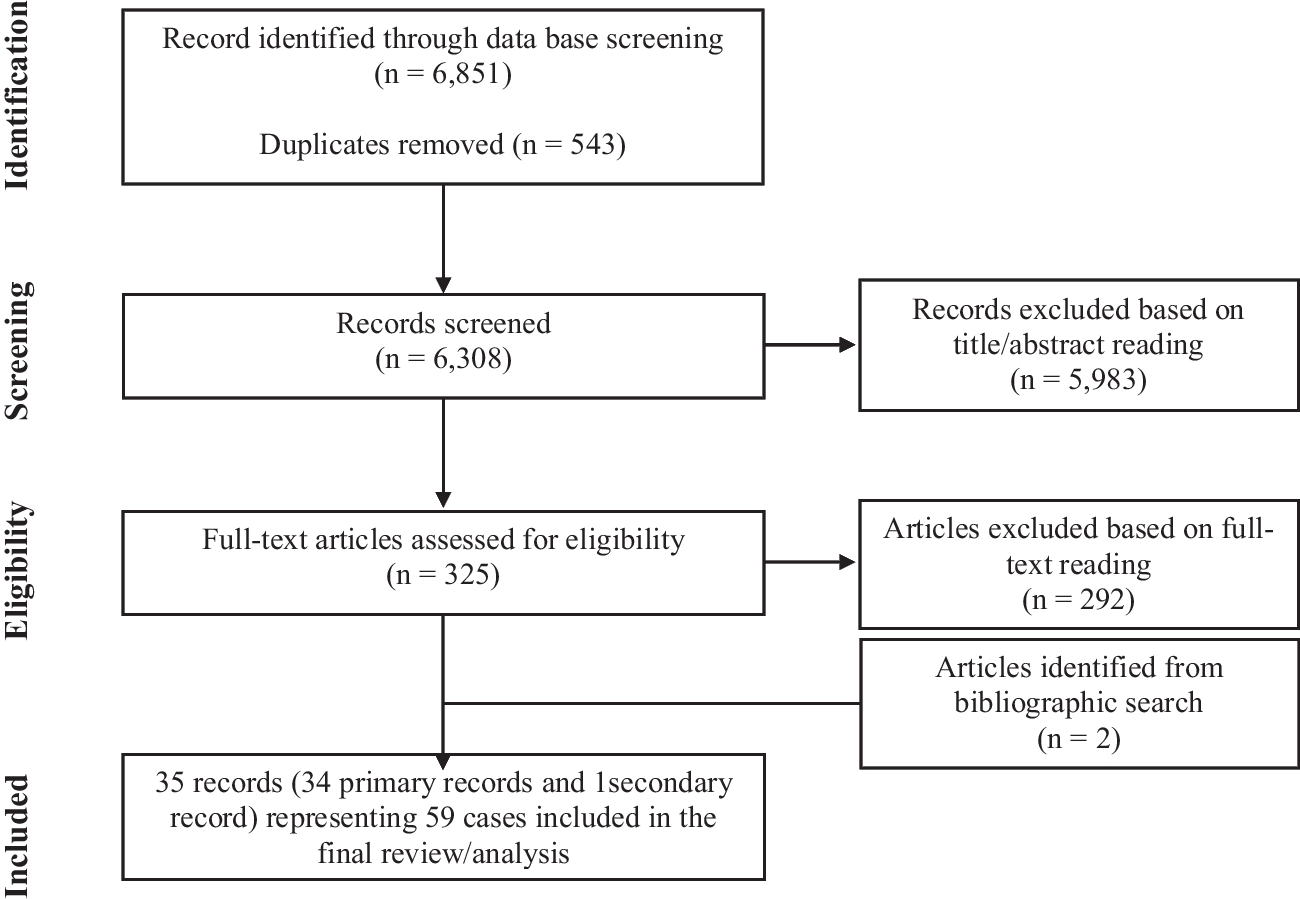
Based on the search strategy, 30 papers were identified; 12 papers were removed because duplicates; 18 full-text papers were fully analyzed, and eight papers were finally included in the review (Fig. 1).
The majority of studies were carried out in the US [31,32,33,34,35,36,37] in the period 1968–2021 and published in peer-reviewed international scientific journals, such as the American Journal of Psychiatry or Bipolar Disorder (Table 1).
The most common false myths, which have been critically revised, are the following: (1) lithium is not the first choice for treating patients with bipolar disorder; (2) lithium should be avoided in adolescents or elderly patients due to its side effects; (3) the risk of drug–drug interactions is one of the most common limitations in lithium treatment; (4) weekly lab tests are required during treatment with lithium; (5) different lithium formulations do not modify its tolerability profile; (6) no drug has antisuicidal effects; (7) lithium should be avoided during pregnancy (Table 2). The following statements, based upon the most recent evidence on lithium treatment, are proposed: (1) lithium should represent the first choice for the treatment of patients with bipolar disorder; (2) lithium treatment is effective in different patients’ groups, including young and elderly patients; (3) the risk of drug–drug interaction during lithium treatment can be easily managed; (4) the optimal management of lithium treatment includes periodical laboratory tests; (5) slow-release lithium formulation has advantages compared to immediate release formulation; (6) lithium has an antisuicidal effect; (7) lithium can be carefully managed during pregnancy.
Table 2 Myths and facts about lithium treatment in psychiatric practiceMyth 1: lithium is not the first choice for treating patients with bipolar disorderFact 1: lithium should represent the first choice for the treatment of patients with bipolar disorder
Lithium plays a relevant role in acute and long-term management of bipolar disorder and must considered as first-line treatment [38]. In fact, lithium increases the duration of free intervals, minimizes the risk of recurrences and improves inter-episodic symptomatology. Nowadays, lithium is still the gold standard in studies evaluating the efficacy of various medications in the long-term treatment of recurrent mood disorders [39].
Available evidence strongly indicates that patients suffering from bipolar disorder should be primarily treated with lithium, using other mood stabilizers as add-on in case of partial response [40]. Moreover, lithium treatment should be started as early as possible, since response rates for mania and for long-term treatments decrease in individuals with more than three episodes [41]. Maintenance treatment with lithium should be started after two hypomanic episodes or even after one severe psychotic, manic or mixed episode [42].
Patients should be educated about the many benefits of a long-term treatment with lithium, in terms of prophylaxis of mood episodes, reduction of suicidal risk, and neuroprotective effects, with a probable reduction of the risk of dementia and a potential protection against cognitive impairment that is a long-term consequence of multiple mood episodes [43].
Myth 2: lithium should be avoided in adolescents or elderly patients due to its side effectsFact 2: lithium treatment is effective in different patients’ groups, including young and elderly patients
Lithium represents the gold standard for the treatment of adult with bipolar disorder, but its role in treating bipolar disorder in childhood or adolescence is still debated.
Amerio et al. [44] concluded that lithium monotherapy is safe and effective for acute mania and for the prevention of affective episodes in children and adolescents. A recent umbrella review highlighted that lithium is reasonably safe and effective in children and adolescents, with adverse events similar to those observed in adults; however, the authors underlined that available evidence is limited, and further studies are needed [45].
Optimal dosing strategies have been extensively studied in the pediatric literature. In children weighing > 30 kg, due to the shorter half-life elimination and the greater creatinine clearance, the dosing strategy with lithium begins at a dose of 300 mg daily, followed by a 300 mg weekly increase, until it reaches serum lithium levels ranging from 0.8 to 1.2 mmol/l, similar to those of adults [46]. This strategy yielded mean total daily doses of 1500 mg (SD = 400.9 mg) and a mean weight-adjusted total daily dose of 29.1 mg/kg/day.
According to the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) study, lithium is prescribed more frequently to adult (37.8%) than to elderly bipolar patients (29.5%) [47]. However, because elderly subjects are often excluded from randomized clinical trials, studies focused on the treatment of bipolar disorder in older age are lacking and the information is mainly based on data derived from mixed age populations [48, 49]. A growing attention is being given to a subset of patients with bipolar disorder, defined “older age bipolar disorder” (OABD), i.e., bipolar patients aged 50 years and over with prevalent cognitive deficits, increased risk of dementia, impaired psychosocial functioning, frequent physical comorbidities, and premature death [50, 51]. In a double-blind, randomized, controlled trial in elderly patients with bipolar disorder, lithium was more effective than valproate in reducing manic symptoms during a 9 week follow-up and both drugs were similarly well tolerated [52].
Recently, it has been proposed that optimal serum levels of lithium in elderly patients between 60 and 79 years should be 0.4–0.8 mmol/l, while in patients aged 80 or more lithium levels should be between 0.4 and 0.7 mmol/l [53]. In the case of physical comorbidities, polypharmacy, cerebrovascular diseases, parkinsonism and dementia, a serum lithium concentration equal to or lower than 0.5 mmol/l (measured after 12 h) is recommended [54].
A dose reduction of lithium of about 20% is often required in elderly patients compared to younger patients. However, for maintenance monotherapy in OABD lithium is effective and well tolerated and it still represents the preferred choice, if correctly used. However, special caution is required to prevent nephropathy and intoxication.
In the elderly, lithium seems to be used more frequently as add-on to antidepressants in the treatment of resistant depression than in bipolar disorder [55]. Long-term treatment with lithium in the elderly is effective and relatively well tolerated both in patients with bipolar disorder and in those suffering from resistant depression. Morlet et al. [56] found that patients with depressive and bipolar disorder who had taken lithium in previous years (12.5 years on average) had less severe psychiatric symptoms, less severe depressive symptoms, and less use of benzodiazepines compared to those who had not received lithium therapy. Except for hypothyroidism, patients taking lithium have no more side effects compared to those not taking lithium.
Myth 3: the risk of drug–drug interactions represents one of the most common limitations in lithium treatmentFact 3: drug–drug interaction risk can be easily managed during lithium treatment
Drug–drug interactions with lithium can be pharmacokinetic or pharmacodynamic in nature.
As regards pharmacokinetic interactions, lithium has a narrow therapeutic index and changes in plasma concentrations can have significant clinical consequences. The ion is extensively absorbed in the gastrointestinal tract, is not metabolized and is almost entirely eliminated by the kidneys [57]. Serum lithium levels are sensitive to physiological factors that affect renal function, including age, dehydration, sodium balance; the most important drug interactions occur when co-administered drugs alter renal function, specifically modifying glomerular filtration and tubular reabsorption.
The most commonly prescribed drugs that have the potential to interact with lithium are ACE inhibitors, angiotensin-II receptor antagonists (sartans), diuretics, and non-steroidal anti-inflammatory drugs (NSAIDs) [58] (Table 3).
Table 3 Lithium drug–drug interactionsCase reports and hospital admission studies have shown that ACE inhibitors and angiotensin-II receptor antagonists can increase lithium serum concentrations, thus increasing the risk of toxicity [59]. Closer monitoring of lithium concentrations is needed when people start either of these drugs, and lithium dose probably needs to be reduced until a stable therapeutic concentration has been achieved. Closer monitoring for several days is also required when those drugs are stopped.
Lithium concentrations must be carefully monitored when a diuretic drug is prescribed. Thiazide and thiazide-like diuretics increase sodium reabsorption, which decreases the clearance of lithium and significantly elevates its serum concentrations [60]. Amiloride is recommended as a diuretic because of its mechanism of action that reduces lithium accumulation and improves kidney function in long-term treatment [61].
Patients taking lithium should be advised not to use regularly nonsteroidal anti-inflammatory drugs (NSAIDs) that can alter lithium concentrations through multiple mechanisms [62]. If NSAIDs are indicated, they should be used under medical guidance with a close monitoring of lithium concentrations; in these cases, lower lithium doses may be required.
Accelerating lithium elimination can be obtained through decreasing lithium reabsorption in the proximal tubule by osmotic diuresis (e.g., mannitol), carbonic anhydrase inhibitor, acetazolamide, and sodium bicarbonate [63]. Some calcium-channel blockers, such as nifedipine or nimodipine, can increase lithium clearance by producing afferent arteriolar vasodilatation. A similar effect is produced by xanthines, such as aminophylline, theophylline, and caffeine. Abrupt withdrawal from excessive drinking of coffee or tea may decrease lithium clearance, which may result in intoxication [57].
When combining lithium with other mood stabilizers, such as carbamazepine, valproate or lamotrigine, there is no significant influence on the levels of each drug; furthermore, combinations with tricyclic antidepressants are pretty safe [64].
Increased lithium neurotoxicity can be caused by the interaction with many drugs, particularly if they are administered at high doses and in elderly patients. These drugs include first (chlorpromazine and other phenothiazines, haloperidol) and second-generation antipsychotics (clozapine, olanzapine, quetiapine, risperidone, paliperidone, aripiprazole, and brexpiprazole). Lithium and antidopaminergic drugs can induce a profound dopamine hypofunctionality as a causative mechanism for neurotoxicity, resulting in increased risk of extrapyramidal symptoms, neuroleptic malignant syndrome and tardive dyskinesia [65].
Other interactions include the enhancement and prolongation of the action of competitive (e.g., pancuronium) and depolarizing (succinylcholine) muscle relaxants which, in rare cases, can trigger attacks of congenital muscle fatigue [66].
Patients with bipolar disorder often receive specific medications for treating comorbid physical conditions, such as obesity, hypertension and cardiovascular disorders. Therefore, interactions between lithium and those medications are frequent.
In patients with high blood pressure treated with certain diuretics, i.e., thiazide diuretics, ACE-inhibitors, and angiotensin-II receptor antagonists, or undergoing low sodium diet, serum levels of lithium might increase up to toxic concentrations. Therefore, different therapeutic options, i.e., loop diuretics, should be considered in these patients [67].
Although caution is required when prescribing lithium to subjects with cardiovascular diseases, such as arrythmias and QT prolongation, especially with concomitant electrolyte imbalances [53], Ponzer et al. [51] found a lower risk for cardiovascular and cerebrovascular diseases in BD patients receiving lithium.
Since lithium pharmacokinetics and body distribution change with body weight, larger maintenance doses may be required in obese patients. Therefore, a strict monitoring of the onset of potential side effects of lithium [68] is recommended.
According to the most recent recommendations, a target serum lithium concentration range of 0.5–0.8 mmol/L (varying upon clinical indication, age, and concurrent physical status) seems most appropriate for most patients. Lower end levels of the therapeutic range (0.5–0.6 mmol/L) are generally recommended for older patients (50 years and over) and for those taking interacting concomitant medications for other risk factors such as heart disease, renal impairment, diabetes insipidus, thyroid dysfunction [67].
Lithium should be prescribed with caution in patients receiving drugs that can slow its renal elimination and increase the risk of toxic effects (e.g., thiazide diuretics, ACE-inhibitors, angiotensin converting enzyme inhibitors, NSAIDs, when assumed more than occasionally and for extended periods), and if a low-sodium diet is required for medical reasons [53].
Kuramochi et al. [69] investigated the administration rates of NSAIDs, loop/thiazide diuretics, angiotensin-converting enzyme inhibitors, and/or angiotensin-II receptor blockers between lithium users and age- and sex-matched non-lithium users. They also investigated the number of patients in the two groups with a diagnosis of somatic conditions who were receiving those medications. Results show that prescriptions of the above medications are less frequent in lithium users compared to non-users (18.3 vs. 31.9%), with subsequent suboptimal treatment of medical comorbidities and impact on physical health.
The presence of alcohol use disorders (AUD) and substances use disorders (SUD) should always be considered when initiating a treatment with lithium [70, 71]. Lithium is still considered the first-line treatment in comorbid BD-AUD/SUD patients who show good adherence. Also, medications for AUD can be safely used in BD given the lack of significant pharmacological interactions [72]. However, in these patients the combination of more drugs is often the rule for improving patients’ outcome. For example, in patients affected by bipolar disorder with AUD/SUD, adding an anticonvulsant drug to lithium is preferable to lithium monotherapy for their effects on substance consumption and craving [73]; the combination of lithium and valproate is effective for affective symptoms and reduces substance use, possibly through an indirect effect on mood stability [74]. Nevertheless, studies are still scarce, findings are often inconsistent and with no difference according to the main substance of use [70]. Further studies are needed before evidence-based guidelines can be delivered for clinician's use.
Myth 4: lithium treatment requires weekly lab testsFact 4: the optimal management of lithium treatment includes periodical laboratory tests
Lithium treatment can be easily implemented in ordinary clinical practice, both at inpatient and outpatient settings. Before starting treatment with lithium, it is recommended to assess blood concentrations of creatinine and urea-nitrogen (to check renal functioning), the levels of electrolytes (sodium, potassium, calcium), and the levels of thyroid and parathyroid hormones, as well as obtaining an electrocardiogram. Lithium blood concentration should be checked 5 days after the targeted dose is achieved. The evaluation of lithium blood concentration levels can be repeated until lithium reaches its therapeutic levels. Afterwards, lithium, creatinine, and TSH levels should be checked every one to 2 months in the first 6 months, and then every 6–12 months, or as clinically indicated.
The most common early side effects of lithium include reduced urinary concentrating ability (by 15% of normal maximum) with possible polyuria/polydipsia, tremor, and gastrointestinal symptoms. Clinical hypothyroidism and/or increased thyroid stimulating hormone (TSH), parathyroid abnormalities (usually normocalcemic hyperparathyroidism), impaired glomerular filtration rate and chronic kidney disease usually occur after a long-term exposure to lithium [75,76,77].
Some of lithium acute side effects can be reduced simply by ensuring that the lowest needed plasma levels are maintained and using prolonged-release formulations that are associated with lower plasma peaks.
In the long term, lithium is associated with a higher risk of impaired glomerular rate filtration and chronic kidney disease stage 3 (GFR < 60 mL/min/1.73 m2) as compared to valproate, olanzapine and quetiapine (but not CKD stage 4—GFR < 30 mL/min/1.73 m2); but lithium is significantly less associated with weight gain and hypertension than other mood stabilizers (e.g., valproate, olanzapine and quetiapine) [78]. Long-term antipsychotic exposure, especially some of the most used atypical antipsychotics such as olanzapine or quetiapine, is indeed associated with increased rates of obesity, metabolic syndrome and cardiovascular diseases, with an excess of mortality due to cardiovascular events [79]. Moreover, long-term exposure to dopamine-blocking agents may have an impact on brain’s reward system and on the extrapyramidal system.
In a small group of patients, lithium is associated with hypercalcemia or normocalcemic hyperparathyroidism (risk of reduced mineral density, osteoporosis and increased fracture risk over the long-term), but their clinical significance remains doubtful. In fact, opposite findings have been found recently, with decreased risk of osteoporosis (HRR, 0.62; 95% CI 0.53–0.72) in bipolar patients treated with lithium compared to those not receiving lithium. Treatment with antipsychotics, valproate, and lamotrigine was not associated with reduced risk of osteoporosis [80]. Concerning clinical hypothyroidism, annual TSH measurements may be sufficient to prevent overt hypothyroidism; in any case, thyroid function abnormalities should not constitute an outright contraindication to lithium treatment, as well as lithium should not be stopped if a responsive patient develops thyroid abnormalities [81, 82].
No studies have been performed to date evaluating the long-term effect of exposure to prolonged-release lithium versus immediate-release lithium on thyroid and renal function; however, one can expect that the lower peak plasma levels and the smaller peak-to-through plasma differences of the prolonged-release formulations are associated with a preserved thyroid and renal function.
Concerning adverse effects associated with lithium treatment, some clarifications need to be made. First, severe adverse renal and endocrine outcomes are very rare (although the absolute risk is higher and significant, the absolute number is low). According to a study in two regions of Sweden with 2.7 million inhabitants [83], renal replacement therapy in patients exposed to lithium occurs in 0.53% as compared to 0.08% in the general population (1.2% in those on lithium for more than 15 years), while a more recent study found that chronic kidney disease occurs in 0.6% of patients (median treatment time 19 months) [84]. Moreover, adverse renal consequences are associated with higher mean plasma levels (greater than 0.60–0.70 mEq/L) [85, 86], indicating that a regular monitoring of plasma levels can minimize or even neutralize the risk. Practical guidelines for prevention and management of renal side effects of lithium therapy advise to use a once-daily dosing schedule, which allow an effective treatment while preventing lithium intoxication [87].
Myth 5: different formulations of lithium do not modify its tolerability profileFact 5: slow-release lithium formulation has advantages compared to immediate release formulation
Conventional slow-release (SR) lithium preparations provide a modulated release of the active ingredient, that is obtained for the reduced solubility of the saline compound used (lithium sulphate), or with the inclusion of lithium in a less easily absorbable matrix. In both cases, lithium is absorbed more slowly, and the peak plasma concentration, which is lower than the immediate-release (IR) formulations, occurs within 4–12 h; the pharmacokinetics, therefore, follow a plateau.
The slower increase in serum lithium concentrations and the lower Cmax (maximum concentration of drug detected in the blood) with SR formulations compared to IR lithium formulations translate into a reduced rate or less severity for some lithium-related adverse events, including tremors, upper gastrointestinal cramps, nausea, rash, cognitive obtundation, polyuria; a close relationship between changes in blood lithium levels and frequency and severity of side effects has been recently highlighted. Pompili et al. [88] found that SR lithium salts offer clinical advantages over IR formulations in terms of more stable circulating concentrations of lithium, less adverse impact on renal function, low incidence of adverse neurological effects (including cognitive impairment and tremor), low subjectively unpleasant adverse effects such as fatigue and weight-gain, and greater treatment adherence.
Slow-release formulations reduce the post-absorption peaks of plasma levels, which is beneficial for patients with gastric upset or transient side effects (e.g., tremors) secondary to temporary increases in blood levels.
Long-term treatment with SR lithium is associated with less impairment of the kidney's function to concentrate urine compared with IR lithium. A drug delivery system designed to achieve prolonged therapeutic effects by continuously releasing the medication over an extended time after the administration of a single dose reduces daily peaks in plasma lithium concentrations, thus preserving the functionality of the kidney.
A worsening of lower gastrointestinal disorders (e.g., diarrhea) has been occasionally reported with SR formulations of lithium compared to IR formulations [89].
A single daily administration of lithium can produce benefits compared to repeated daily administrations regarding adherence to therapy and reduction of renal and thyroid side effects. Double administration of lithium during the same day could produce renal impairment and a higher risk of polyuria [90]. A single evening dosage is recommended, allowing greater treatment adherence [38].
The overall decrease in adverse events with SR formulations compared to lithium IR formulations may reduce drug discontinuation, although this factor has not been evaluated in controlled clinical studies [90,91,92,93].
Prolonged-release lithium sulphate represents a therapeutic option of great advantage for the clinician, as it allows for constant plasma concentrations of lithium while minimizing the undesirable effects associated with concentration peaks of standard-release formulations [94]. Furthermore, in the event of an overdose of slow-release preparations, the chances of survival increase [95].
According to Bowden [89], adverse effects of lithium can be resolved by dose reduction, extended-release lithium, or combination therapy.
Barbuti et al. [96] investigated differences between patients receiving IR (lithium carbonate) vs. SR (lithium sulphate) lithium formulations in a prospective naturalistic study. Both lithium formulations significantly improved



Comments (0)