This study demonstrated that urine culture-guided prophylactic antibiotic selection before ureteral stent removal was associated with a significantly lower risk of febrile pyelonephritis following radical cystectomy with ileal conduit urinary diversion.
Several aspects of surgical practice remain unclear, including the role of perioperative ureteral stenting in patients undergoing radical cystectomy with urinary diversion. Perioperative ureteral stenting is intended to prevent urinary leakage and reduce ureteroenteric anastomotic complications, which account for approximately 30% of postoperative morbidity [2, 11, 12]. However, ureteral stent placement or prolonged stent retention may increase the risk of UTI, potentially necessitating antibiotic treatment or prophylaxis and additional follow-up for stent removal [13].
Despite these concerns, the absence of consensus and high-quality evidence hinders definitive recommendations and the establishment of clear guidelines for interventions aimed at reducing infectious complications following radical cystectomy.
The American Urological Association guidelines on antimicrobial prophylaxis for urological surgery currently recommend a single preoperative dose of cefazolin for cystectomy when the small bowel is used for urinary diversion [14]. While antibiotic prophylaxis is recommended before bladder catheter removal in patients with risk factors, prophylactic antibiotic administration before ureteral stent removal is not recommended [15]. Conversely, the current EAU guidelines do not provide specific recommendations for antibiotic prophylaxis during or after cystectomy or at ureteral stent removal [8].
Furthermore, Parekh et al. [4] reported that the incidence of symptomatic UTIs following radical cystectomy was approximately 26% and 35% after open and robot-assisted surgery, respectively.
In contrast, Beano et al. [16] reported that after obtaining urine cultures from ureteral stents or urostomy bags and administering a single intravenous antibiotic dose tailored to the culture results, the UTI-related readmission rate within 90 days postoperatively increased from 6.6 to 18.6% in patients with negative and positive cultures, respectively. The incidence of urinary tract infections (UTIs) following radical cystectomy remains elevated, and the presence of bacteria within the urinary diversion appears to be a critical factor in postoperative UTI development. Consequently, prophylactic antibiotic strategies targeting these organisms may reduce UTI incidence after radical cystectomy. Nasu et al. [17] evaluated 50 patients who underwent radical cystectomy with intestinal urinary diversion. Among 43 patients for whom antibiotic selection was guided by urine cultures obtained from ureteral stents, only three (7%) developed febrile UTIs after ureteral stent removal, a significantly lower incidence than the 71% observed in patients whose antibiotic therapy was not culture-guided. Wang et al. [13] reported that urine cultures obtained from the ileal conduit on postoperative day 3 and from ureteral stent tips on postoperative day 7, followed by prophylactic antibiotic selection based on these results, reduced febrile UTI incidence from approximately 13.4% to 4.5%. Werntz et al. [18] reported that postoperative prophylactic oral trimethoprim–sulfamethoxazole (160/800 mg daily), nitrofurantoin (100 mg daily), or ciprofloxacin (250 mg daily) reduced the overall postoperative UTI rate from 36% to 12%. Furthermore, prophylactic antibiotic use decreased UTI incidence from 30 to 0% on the day after ureteral stent removal. Shigemura et al. [19] investigated patients who underwent radical cystectomy and received perioperative prophylaxis with tazobactam/piperacillin. Among patients with a positive preoperative urine culture (16 of 49), oral fluoroquinolones were administered 1–2 h before ureteral stent removal. Infectious complications occurred in only one of the 16 patients (6%) who received prophylactic antibiotics. Conversely, UTIs were observed in six of the 33 patients (18%) who did not receive prophylactic antibiotics at stent removal. However, a prospective study by Tobia et al. [20] reported limited concordance between perioperative intestinal or catheter cultures and pathogens identified during subsequent urinary tract infections after cystectomy with intestinal urinary diversion, suggesting that perioperative colonization may not reliably predict later infectious events.
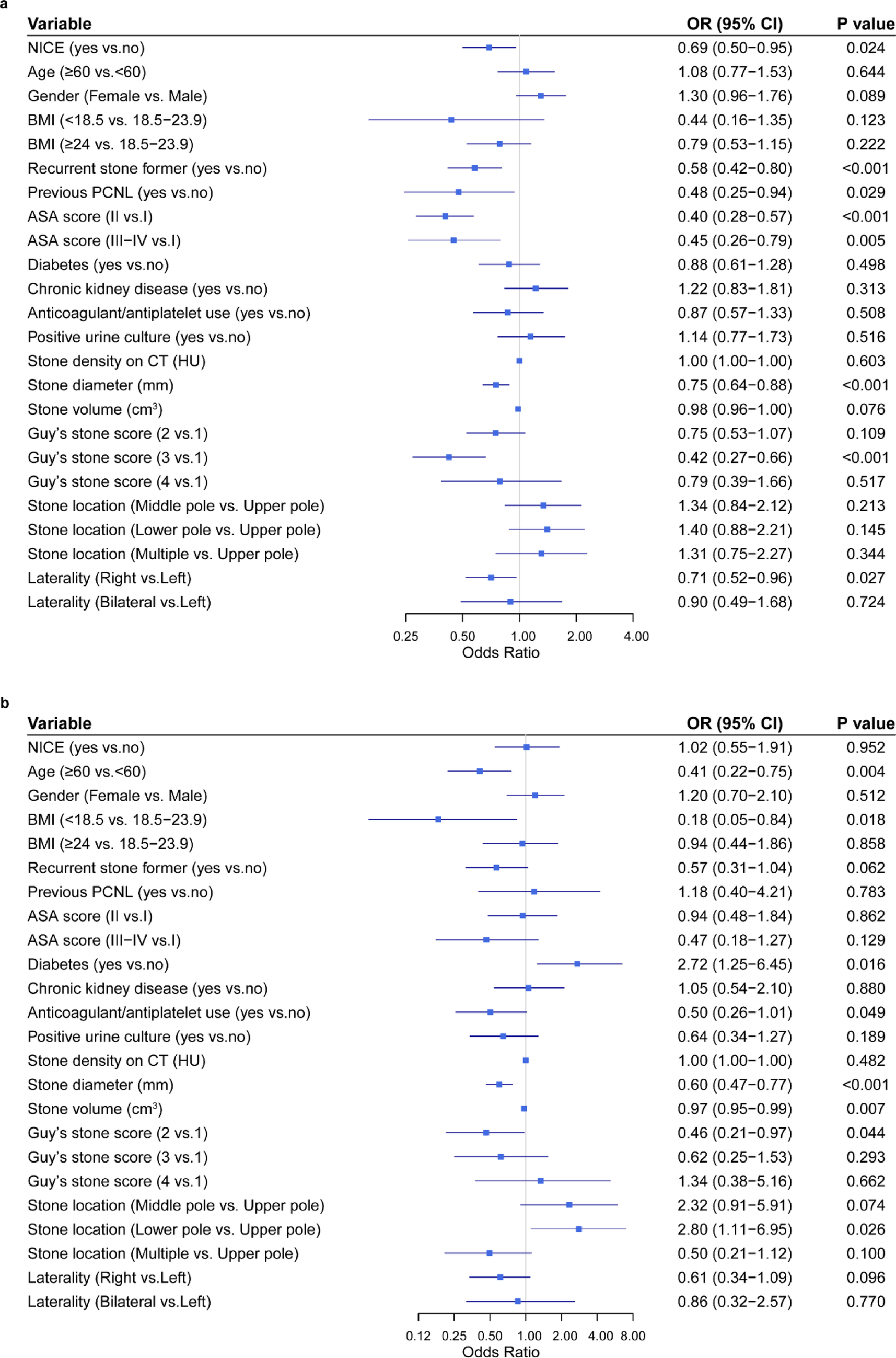
Nevertheless, previous studies suggest that prophylactic antibiotic administration at ureteral stent removal during urinary diversion after radical cystectomy may be associated with a reduced incidence of post-stent removal UTIs. However, prolonged antibiotic exposure is associated with an increased risk of multidrug-resistant organism emergence [21] and Clostridioides difficile infections [22]. Therefore, a strategy that targets a limited organism spectrum and uses short-duration prophylactic antibiotic therapy may better balance infection prevention with appropriate antimicrobial stewardship. In this context, our study demonstrated that identifying target organisms and administering narrow-spectrum antibiotics for approximately 2 days can effectively reduce the incidence of UTIs after ureteral stent removal. Moreover, the culture-guided strategy enabled short-course, narrow-spectrum prophylaxis, potentially reducing unnecessary antimicrobial exposure while aligning with current antimicrobial stewardship principles. Notably, the odds ratio for antithrombotic therapy differed between univariable and multivariable analyses. This change likely reflects confounding by perioperative factors included in the adjusted model rather than a direct causal relationship, and therefore should be interpreted with caution given the limited number of events.
Previous studies [5, 18] have reported that common causative pathogens of UTIs after radical cystectomy include Enterococcus spp., Escherichia coli, and Staphylococcus aureus. Moreover, polymicrobial infections have also been reported [23], consistent with our findings. In the present cohort, several frequently isolated organisms, including Enterococcus faecalis, Pseudomonas aeruginosa, Enterobacter cloacae, and Klebsiella pneumoniae, would generally be expected to be covered by fluoroquinolone-based empirical prophylaxis. However, other organisms such as Enterococcus faecium, MRSA, MRSE, and Corynebacterium striatum would not be reliably covered by such regimens and would require glycopeptide-based therapy. These microbiological differences may partly explain the potential benefit of culture-guided prophylaxis. When glycopeptide agents were selected, therapeutic drug monitoring was performed to ensure safety, and in a limited number of cases antibiotics were administered for approximately 72 h.
Total hospital costs tend to be higher for robot-assisted surgery than for open surgery and have been reported to be positively associated with a Charlson Comorbidity Index ≥ 2, the occurrence of complications, and increased length of hospital stay [24].
To the best of our knowledge, no previous study has specifically examined whether pyelonephritis alone affects total hospital costs, as evaluated in the present study. Because pyelonephritis was not associated with increased total hospital costs in our analysis, other postoperative complications may have contributed more substantially to overall hospital costs.




Comments (0)