
Remember me
The management of CCA should be undertaken at centres with expertise across all relevant specialties, including surgery, interventional radiology, endoscopy, hepatobiliary medicine, oncology and pathology.
Recommendation 1: All patients with CCA discussed at multidisciplinary team (MDT) meetings should be classified as best as possible into either intrahepatic, perihilar or distal CCA. This should be clearly recorded in the MDT outcome discussion.
Strength of recommendation: STRONG
Quality of evidence: MODERATE
Recommendation 2: The requirement to have tissue available for molecular profiling to inform treatment decisions should be considered when immunohistochemistry is planned on lesional biopsy material.
Strength of recommendation: STRONG
Quality of evidence: HIGH
Recommendation 3: A diagnosis of combined hepatocellular-CCA should be made on morphological pathological grounds only.
Strength of recommendation: MODERATE
Quality of evidence: MODERATE
Recommendation 4: All centres managing patients with CCA should have clear established diagnostic pathways for patients presenting with jaundice/biliary obstruction, with streamlined transition to local and regional hepato-pancreato-biliary (HPB) MDT meetings.
Strength of recommendation: STRONG
Quality of evidence: HIGH
Recommendation 5: Having completed imaging, all patients should undergo a detailed review of clinical presentation, examination findings, blood investigations and imaging, ideally at a regionally coordinated hepatobiliary MDT meeting, with prompt assessment of the results and communication with the patient.
Strength of recommendation: STRONG
Quality of evidence: HIGH
Recommendation 6: Consideration should be given to possible benign causes of biliary tract stricturing/obstruction during MDT discussion, in correlation with appropriate serological investigations and clinical history, to ensure that alternative diagnoses are considered while a pathological diagnosis of CCA is secured.
Strength of recommendation: STRONG
Quality of evidence: MODERATE
Recommendation 7: Contrast enhanced multiphasic CT of the chest, abdomen and pelvis to stage the primary tumour, including assessment of local vascular relationships, should be undertaken for all types of CCA.
Strength of recommendation: STRONG
Quality of evidence: MODERATE
Recommendation 8: Contrast enhanced MRI and magnetic resonance cholangiopancreatography (MRCP) should be undertaken for perihilar and intrahepatic tumours to better delineate the extent of biliary involvement and identify any satellites/intrahepatic metastases.
Strength of recommendation: STRONG
Quality of evidence: MODERATE
Recommendation 9: For tumours involving the more distal extrahepatic duct, MRI is unlikely to add any further information over and above CT.
Strength of recommendation: MODERATE
Quality of evidence: LOW
Recommendation 10: 18F-fluoro-deoxy-glucose positron emission tomography ( 18FDG-PET) CT for detection of nodal and distant metastatic disease is recommended as part of staging investigations.
Strength of recommendation: STRONG
Quality of evidence: MODERATE
Recommendation 11: Ultrasound (US) or CT-guided biopsy of the primary intrahepatic tumour or metastatic lesions should be undertaken to acquire a pathological diagnosis following MDT discussion and consensus.
Strength of recommendation: STRONG
Quality of evidence: HIGH
Recommendation 12: Before undertaking any endoscopic investigations for a suspected CCA, all patients should have undergone a triple-phase CT scan of the abdomen/pelvis and chest along with dynamic MRI and MRCP if proximal biliary obstruction is suspected.
Strength of recommendation: STRONG
Quality of evidence: MODERATE
Recommendation 13: Patients with operable distal malignant tract obstruction (DMTO) should undergo a combination of endoscopic US and endoscopic retrograde cholangiopancreatography (ERCP) to try to confirm a malignant histological diagnosis before proceeding to surgery.
Strength of recommendation: MODERATE
Quality of evidence: LOW
Recommendation 14: In a suspected case of operable distal CCA, in the absence of jaundice, a standalone endoscopic ultrasound (EUS) scan should be undertaken first, to avoid the complications of ERCP, which could delay or render the patient inoperable.
Strength of recommendation: WEAK
Quality of evidence: LOW
Recommendation 15: In the presence of jaundice and DMTO, where EUS is not available, patients may only be able to have an ERCP and brush cytology in the first instance to confirm the presence of a CCA.
Strength of recommendation: MODERATE
Quality of evidence: MODERATE
Recommendation 16: At present biliary biomarkers cannot be recommended as a replacement for cytological and histological standards. However, biliary next-generation sequencing shows great promise and should be taken forward for replicative National Institute for Health Research/UK Research and Innovation (NIHR/UKRI) funded multisite studies.
Strength of recommendation: MODERATE
Quality of evidence: MODERATE
Recommendation 17: It should be realised that a cytological/histological confirmation of a malignant biliary tract obstruction (MBTO) is imperfect at present, and in cases where uncertainty remains, a decision on follow-up imaging versus surgery for a definitive diagnosis should be reached only after a full discussion between thepatient and the clinician. These guidelines acknowledge that it is acceptable to offer surgery where histological confirmation cannot exclude malignancy with absolute certainty and surgery might provide a cure and a secure diagnosis.
Strength of recommendation: STRONG
Quality of evidence: LOW
Recommendation 18: The decision to drain preoperative jaundice in distal CCA causing DMTO should be made in accordance with local hepato-pancreatico-biliary (HPB) centre guidance. In cases where rapid access to surgery can be offered, it may be appropriate to bypass biliary drainage at ERCP to avoid ERCP-related complications and postoperative sepsis.
Strength of recommendation: STRONG
Quality of evidence: HIGH
Recommendation 19: Patients with DMTO with inoperable disease from distal CCA should undergo an EUS/ERCP or standalone ERCP to confirm a pathological diagnosis and have their jaundice palliated.
Strength of recommendation: STRONG
Quality of evidence: HIGH
Recommendation 20: Patients with DMTO from distal CCA should have a fully covered self-expanding metal stent placed. Plastic stents should not be placed for long-term palliation of jaundice.
Strength of recommendation: STRONG
Quality of evidence: HIGH
Recommendation 21: Where patients cannot have a stent placed at ERCP, we recommend that EUS guided biliary drainage is undertaken rather than percutaneous transhepatic cholangiography (PTC). However, PTC can be offered if EUS bile duct drainage is not locally available.
Strength of recommendation: STRONG
Quality of evidence: HIGH
Recommendation 22: No patient with a perihilar CCA should undergo endotherapy until the case has been fully discussed at an HPB treatment centre.
Strength of recommendation: STRONG
Quality of evidence: LOW
Recommendation 23: Unilateral drainage in the future remnant lobe should be considered ahead of surgery. Bilateral/further stenting should only be considered if the level of preoperative jaundice does not improve, or there is cholangitis in residual obstructed biliary segments.
Strength of recommendation: MODERATE
Quality of evidence: MODERATE
Recommendation 24: Inoperable perihilar CCA - proximal malignant tract obstruction (PMTO) and jaundice should be considered for palliative stenting by either ERCP or PTC. Decisions about unilobar (UL) versus bilobar (BL) stenting should be predetermined by the local MDT depending on both local availability and expertise.
Strength of recommendation: STRONG
Quality of evidence: MODERATE
Recommendation 25: At present the use of adjunctive endobiliary radiofrequency ablation (RFA) and photodynamic therapy is not considered standard of care for patients with hilar and distal CCA receiving palliative care.
Strength of recommendation: STRONG
Quality of evidence: HIGH
Recommendation 26: EUS guided biliary drainage is recognised as a treatment option, but use of this technique should be planned at a MDT meeting with units adopting this approach able to show clear audit data in relation to alternative and more traditional methods of biliary drainage.
Strength of recommendation: MODERATE
Quality of evidence: MODERATE
Recommendation 27: Patients should have a clear monitoring pathway for early detection of recurrent stent blockage and on-demand endoscopic intervention.
Strength of recommendation: STRONG
Quality of evidence: LOW
Standard 28: Patients with recurrent pain after biliary stenting during their disease process should be evaluated with cross-sectional imaging. Patients with stent dysfunction should also be re-evaluated with cross-sectional imaging before any further endotherapy is undertaken.
Strength of recommendation: MODERATE
Quality of evidence: LOW
Recommendation 29: High-resolution cross-sectional imaging is essential for assessment of resectability and accurate staging.
Strength of recommendation: STRONG
Quality of evidence: HIGH
Recommendation 30: Preoperative preparation, including augmentation of the functional liver remnant (FLR) and biliary drainage, may be required to ensure safe resection.
Strength of recommendation: STRONG
Quality of evidence: HIGH
Recommendation 31: Staging laparoscopy should be used selectively.
Strength of recommendation: STRONG
Quality of evidence: MODERATE
Recommendation 32: R0 resection is the only curative treatment available.
Strength of recommendation: STRONG
Quality of evidence: MODERATE
Recommendation 33: Surgical resection of CCA should be undertaken only at high-volume centres with expertise across all relevant supporting specialties, including interventional radiology, endoscopy, hepatobiliary medicine, oncology and pathology.
Strength of recommendation: STRONG
Quality of evidence: MODERATE
Recommendation 34: Liver transplantation for selected patients with perihilar CCA (pCCA) in the presence of chronic liver disease (most commonly primary sclerosing cholangitis), less than 3 cm in size with no evidence of extrahepatic disease, results in long-term disease-free survival. This is an established indication in an increasing number of centres internationally. There is a need for evaluation of novel neoadjuvant chemoradiation strategies and assessment of long-term outcomes with national protocols and multicentre studies. Liver transplantation in the absence of background chronic liver disease remains an investigational treatment.
Strength of recommendation: MODERATE
Quality of evidence: STRONG
Recommendation 35: Neoadjuvant therapy in uncontrolled studies appears to be effective in controlling disease and selecting patients who are most likely to benefit from transplantation.
Strength of recommendation: MODERATE
Quality of evidence: LOW
Recommendation 36: Transplantation for intrahepatic CCA (iCCA) on a background of chronic liver disease precluding resection should be evaluated prospectively within a national protocol. LAG tumour size criteria to be monitored and modified to improve recruitment for evaluation.
Strength of recommendation: STRONG
Quality of evidence: MODERATE
Recommendation 37: Patients who have undergone surgical resection for CCA should be considered for 24 weeks of adjuvant chemotherapy (currently capecitabine).
Strength of recommendation: STRONG
Quality of evidence: MODERATE
Recommendation 38: The routine use of neoadjuvant chemotherapy in patients with resectable CCA is not recommended.
Strength of recommendation: STRONG
Quality of evidence: LOW
Recommendation 39: Cisplatin plus gemcitabine (CisGem) chemotherapy is recommended as the first-line treatment in patients with advanced biliary tract cancer (BTC). Immunotherapy may be added to CisGem chemotherapy, if approved and available, cognisant of the magnitude of benefit and toxicities.
Strength of recommendation: STRONG
Quality of evidence: HIGH
Recommendation 40: Combination chemotherapy is recommended in patients with adequate performance status following failure of first-line chemotherapy, particularly in the absence of a targetable molecular alteration.
Strength of recommendation: MODERATE
Quality of evidence: HIGH
Recommendation 41: CCA should be subjected to molecular profiling at the earliest opportunity, and results and treatment options should be reviewed by clinicians with appropriate expertise.
Strength of recommendation: STRONG
Quality of evidence: HIGH
Recommendation 42: Consider the use of adjuvant chemoradiotherapy for extrahepatic CCA or gallbladder cancer and a microscopically positive surgical margin resection (R1 resection) with a shared decision-making approach, considering the risk of potential harm and potential for benefit.
Strength of recommendation: MODERATE
Quality of evidence: MODERATE
Recommendation 43: Consider the delivery of stereotactic radiotherapy (SBRT) or proton beam therapy (PBT) in patients with locally advanced inoperable CCA who have received systemic therapy. Modern radiotherapy techniques should be employed to maximise radiotherapy dose and minimise toxicity.
Strength of recommendation: MODERATE
Quality of evidence: LOW
Recommendation 44a: Refer patients with symptomatic metastatic disease for consideration of palliative radiotherapy.
Strength of recommendation: MODERATE
Quality of evidence: MODERATE
Recommendation 44b: Refer for SBRT in the setting of oligometastatic disease.
Strength of recommendation: MODERATE
Quality of evidence: MODERATE
Recommendation 45: All patients with incurable CCA should have access to a palliative care assessment to fully evaluate their holistic care needs. Evidence suggests that early palliative care involvement is associated with higher health-related quality of life and lower rates of depression. Good symptom control should be delivered alongside active oncology management.
Strength of recommendation: MODERATE
Quality of evidence: MODERATE
Recommendation 46: Development and funding of clinical trials is key to fully evaluate the impact of pharmacological management of symptoms in patients with CCA and different models of care.
Strength of recommendation: MODERATE
Quality of evidence: LOW
Recommendation 47: All patients diagnosed with CCA should have access to a hepatobiliary cancer nurse specialist who can provide expertise and support to the patient and their immediate family.
Strength of recommendation: STRONG
Quality of evidence: MODERATE
Recommendation 48: All patients diagnosed with CCA should have access to a dietician.
Strength of recommendation: STRONG
Quality of evidence: MODERATE
Recommendation 49: All patients diagnosed with CCA should have timely access to high-quality information and should be diected to a dedicated CCA patient charity so that they can access support and information.
Strength of recommendation: STRONG
Quality of evidence: LOW
Recommendation 50: All patients with CCA should be enabled to access a second specialist clinical opinion if they need to seek reassurance about either their diagnosis or treatment.
Strength of recommendation: MODERATE
Quality of evidence: LOW
Scope and purposeThese guidelines have been commissioned on behalf of the British Society of Gastroenterology (BSG) liver section with the aim of updating and assisting clinicians in the diagnosis and management of patients with cholangiocarcinoma. The previous version was published in 2012.1 These guidelines do not cover gallbladder cancer or neoplasia of the ampulla of Vater/duodenum. Members of the writing committee included: gastroenterologists, hepatologists, transplant physicians, radiologists, hepatobiliary surgeons, hepatobiliary endoscopists, oncologists, histopathologists, patient representatives (from AMMF and PSC Support), and colleagues from Cholangiocarcinoma-UK (a specialist interest group within the British Association for the Study of the Liver, BASL). Where appropriate and feasible, specific clinically applicable recommendations are provided. The guidelines were reviewed and endorsed by the BSG Clinical Standards and Services Committee. We recommend this document be used in conjunction with other BSG guidelines and similar themed publications by other international bodies (such as recommendations from the European Network for the Study of Cholangiocarcinoma (ENS-CCA), the European Association for the Study of the Liver, the International Liver Cancer Association and the European Society for Medical Oncology). We also recommend revision of the guidelines in, at most, 5 years.
Evidence baseThese guidelines have been produced with a systematic review of publications identified using PubMed Medline, and Cochrane database searches. Each section of the guideline was allocated at least one lead author responsible for performing a comprehensive literature search. The literature search was updated and completed in November 2022 before submission for peer review. Where possible, guidance is based on the highest levels of evidence available. Where no high-quality studies or clear evidence exist, guidance is based on the majority consensus advice of expert opinion in the literature and the writing committee. All recommendations achieved complete consensus following extensive review and discussion among the guideline development group. The grade of evidence is presented according to the international GRADE system2 3 as follows:
High-quality evidence: The authors are very confident that the estimate presented lies very close to the true value. One could interpret it as: there is very low probability of further research completely changing the presented conclusions.
Moderate-quality evidence: The authors are confident that the presented estimate lies close to the true value, but it is also possible that it might be substantially different. Hence further research might alter the conclusions completely.
Low-quality evidence: The authors are not confident of the effect estimate and the true value might be substantially different—that is, further research is likely to change the presented conclusions completely.
Very low-quality evidence: The authors do not have any confidence in the estimate and it is likely that the true value is substantially different from it. One could interpret it as: new research will most probably change the presented conclusions completely.
All members of the guideline working group were asked to complete conflicts of interest declarations. These are available as online supplemental file 1.
BackgroundCCA is a frequently lethal liver cancer arising from epithelial cells, cholangiocytes, anywhere along the biliary tree within or external to the liver.4 5 These are exceptionally desmoplastic tumours and are enmeshed in a dense network of inflammatory cells and extracellular matrix, called the tumour immune microenvironment.6 CCA are typically classified into three subtypes according to their anatomical site of origin: intrahepatic (iCCA), perihilar (pCCA) and distal (dCCA) CCA, with pCCA and dCCA collectively referred to as extrahepatic CCA (eCCA). iCCA by definition arises within the liver parenchyma, proximal to the second order bile ducts and comprises the second most common form of primary liver cancer globally, after hepatocellular carcinoma (HCC).7 pCCA is localised between the second-degree bile ducts and the insertion of the cystic duct into the common bile duct. dCCA is confined to the common bile duct below the cystic duct insertion. Historic studies report that pCCA accounts for around 50–60% of all CCA, and iCCA accounts for less than 20% of CCA.8 These CCA subtypes are heterogeneous and can vary in their respective clinical presentations, risk factors, routes to diagnosis and clinical management, as well as exhibiting distinct epidemiological, clinical, molecular and genetic characteristics.9
Patients diagnosed with CCA have a high mortality because they typically present too late for surgical resection or transplantation, the only potentially curative options. The clinical presentation of CCA typically depends on its location. pCCA and dCCA are likely to present with obstructive jaundice as well as other constitutional symptoms. iCCA, unless extending into the hilum, tends not to present with jaundice but rather with more non-specific symptoms, such as weight loss, anorexia, abdominal discomfort, nausea and malaise. iCCA can be an incidental finding in around 20% of cases4 5—for example, during surveillance for HCC, or following imaging for another reason. A diagnosis of iCCA can also occur after resection/transplant for a tumour originally deemed to have been something else, such as an HCC or a carcinoma of unknown primary. Diagnosis of anatomical subtype can be clinically and radiologically challenging with some large CCAs which extend into the perihilar or extrahepatic bile ducts, making the site of origin unclear. How to record this uncertainty at MDT meetings in a standardised and systematic way to facilitate epidemiological studies has yet to be resolved.
Epidemiology and risk factorsRecommendation 1: All patients with CCA discussed at MDT meetings should be classified as best as possible into either intrahepatic, perihilar or distal CCA. This should be clearly recorded in the MDT outcome discussion.
Strength of recommendation: STRONG
Quality of evidence: MODERATE
Consistent findings reported over the past two decades are the rising incidence and mortality rates for iCCA and declining rates for eCCA.10–13 A recent study of the National Cancer Registration Dataset reported that almost 51 000 BTC were diagnosed in England during 2001–2018.14 CCA were the most commonly diagnosed BTC (63%) followed by gallbladder (23%) and ampulla of Vater (14%). 74% of CCA were iCCA, a higher proportion compared with historic studies. Over 95% of CCA were diagnosed in patients aged 50 years or older, with the median age at diagnosis being 75. Men and women were approximately equally affected. The age -standardised incidence rate for CCA rose from 2.9 per 100 000 population in 2001–2003 to 4.6 in 2016–2018. The rise in CCA incidence was predominantly in iCCA (figure 1) with age-standardised incidence rates increasing from 2.1 to 3.4 between 2001–2003 and 2016–2018, whereas for the same time period the rise in eCCA was from 0.6 to 1.0. There was evidence of geographical variation in CCA incidence between regional Cancer Alliances in England. The age-standardised mortality rates of CCA rose from 2.6 to 4.9 between 2001–2003 and 2016–2018 in parallel with the incidence rates. The trends for eCCA and iCCA age-standardised mortality rates mirrored those of incidence, with most deaths due to iCCA. The most common route to diagnosis was the emergency route (iCCA 50.4%, eCCA 46.1%), highlighting the late presentation of this disease. Overall survival after diagnosis of CCA was less than 10%.
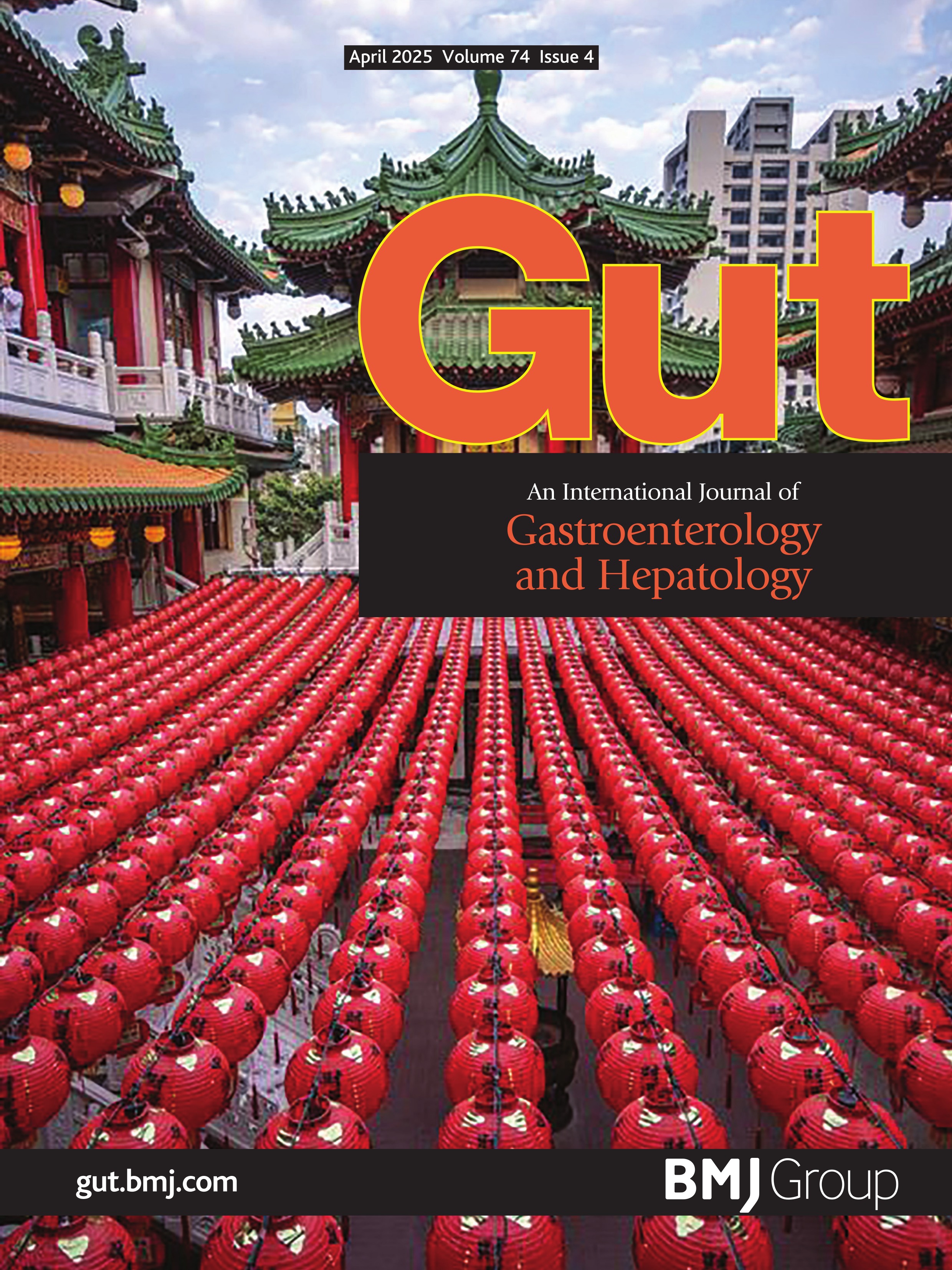
 Figure 1
Figure 1 Histopathology of intrahepatic cholangiocarcinoma (iCCA). (A) Small duct iCCA shows an anastomosing tubular architecture. (B) In large duct iCCA, columnar cancer cells with intracytoplasmic mucus are arranged in a ductal structure against the background of fibrotic stroma.
An important limitation in CCA epidemiology studies is the unknown rate of pCCA specifically, as the main WHO International Classification of Diseases (ICD) coding systems have historically lacked a specific code for pCCA, which has probably been mostly miscoded to iCCA in the past.15 The lack of specific coding for pCCA is to be corrected in the latest version of ICD (2021) but this will not help with understanding the historical rates of pCCA distinct from iCCA and distal eCCA.
Aetiology and risk factorsThe global variability of CCA prevalence is thought to be the result of a complex interaction between the host-specific genetic background and the geographical distribution of associated risk factors (table 1). The highest rates of CCA globally are in northeast Thailand and surrounding areas, where the main risk factor is believed to be chronic infection with liver flukes.9 With the absence of liver flukes in the Western world, the the most common known risk factor for CCA is primary sclerosing cholangitis (PSC).7 16 Of note, some risk factors are shared by both iCCA and eCCA, while others seem more specific for iCCA or eCCA.7 16 17 Most of the known major risk factors are associated with chronic inflammation of the biliary epithelium and bile stasis. However, the majority of CCA cases in the West are sporadic, without any identifiable risk factors present.
Table 1Risk factors for cholangiocarcinoma together with type of study (adapted from7 9 17)
Polymorphisms of host genes encoding enzymes involved in xenobiotic detoxification, DNA repair, multidrug resistance, immune response and folate metabolism have also been linked to cholangiocarcinogenesis4 9 16; however, there are currently no published genome-wide association studies in CCA.
PathologyRecommendation 2: The requirement to have tissue available for molecular profiling to inform treatment decisions should be considered when immunohistochemistry is planned on lesional biopsy material.
Strength of recommendation: STRONG
Quality of evidence: HIGH
Recommendation 3: A diagnosis of combined hepatocellular-CCA should be made on morphological pathological grounds only.
Strength of recommendation: MODERATE
Quality of evidence: MODERATE
Histological classificationIn addition to the subclassification of CCA as intrahepatic and extrahepatic, WHO 5th edition furthermore classifies lesions into benign, premalignant and malignant (box 1).18
Box 1 The range of neoplastic diagnoses in the intrahepatic and extrahepatic biliary tree in accordance with WHO 5th edition.18Intrahepatic bile ductsBenign: bile duct adenoma, biliary adenofibroma, serous cystadenoma (microcystic adenoma).
Premalignant: mucinous cystic neoplasm (MCN), biliary intraepithelial neoplasia (BilIN), intraductal papillary neoplasm of the bile duct (IPNB).
Malignant: intrahepatic CCA, IPNB with associated invasive malignancy, MCN with associated invasive malignancy.
Extrahepatic bile ductsBenign: none.
Premalignant: BilIN, MCN, IPNB.
Malignant: extrahepatic CCA, IPNB with associated invasive malignancy, MCN with associated invasive malignancy, neuroendocrine neoplasms.
Macroscopic features of CCAIntrahepatic CCA has two main subtypes, large duct and small duct.18 Large duct tumours typically arise near the large central ducts and small duct tumours are found more peripherally. Small duct tumours are usually white or grey mass-forming lesions in the hepatic parenchyma. Large duct tumours typically grow along the wall of the larger ducts from which they arise. Both forms are whiter and firmer than HCCs due to their stromal component.
There are four major patterns of macroscopic growth recognised: mass-forming, periductal infiltrating, intraductal and mixed. The majority of iCCA are mass-forming tumours, with only 10% demonstrating a periductal/intraductal pattern of growth.19 Extrahepatic CCA conversely is most commonly a sclerosing, circumferential lesion or thickening of the bile duct without clear distinction from the non-lesional duct wall. Nodular or papillary types are also found.18
Histopathological features of CCAiCCA can be subdivided into small duct and large duct. Small duct (cholangiocellular) iCCA are typically non-mucin-secreting adenocarcinomas with a ductular or tubular pattern (figure 1A). Cholangiolocarcinoma and iCCA with a ductal plate malformation pattern are considered subtypes of small duct iCCA. Large duct iCCA are typically mucin-secreting tubular adenocarcinomas resembling the perihilar and extrahepatic forms (figure 1B). Rare subtypes of eCCA can occur in large duct intrahepatic tumours. Both large and small duct forms of iCCA have a variable fibrous stroma.
Most eCCA are adenocarcinomas of pancreaticobiliary morphology with glandular structures and small groups of cells within a dense desmoplastic stroma. Other types of eCCA include: intestinal-type, foveolar-type, mucinous, signet ring, clear cell, pyloric gland, hepatoid and invasive micropapillary. Rarer types include: squamous cell carcinoma, adenosquamous carcinoma, sarcomatoid carcinoma and undifferentiated carcinoma.
Histological gradeNo definitive grading system for CCA has been accepted.20 The International Collaboration on Cancer Reporting (ICCR) guidance documents a commonly used semiquantitative grading system for iCCA based on the proportion of the tumour that shows gland formation:
>95% of tumour composed of glands: well-differentiated.
50–95% of tumour composed of glands: moderately differentiated.
<50% of tumour composed of glands: poorly differentiated.
The ICCR guidance also states that the differentiation of pCCA should be classified in the same way as distal large bile duct/pancreatic adenocarcinomas, where grading is determined by the least well-differentiated component rather than the proportion of glandular elements; it should be divided into three grades and is based on gland formation, mucin production, mitotic activity and nuclear features.
ImmunohistochemistryImmunostaining is not essential for the histological diagnosis of CCA and the increasing requirement for molecular profiling of lesional tissue to determine targeted therapies should lead to a reduction in the use of tissue for purely confirmatory immunohistochemical staining. Where imaging is in keeping with CCA, particularly the absence of prior or current extrahepatic malignancy, and the morphology is that of adenocarcinoma, there is no additional diagnostic discrimination offered by immunohistochemical staining.
However, two specific diagnostic scenarios may be aided by targeted immunohistochemistry: (1) When there is a prior history of carcinoma or a possible contemporary extrahepatic primary lesion and the morphology is compatible with both CCA and a metastasis from that prior or putative extrahepatic lesion, immunohistochemistry can be used to confirm the biliary phenotype of cancer cells and differentiate them from metastasis. To aid that particular distinction, CCA is typically positive for cytokeratin (CK) 7 and CK19, and negative for CK20. Large duct iCCA, particularly in cases associated with PSC, sometimes expresses intestinal markers (eg, CK20 and CDX2).21 C-reactive protein (CRP) is a highly specific and sensitive marker for iCCA (particularly small duct type), as it is not expressed in adenocarcinomas of other organs.22 23 The site of the prior or putative extrahepatic primary lesion allows specific cell lineage–specific transcriptional factor expression to be examined; for example, TTF-1 (expressed in lung and thyroid cancers), PAX8 (renal, thyroid, ovarian and endometrial cancers) and GATA-3 (breast and urothelial cancers) are typically negative in CCA. (2) When there is no prior or contemporary extrahepatic malignancy but the histological features are equivocal in their capacity to distinguish between CCA and HCC, immunohistochemistry may be helpful. Heppar-1, arginase-1 and glypican-3 are often expressed by HCC and not by CCA, although their expression can be lost in poorly differentiated HCCs.
If subclassification of iCCA cannot be made on morphological features alone, a panel of CRP, N-cadherin and S100 calcium binding protein P (S100P) can be useful as CRP/N-cadherin and S100P are commonly expressed in small duct and large duct iCCA, respectively.23
Molecular profileSmall duct iCCA has distinct molecular features: IDH1/2 mutations (20%), BAP1 mutations (10–20%) and FGFR2 fusions (15%).24–26 In contrast, large duct iCCA and eCCA harbour alterations in KRAS (20%) and SMAD4 (10–20%).24 25 27 Mutations in TP53 are observed in either type (30%).24 26
FGFR2, NTRK and other fusions or other rearrangements can be diagnosed by RNA sequencing (preferred to immunohistochemistry) or fluorescent in situ hybridisation (FISH), and their identification prior to the use of FGFR inhibitors is essential.28 Mismatch repair protein (MMR) or microsatellite instability (MSI) tests need to be considered if clinically indicated. MMR deficiency is observed in 1–6% of CCA, and those cases often show a solid, mucinous or signet ring cell histological appearance.29–31 NTRK fusions, a category of treatment-related, pan-cancer molecular alterations, are estimated to be detectable in 1% of CCA.32 Table 2 shows the relevant codes from NHS England Genomics that can be used for sequencing. The logistics of molecular testing to guide therapeutic decisions varies within the healthcare systems of the UK’s devolved nations. For example, testing in England is provided by the NHS England Genomic Laboratory Hubs, and the available tests are listed within the test directory (https://www.england.nhs.uk/publication/national-genomic-test-directories).
Table 2Available assays through genomics England for cholangiocarcinoma tissue
Combined hepatocellular–cholangiocarcinomaThe diagnosis of combined hepatocellular–cholangiocarcinoma requires morphological confirmation of both HCC and adenocarcinoma components.33 Immunohistochemical expressions of hepatocellular markers in otherwise typical iCCA or expressions of CK7/CK19 in HCC are insufficient alone to merit designation of tumours as combined hepatocellular–cholangiocarcinoma. CK7 and CK19 are known to be expressed in 20% and 10% of HCC, respectively.34 35 Most cases of combined hepatocellular–cholangiocarcinoma harbour gene mutations that are identified in HCC (eg, TERT) even within the CCA components.36 37 Tumour, node and metastasis (TNM) staging is currently based on that of iCCA.
Premalignant neoplasmsBiliary intraepithelial neoplasia (BilIN)Most cases of large duct CCA are thought to progress from BilIN (previous term, biliary dysplasia) via a multistep carcinogenesis.38 BilIN is diagnosed incidentally in surgically resected specimens or explanted livers. The diagnosis of BilIN in biopsy specimens should be made with caution, as BilIN is unlikely to cause biliary strictures. In contrast, premalignant lesions of small duct iCCA are unknown.
Intraductal papillary neoplasm of the bile duct (IPNB)IPNB is characterised by an intraductal high-papillary proliferation, and is currently classified into two types.39 Type 1 IPNBs develop in intrahepatic (70%) or perihilar ducts (30%), and they are typically associated with cystic or fusiform duct dilatation and mucus overproduction.39–41 Type 2 IPNBs arise in distal (70%) or perihilar ducts (30%), and present with an intraductal solid mass and extensive dilatation of the upstream ducts. The presence of invasive malignancy is confirmed in 50% of type 1 IPNBs and >90% of type 2 IPNBs at the initial presentation.39–41 The gallbladder counterpart of IPNB is referred to as intracholecystic papillary neoplasm.42
Mucinous cystic neoplasm (MCN)This condition was traditionally called biliary cystadenoma. MCN is defined as a cyst-forming epithelial neoplasm with ovarian-type subepithelial stroma and a lack of communication to the bile duct.43 44 Approximately 50% of MCNs develop in segment IV of the liver.44 Progression to CCA is confirmed in only 5% of surgically resected cases.43
Pathological diagnosisDefinitive histology and/or cytology are required to confirm a diagnosis of CCA. Even with successful lesional sampling, distinction of iCCA from metastatic lesions, particularly upper GI, pancreas, or extrahepatic biliary lesions, is difficult, as discussed earlier. Identification of an invasive component associated with a mucinous cystic neoplasm or intraductal papillary neoplasm on a needle biopsy can also be problematic due to its focal nature.44
Brush cytology from percutaneous or endoscopic procedures has a diagnostic sensitivity of only 30–60%,45 46 meaning negative cytology does not exclude malignancy. Combining cytology with biopsy increases the diagnostic yield.47 48 The further addition of FISH for polysomy and 9p21 detection increases sensitivity for the detection of malignancy further.48 49 However, in a meta-analysis examining patients with PSC, FISH did not increase the sensitivity to detect malignancy compared with cytology.50 In contrast, the addition of a 28-gene next-generation sequencing panel to pathological assessment of brushings or biopsies increased the sensitivity for the detection of malignancy in patients with and without PSC to over 80%.51
Reporting surgical specimensSurgical resection specimens should be reported systematically—for example, following The Royal College of Pathologists or ICCR reporting guidance.20 Box 2 provides a summary of how the report should be structured.
Box 2 Reporting surgical specimensSurgical resections specimens should be reported systematically—for example, following The Royal College of Pathologists or ICCR reporting guidance.20
The final report should include:
Tumour site and number: pCCA is defined as arising above the junction of the common hepatic duct and the cystic duct up to the second-order divisions of the right and left hepatic ducts. In iCCA, the number of tumours is a prognostic factor.
Maximum tumour dimension: increasing tumour size is associated with poorer prognosis.
Histological tumour type.
Histological tumour grade.
Extent of local invasion: required for TNM classification.
Presence of vascular invasion: an important prognostic factor in iCCA and pCCA, and a component of the TNM classification.
Presence of precursor lesions.
Presence of coexistent parenchymal liver disease.
Margin and lymph node status.
Pathological staging – American Joint Committee on Cancer/Union for International Cancer Control (AJCC/UICC) TNM 8th edition.20 iCCA, pCCA and dCCA are staged using separate, specific classifications (see online supplemental figures 1–3)
Additional non-core elements should also be reported:
Tumour growth pattern: mass-forming, periductal infiltrating, intraductal or mixed.
Presence of perineural invasion: of greatest significance in perihilar tumours.
Response to neoadjuvant therapy.
PresentationRecommendation 4: All centres managing patients with CCA should have clear established diagnostic pathways for patients presenting with jaundice/biliary obstruction, with streamlined transition to local and regional HPB MDT meetings.
Strength of recommendation: STRONG
Quality of evidence: HIGH
Recommendation 5: Having completed imaging, all patients should undergo a detailed review of clinical presentation, examination findings, blood investigations and imaging, ideally at a regionally coordinated hepatobiliary MDT meeting, with prompt assessment of and communication to the patient.
Strength of recommendation: STRONG
Quality of evidence: HIGH
Recommendation 6: Consideration should be given to possible benign causes of biliary tract stricturing/obstruction during MDT discussion, in correlation with appropriate serological investigations and clinical history, to ensure alternative diagnoses are considered while a pathological diagnosis of CCA is secured.
Strength of recommendation: STRONG
Quality of evidence: MODERATE
Most patients with a CCA will typically present through either emergency services or via referral to a secondary care centre on a 2 week-wait upper GI or jaundice related pathway.14 For patients presenting with eCCA, malignant biliary tract obstruction is a common mode of presentation. Following this, an imaging investigation followed by discussion at a local/regional hepato-pancreato-biliary MDT meeting is likely to occur, where a plan will be made on how to achieve: (1) a histological diagnosis, (2) restore bile flow for those patients with jaundice, (3) determine if the patient is an operative candidate, (4) determine what other imaging tests are required for subsequent patient management.
With regards to tissue sampling, a biopsy/cytological sample may be taken from the following sites to secure a diagnosis of CCA: a biliary stricture, periductal/intrahepatic mass lesion, lymph node metastasis, organ metastasis, pathological serosal fluid sample (pleural fluid, ascites, pericardial fluid) or peritoneal biopsy.
Malignant biliary tract obstruction can present with a wide range of symptoms that include: abnormal liver function tests, jaundice, abdominal pain, tiredness/lethargy, anorexia plus weight loss, thromboembolic disease, hypercalcaemia, paraneoplastic syndromes, abdominal masses/distant organ infiltration, malignant adenopathy, pleural disease, ascites and fever of unknown origin.1 4 5 At presentation, both distal and hilar biliary strictures essentially remain indeterminate until there is either a positive cytological or histopathological confirmation of CCA, with ultimately, over 80% of such strictures proving to be malignant.52
It is imperative that all patients presenting with possible MBTO have a detailed history taken in reference to age of presentation, country of origin, travel history, constitutional symptoms and weight loss, history of prior HPB surgery, pancreatitis, or inflammatory bowel disease, family history of inflammatory bowel disease, previous investigations to detect possible causes of indeterminate biliary strictures and history of chronic liver disease including viral hepatitis. Benign causes of a cholangiopathy/biliary stricturing should also be considered with appropriate collaborative serological testing for diseases which can mimic CCA (box 3).
Box 3 Benign diseases which can mimic cholangiocarcinomaRecurrent pyogenic cholangitis
Mirizzi syndrome
Stricture in primary sclerosing cholangitis
Portal hypertensive biliopathy
Heterotopic tissue
Ischaemic cholangiopathy
Inflammatory-infiltrative
Inflammatory pseudotumour
IgG4 sclerosing cholangitis
Eosinophilic cholangiopathy
Mast cell cholangiopathy
Follicular cholangitis
Xanthogranulomatous cholangitis
Sarcoidosis
A detailed family history should also be undertaken to exclude familial cancer syndromes that are associated with CCA. In a study of 267 patients, over 15% of patients had a pathogenic/likely pathogenic somatic variant in a cancer risk gene including: ATM, CHEK2, BAP1, BRCA1, MLH1, BRCA2, PALB2, TP53, APC, CDH1, MSH6, PMS2 and MUTYH.53
If a familial cancer syndrome is suspected from the patient’s genetic history, we would recommend that the patient is referred to a clinical geneticist. Things that might alert clinicians to this include: (1) three or more primary cancers in a single individual, (2) three or more cases of cancer at the same site, (3) any two of: sarcoma, breast cancer, brain tumour, leukaemia or adrenal cortical tumour, in someone under 45, (4) childhood cancer plus one close relative with cancer, (5) any individual or family with an unusual pattern of cancer—for example, rare tumours or young ages at diagnosis, (6) families with a known cancer predisposition syndrome for example, Li-Fraumeni, Lynch syndrome and Peutz Jeghers, (7) people who meet diagnostic criteria for familial genetic syndromes.
ImagingRecommendation 7: Contrast enhanced multiphasic CT of the chest, abdomen and pelvis to stage the primary tumour, including assessment of local vascular relationships, should be undertaken for all types of CCA.
Strength of recommendation: STRONG
Quality of evidence: MODERATE
Recommendation 8: Contrast enhanced MRI and MRCP should be undertaken for perihilar and intrahepatic tumours to better delineate the extent of biliary involvement and identify any satellites/intrahepatic metastases.
Strength of recommendation: STRONG
Quality of evidence: MODERATE
Recommendation 9: For tumours involving the more distal extrahepatic duct, MRI is unlikely to add any further information over and above CT.
Strength of recommendation: MODERATE
Quality of evidence: LOW
Recommendation 10: 18FDG-PET CT for detection of nodal and distant metastatic disease is recommended as part of staging investigations.
Strength of recommendation: STRONG
Quality of evidence: MODERATE
Recommendation 11: US or CT-guided biopsy of the primary intrahepatic tumour or metastatic lesions should be undertaken to acquire a pathological diagnosis following MDT discussion and consensus.
Strength of recommendation: STRONG
Quality of evidence: HIGH
In the diagnosis and staging of suspected CCA, the local tumour extent, vascular/biliary involvement, anatomic variations of the vessels/biliary tree and presence or absence of extrahepatic disease should be assessed. A multimodality approach is often required to combine the advantages of the various imaging techniques, which provide additive information.54–56
Imaging studies should be performed before any biliary intervention to avoid secondary inflammatory change that can mask the tumour and lead to overestimation or underestimation of its true extent.56 All imaging modalities can underestimate the longitudinal tumour extent owing to microscopic spread along the mucosal/submucosal layer of the bile duct.57
Transabdominal ultrasound (TUS)Cholangiocarcinoma should be suspected when there is biliary ductal dilatation, particularly with a related mass and consistent clinical history. In suspected biliary obstruction, TUS is reliable for excluding gallstones but is operator-dependent and is insufficient alone for investigating suspected CCA. For detecting advanced CCA in patients with PSC, TUS offers specificity and negative predictive value of 90%, but sensitivity and positive predictive value are only 50%.58 59 TUS may miss small tumours and cannot accurately define tumour extent.58 60 The role of contrast enhanced ultrasound (CEUS) in CCA is also limited but might be helpful as an additional modality when assessing indeterminate focal liver lesions.
Contrast enhanced computed tomography (CECT)Contrast enhanced computed tomography (CECT) should be performed in all cases of suspected CCA as the initial standard imaging modality, to include the chest, abdomen and pelvis. The main advantage is the excellent spatial resolution, providing comprehensive assessment of the primary tumour, its local vascular relationships (including any aberrant vessels) and overall resectability.56 61 62 It also allows detection of local lymphadenopathy and metastatic disease, although sensitivity is lower than that of PET.63 A meta-analysis including 448 patients from 16 studies, found data primarily related to CT, with accuracy estimates for CT evaluation of the extent of ductal tumour to be 86%; the sensitivity and specificity estimates were 89% and 92% for evaluation of portal vein involvement, 83% and 93% for hepatic artery involvement, and 61% and 88% for lymph node involvement, respectively.54
A multiphase examination of the abdomen including an unenhanced, arterial and portal venous phase is ideal. The unenhanced phase helping to differentiate high-attenuation calcified stones from enhancing tumour. Multiplanar reconstruction should be routinely used.64 Assessment of vascular involvement on CT is more difficult for the hepatic artery than the portal vein, with variable positive predictive values reported for the former ranging from 53% to 95%.56 65 66 Assessment of the extent of biliary involvement can also be difficult with CT, particularly the proximal extent of perihilar tumours.
Magnetic resonance imaging (MRI) and magnetic resonance cholangiopancreatography (MRCP)A meta-analysis of 32 studies with 1626 patients reported a pooled sensitivity and specificity of MRI for T-stage of 0.90 and 0.84, and pooled sensitivity and specificity for N-stage of 0.64 and 0.69, respectively.67 In a recent study of 334 patients comparing CT and MRI staging of mass-forming intrahepatic CCA, MRI showed superior sensitivity for T-staging, with CT and MRI having comparable sensitivity for N-stage.
Comments (0)