoing major surgical procedures, with its prevalence varying significantly depending on the surgical specialty, patient case mix, and the diagnostic criteria employed in different studies. Table 2 summarizes the findings of representative studies in this review that used standardized definitions for diagnosing malnutrition. However, comparing these studies is challenging due to inconsistent definitions, which often show poor concordance. Despite these limitations, some general trends are evident. Patients undergoing pancreatic and esophagogastric surgeries exhibit the highest prevalence of malnutrition, with over half of those undergoing major organ resections for cancer being affected. Severe malnutrition rates in these groups typically range from 10 to 20%. Patients undergoing thoracic, colorectal, urological, and orthopedic surgeries are generally at a moderate nutritional risk, with overall malnutrition rates of 25–50% and severe malnutrition rates often exceeding 10%. In contrast, cardiac surgery patients are at the lowest nutritional risk, with overall malnutrition rates below 20% and minimal occurrences of severe malnutrition.
Table 2 Rates of malnutrition in selected studies using standard diagnostic definitionsThe prevalence of malnutrition is influenced by several factors beyond the anatomical site of surgery. These include advancing age; cancer diagnosis and staging; higher American Society of Anesthesiologists (ASA) classifications (> II); polypharmacy (use of > 10 medications); increased comorbidity burden; and underlying medical conditions such as severe, untreated, or poorly controlled bowel, liver, kidney, or metabolic diseases (e.g., diabetes) [27, 28]. Geriatric frailty is inherently associated with malnutrition in surgical patients. Although age alone is not always confirmed as a risk factor, the progressive decline in health and functional status associated with aging is a significant determinant of malnutrition in older individuals [29]. While cognitive decline, dementia, and psychiatric disorders are not consistently identified as risk factors for malnutrition in surgical populations, they have been extensively studied in non-surgical populations and should be considered when evaluating these patients [29].
Impact of malnutrition on outcomes in major surgical proceduresMalnutrition affects various organs and systems, leading to structural changes and functional impairments. Muscle atrophy impairs mobility, functional independence, and cardiorespiratory reserves [30]. It suppresses the immune system, particularly cell-mediated immunity, thus increasing susceptibility to infections [31]. Atrophy of the bowel mucosa compromises the intestinal barrier, heightening the risk of enteric infections, while reduced pancreatic secretion exacerbates nutritional deficiencies [32]. Anemia, commonly associated with deficiencies in iron, vitamin B12, or folate, further compromises wound healing. Additionally, the liver’s reduced capacity to synthesize proteins, including clotting factors, aggravates clinical outcomes [33]. Malnutrition is an unequivocal risk factor for poor postoperative outcomes across surgical disciplines, settings, and populations undergoing major operations [8, 13, 22, 34,35,36,37]. Malnourished patients face 2–3-times higher rates of postoperative complications, including life-threatening events, resulting in a similar increase in postoperative mortality [38, 39]. These outcomes are independent of other risk factors such as the type of surgery, patient performance status, presence of malignancy, and comorbidities [25, 40,41,42,43,44,45,46,47].
Preoperative malnutrition is a strong independent predictor of not only short-term postoperative survival but also of long-term survival in both benign and malignant conditions [39, 47,48,49,50,51]. It increases the incidence of surgical site infections [10, 52,53,54] and remote infections [15, 18, 54]. Furthermore, malnutrition is associated with hospital stays prolonged by 6 days on average [10, 22, 27, 37, 38, 47, 51, 55, 56], extended intensive care unit (ICU) admissions [18, 22, 42, 51, 57, 58], increased rates of reoperations and readmissions [18, 37, 47, 50, 59], reduced quality of life [37], impaired functional status [56, 58, 60,61,62], higher healthcare costs [55], and a greater incidence of postoperative delirium [24, 63, 64].
Screening for malnutrition in surgical patientsGiven the high volume of surgical patients and the time and resource constraints in surgical settings, applying comprehensive malnutrition assessment methods and diagnostic criteria universally is impractical, unfeasible, and cost ineffective. Screening tools offer a rational approach by stratifying patients into risk categories, ensuring that only those at a higher risk undergo detailed nutritional assessments and interventions. This strategy can significantly reduce the need for comprehensive assessments, as up to 80% of patients undergoing major surgery are typically well nourished [4, 39]. Screening enables the early identification of malnutrition risk, ideally before clinical manifestations such as organ dysfunction or complications arise. This proactive approach facilitates the timely implementation of interventions, preventing the onset of malnutrition during the perioperative period. In contrast, diagnostic methods and criteria often identify malnutrition only after it has become clinically evident, advanced, and more challenging to manage effectively.
The literature describes over 50 nutritional screening tools developed for surgical, non-surgical, and mixed populations, many of which have been individually and comparatively evaluated in various surgical settings [4, 38, 65,66,67,68,69]. Although there is no consensus on the optimal tool for surgery [2], the available evidence supports the Malnutrition Universal Screening Tool (MUST) as the most accurate for preoperative malnutrition screening [4]. The MUST incorporates body mass index (BMI), unintentional weight loss, and the presence of acute disease, categorizing patients into low, intermediate, and high nutritional risk levels ([70]; Table 3). Developed by the British Association for Parenteral and Enteral Nutrition (BAPEN) in 2003, the MUST was designed to be valid, reliable, and easy to use across all adult care settings. For patients identified as having a medium risk, BAPEN recommends documenting dietary intake for 3 days, with reassessment in 7 days if intake is adequate. For those at a high risk, referral to a nutritional specialist or implementation of interventions based on local policies and protocols is advised.
Table 3 The Malnutrition Universal Screening Tool>Methods for diagnosis of malnutrition in the surgical populationThe next step in nutritional management after screening is to confirm the diagnosis of malnutrition. Screening tools are designed to identify individuals at risk; however, their diagnostic accuracy compared to diagnostic methods is typically around 80%. This means that many patients who test positive in screening may not actually have malnutrition, leading to unnecessary interventions which may be both costly and harmful, such as establishment of a parenteral nutrition route [4, 65, 68]. Accurate diagnosis is essential for targeted, effective interventions. This approach is superior to applying generic nutritional strategies, as it enhances the evaluation of treatment outcomes and enables meaningful comparisons across different patient populations. Consequently, accurate diagnosis improves research quality, care delivery, and the rational allocation of healthcare resources.
Internationally recommended GLIM diagnostic criteria for malnutrition, as outlined in the introduction, should be employed to standardize diagnosis and facilitate comparisons of treatment outcomes and healthcare policies [2, 7]. The Subjective Global Assessment (SGA) is a diagnostic tool that evaluates 10 features derived from a patient’s history and physical examination. It has been extensively validated in nutritional studies across both surgical and non-surgical populations [71]. SGA is recognized as a valid, comprehensive method and a strong predictor of clinical outcomes in various settings. It is considered the gold standard for evaluating the diagnostic accuracy of most nutritional screening tools and has been used in validation studies for the GLIM diagnostic criteria [72,73,74]. Furthermore, the use of SGA allows for valid comparisons with historical cohorts when necessary.
Both the GLIM criteria and the SGA tool can be applied by non-nutritional specialists. However, if a diagnosis of malnutrition is confirmed, a detailed nutritional assessment by a specialist dietitian is recommended. Such an evaluation encompasses the patient’s nutritional history, clinical presentation, physical status, somatometry, biochemistry, and body composition analysis [2, 73]. Accurate diagnosis of malnutrition identifies the specific type of condition, such as micronutrient deficiency, protein–energy malnutrition, marasmus, overnutrition etc., and facilitates targeted, effective interventions [75]. This holistic approach addresses the multifaceted nature of malnutrition, which includes medical, social, and psychological parameters, and tailors interventions to the patient’s health status, age, activity level, and cultural preferences. A significant limitation of this strategy is the unavailability of dietitians in many healthcare settings. In such cases, protocolized general assessments and interventions provide a reasonable alternative.
Preoperative nutritional therapyIndicationsThe goals of preoperative nutritional therapy are to prevent the occurrence of malnutrition and its associated complications in at-risk patients and to treat malnutrition in diagnosed cases. This approach aims to prevent further deterioration and mitigate the impact of malnutrition on surgical outcomes. Current screening tools, however, were not designed to identify individuals at risk of developing malnutrition in the near perioperative period, as they were validated against simultaneously performed diagnostic methods. Developing tools specifically to identify patients in whom early intervention could prevent the onset of malnutrition should be a focus of future studies in surgical patients.
For patients diagnosed with malnutrition, preoperative nutritional therapy is reasonable and justified, and its omission would be negligent given the substantial body of evidence linking preoperative malnutrition to postoperative complications [76]. Furthermore, evidence suggests that preoperative nutritional supplementation reduces the risk of postoperative complications. However, not all clinical trials investigating preoperative nutritional therapy have exclusively included malnourished patients. It is possible that some well-nourished patients would also benefit from such interventions, as they may be protected from developing postoperative malnutrition [77, 78]. Currently, there are insufficient data to determine which well-nourished patients are most likely to develop postoperative nutritional deficiencies and whether preoperative nutritional intervention could prevent postoperative malnutrition and its sequelae. These questions present compelling areas for future research.
A particularly important subset of patients includes oncology patients who are well nourished at the time of their initial diagnosis but undergo preoperative oncological treatments which often lead to gastrointestinal symptoms as side effects, thus increasing the risk of malnutrition [79]. According to international guidelines, these patients should be screened for malnutrition at diagnosis, during treatment, and after completing treatment [80]. Patients initially identified as being at a low risk for malnutrition but scheduled for preoperative oncological therapy should undergo regular nutritional screening. While there is no definitive evidence regarding the optimal frequency of these assessments, it is reasonable to conduct them every 1–2 weeks, as a reduction in dietary intake lasting more than 1 week is a diagnostic criterion for malnutrition [2, 70, 80].
Framework and duration of nutritional interventionsPrevention and early diagnosis of malnutrition are crucial for enabling timely nutritional interventions that optimize patients’ physical status. These interventions are most effective when integrated into an enhanced recovery after surgery (ERAS) program or a prehabilitation framework [81,82,83]. This comprehensive approach has been shown to reduce postoperative complications and shorten hospital stays, as recommended by international guidelines [76,
Comments (0)