
Remember me

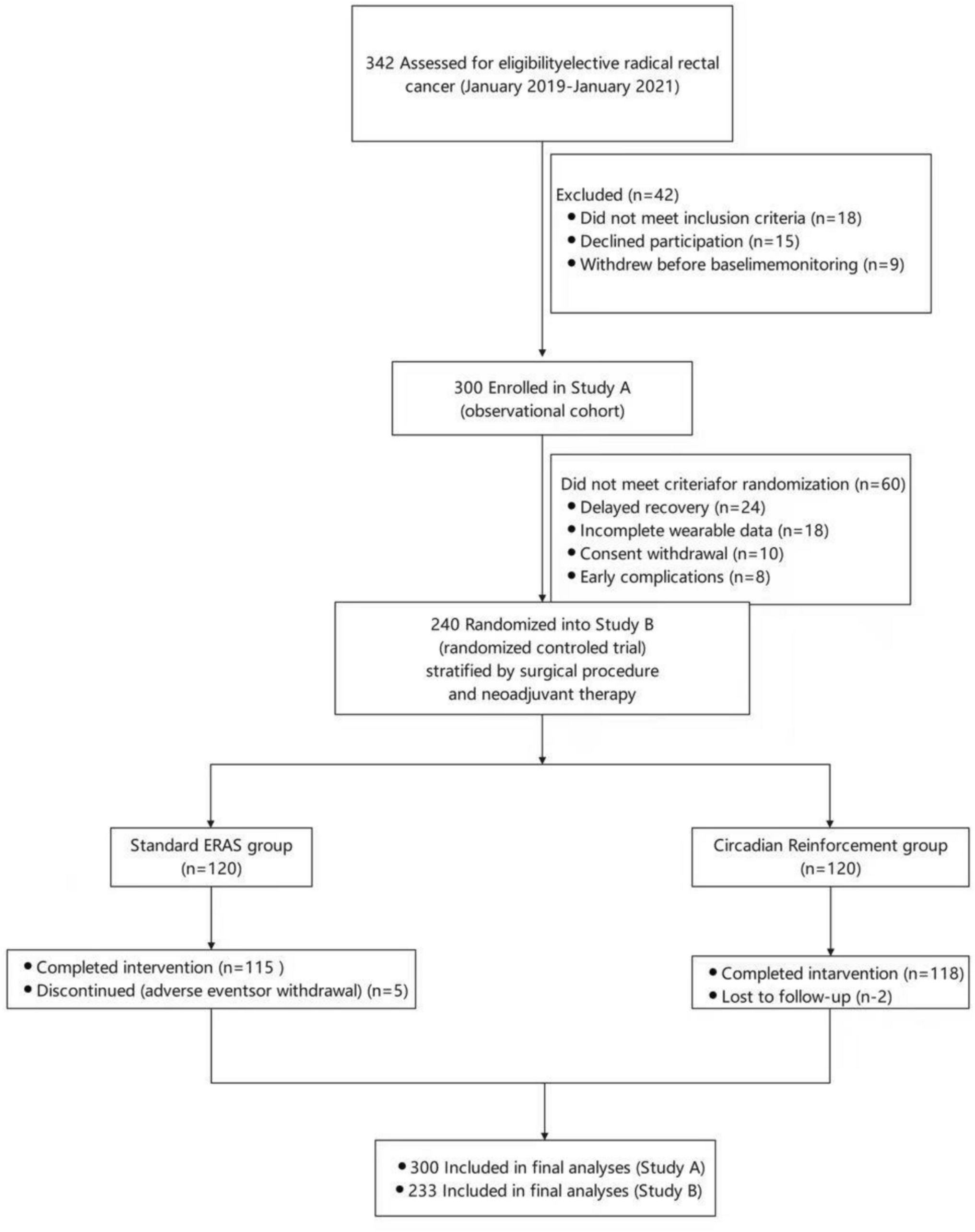


This is a retrospective review of prospectively collected data on patients who underwent G-POEM for the management of medically refractory gastroparesis at Allegheny Health Network hospitals (Pittsburgh, PA) between 2019 and 2024. Patients with at least 1 year of postoperative follow-up were included. Exclusion criteria were age under 18 years, prior pyloric drainage procedures, or anatomic abnormalities such as mechanical gastric outlet obstruction. This study was approved by the Institutional Review Board of Allegheny Health Network (IRB #2020–076).
Gastroparesis diagnosis and preoperative assessmentGastroparesis was diagnosed based on a comprehensive foregut evaluation incorporating both symptom characterization and objective diagnostic testing. All patients underwent a standardized workup that included gastric emptying scintigraphy (GES), completion of the Gastroparesis Cardinal Symptom Index (GCSI), and classification of disease etiology as diabetic, idiopathic, or postsurgical. Predominant symptoms such as nausea/vomiting, bloating, or early satiety were documented. Alternative diagnoses, including rumination syndrome, functional dyspepsia, superior mesenteric artery syndrome, and eating disorders, were excluded through clinical history, physical examination, and ancillary testing. Patients diagnosed with gastroparesis were initially managed with dietary modification and prokinetic therapy. Only those with persistent symptoms despite optimized medical management were considered for G-POEM.
GCSI assessmentThe GCSI is a validated patient-reported outcome measure assessing nine gastroparesis-related symptoms on a Likert scale from 0 (none) to 5 (very severe). The nausea/vomiting subscore reflects responses to nausea, retching, and vomiting; the early satiety subscore includes stomach fullness, inability to complete a normal meal, excessive fullness, and loss of appetite; and the bloating subscore includes bloating and visible distention. The total GCSI score was calculated as the mean of these three sub-scores, while the summed total score represented the aggregate of all nine symptom ratings. Both the predominant symptom and GCSI scores were recorded preoperatively and at postoperative follow-up.
Gastric emptying scintigraphy technique and interpretationGastric emptying scintigraphy (GES) was performed using a standardized radiolabeled solid meal containing 1 mCi of technetium 99 m sulfur colloid. Anterior and posterior planar images of the abdomen were obtained for 60 s immediately after ingestion and at hourly intervals over a 4-h period. The gastric region of interest was delineated, and radiotracer counts were measured at each time point. Attenuation-corrected counts were compared with baseline values to determine the percentage of meal retention. Delayed gastric emptying was defined as > 10% retention at 4 h, in accordance with established guidelines.
G‑POEM techniqueAll G-POEM procedures were performed under general anesthesia by a small group of high-volume foregut surgeons using a standardized technique. All attending surgeons had substantial prior experience with advanced endoscopic foregut interventions, including both esophageal POEM and G-POEM, and were proficient in submucosal tunneling and endoscopic myotomy techniques prior to adoption of the SBK. Clinical fellows were actively involved in all procedures. A submucosal cushion was created approximately 2–3 cm proximal to the pylorus along the lesser curvature using a saline and dye solution. A transverse mucosal incision was then made to initiate submucosal tunneling.
SBK groupThe SBK (Speedboat-RS2; Creo Medical Ltd., UK) is a novel bipolar endoscopic dissection tool specifically designed for submucosal tunneling and myotomy procedures. Compatible with a 3.7-mm working channel of a single-channel therapeutic endoscope, the device features a fully rotatable shaft, front and lateral cutting edges, and an insulated upper surface to allow precise dissection while minimizing thermal injury to underlying tissue. Its integrated 26-gauge needle allows for real-time submucosal injection and irrigation. The SBK delivers bipolar radiofrequency energy (400 kHz, 35 W) for cutting and microwave energy (5.8 GHz, 10 W) for coagulation, eliminating the need for instrument exchange during the procedure (Fig. 1). A newer, smaller profile version of the SBK is compatible with diagnostic endoscopes with a working channel ≥ 2.7 mm. This lower-profile device was not used in the present cohort.
Fig. 1
Design and functionality of the SBK system. A Schematic view of the distal end of an earlier-generation SBK illustrating the active bipolar cutting electrode, return electrode, integrated microwave antennas, and insulated shaft. B Lateral schematic view demonstrating the cutting edge, integrated injection needle, and protective hull designed to facilitate controlled submucosal dissection. C Representative images of two low-profile SBK variants compatible with diagnostic endoscopes. D The CROMA electrosurgical generator used to deliver bipolar radiofrequency energy for tissue cutting and microwave energy for coagulation during endoscopic procedures. Panels A and B are adapted from an open-access publication (New Kid on the Block: “Speedboat,” Journal of Digestive Endoscopy, 2022; CC BY-NC-ND 4.0), and panels C and D were provided courtesy of the manufacturer
During the procedure, the tip of the SBK was used to initiate a longitudinal mucosal incision, approximately 4 cm in length, along the lesser curvature. This was followed by downhill tunneling toward the pylorus, facilitated by the device’s rotatable body and protective hull, which provided both stability and depth control to avoid unintentional muscle injury. The full-thickness myotomy began just distal to the pyloric ring and was extended proximally into the antrum by approximately 1.5 cm. The bipolar blade enabled both forward and lateral muscle division, while microwave coagulation was applied selectively to submucosal vessels and for hemostasis throughout the dissection.
TTK groupIn the TTK group, the triangle-tip knife (Olympus, Tokyo, Japan) was used to perform the mucosotomy, submucosal tunneling, and pyloromyotomy. The TTK is a needle-type electrosurgical knife compatible with standard diagnostic endoscopes with a ≥ 2.7-mm working channel. The triangle-tip design enabled controlled and focused energy delivery for muscle division while minimizing mucosal injury. The TTK is a needle-type electrosurgical knife with a 4.5 mm cutting length, a 0.4 mm shaft diameter, and a triangular tip measuring 0.7 mm in radius and 0.4 mm in thickness. After mucosotomy, submucosal tunneling was carried out using TTK to reach the level of the pyloric ring. A selective full-thickness myotomy of the circular pyloric muscle fibers was then performed under direct endoscopic visualization using the same device.
In both groups, after completing the myotomy, the submucosal tunnel was irrigated, and the mucosal entry site was carefully inspected for serosal injury before being closed with endoscopic clips (Resolution™, Boston Scientific, Marlborough, MA). All patients underwent an upper gastrointestinal contrast study on postoperative day one to evaluate for contrast extravasation or obstruction.
Learning curve analysisTo assess the learning curve and identify the turning point where a significant improvement in operative efficiency occurred, we applied a change-point analysis based on operative time. First, procedures were ordered chronologically by date. Each procedure date was evaluated as a potential cut point to divide the series into two phases: an early phase (prior to the cut point) and a late phase (after the cut point). For each potential cut point, mean operative times between the two phases were compared using Student’s t test. The turning point was defined as the procedure date associated with the highest absolute t value, indicating the greatest difference in operative duration between early and late phases. The corresponding case number at this turning point was recorded as the estimated learning threshold. To visually represent the analysis, a graph was generated plotting the absolute t values against the cumulative case number, allowing for intuitive identification of the learning curve inflection point. Since procedures were performed by multiple surgeons within a training program, with fellows assisting or performing portions under supervision, the analysis reflects a center-wide learning pattern rather than that of individual operators.
Outcomes and statistical analysisBaseline demographic, procedural, and postoperative outcomes were compared between patients who underwent G-POEM using the TTK or the SBK for medically refractory gastroparesis. The primary outcome was technical success, defined as completion of the procedure without switching to an alternative knife. Secondary outcomes included operative efficiency (operative time and number of closure clips), perioperative and postoperative complications (perforation, pneumoperitoneum, and leak), and clinical outcomes including resolution of predominant symptoms, postoperative GCSI scores, 30- and 90-day length of hospital stay, and improvement in gastric emptying scintigraphy results. Preoperative and postoperative gastric emptying scintigraphy results were evaluated to assess improvement in gastric retention and normalization of gastric emptying. Values for continuous variables are presented as mean (standard deviation) or median with interquartile range, as appropriate. Categorical variables are reported as frequency and percentage. Comparisons between groups were performed using nonparametric tests, including the Mann–Whitney U test for continuous variables and Pearson’s chi-square test or Fisher’s exact test for categorical variables, as appropriate. A p value of < 0.05 was considered statistically significant. All statistical analyses were conducted using SAS software (version 9.4, SAS Institute, Cary, NC).
Comments (0)